w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Correlation
of
rheumatoid
arthritis
activity
indexes
(Disease
Activity
Score
28
measured
with
ESR
and
CRP,
Simplified
Disease
Activity
Index
and
Clinical
Disease
Activity
Index)
and
agreement
of
disease
activity
states
with
various
cut-off
points
in
a
Northeastern
Brazilian
population
Marta
Maria
das
Chagas
Medeiros
a,∗,
Brenda
Maria
Gurgel
Barreto
de
Oliveira
b,
João
Victor
Medeiros
de
Cerqueira
c,
Raquel
Telles
de
Souza
Quixadá
b,
Ídila
Mont’Alverne
Xavier
de
Oliveira
baFaculdadedeMedicina,UniversidadeFederaldoCeará,Fortaleza,CE,Brazil
bHospitalUniversitárioWalterCantídio,Fortaleza,CE,Brazil
cUniversidadedeFortaleza,Fortaleza,CE,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received20February2014 Accepted1December2014 Availableonline10March2015
Keywords:
Rheumatoidarthritis Diseaseactivity DAS28
Correlation Agreement
a
b
s
t
r
a
c
t
Introduction:TheDiseaseActivityScore28(DAS28)anditsversionshavebeenusedto
mea-surerheumatoidarthritisactivity,butthereisnoconsensusaboutwhichoneisthebest.
Objectives: Determinethecorrelationamongindexes(DAS28ESR,DAS28CRP,SDAIandCDAI)
andevaluateagreementofactivitystratausingdifferentcut-offpoints.
Methods:Rheumatoidarthritispatientswerecross-sectionallyevaluatedwithdata
collec-tiontocalculatetheDAS28(ESRandCRP),SDAIandCDAI,usingdifferentcut-offsfordefining remission,mild,moderateandhighactivity.Pearsoncorrelationswerecalculatedfor con-tinuousmeasuresandagreement(kappatest)forthestrata(remission,mild,moderateand highactivity).
Results:Of111patientsincluded,108werewomen,age55.6years,11-yeardiseaseduration.
DAS28(ESR)wassignificantlyhigherthanDAS28(CRP)(4.0vs.3.5;p<0.001)andthevalues remainedhigherafterstratificationbyage,gender,diseaseduration,rheumatoidfactorand HAQ.Correlationsamongindexesrangedfrom0.84to0.99,withbettercorrelationbetween SDAIandCDAI.Agreementsamongactivitystratarangedfrom46.8%to95.8%.DAS28(CRP) withcut-offpointfortheremissionof2.3underestimateddiseaseactivityby45.8% com-paredwithDAS28(ESR).SDAIandCDAIshowedagreementof95.8%.Thefourindexeswere associatedwithdiseasedurationandHAQ.
∗ Correspondingauthor.
E-mail:[email protected](M.M.C.Medeiros).
http://dx.doi.org/10.1016/j.rbre.2014.12.005
Conclusions: Althoughtheactivityindexesshowgoodcorrelation,theyshowdiscrepancies inactivitystrata,thusrequiringmoreresearchestodefineabetterindexandbettercut-off points.
©2015ElsevierEditoraLtda.Allrightsreserved.
Correlac¸ão
dos
índices
de
atividade
da
artrite
reumatoide
(Disease
Activity
Score
28
medidos
com
VHS,
PCR,
Simplified
Disease
Activity
Index
e
Clinical
Disease
Activity
Index)
e
concordância
dos
estados
de
atividade
da
doenc¸a
com
vários
pontos
de
corte
numa
populac¸ão
do
nordeste
brasileiro
Palavras-chave:
Artritereumatoide Atividadedoenc¸a DAS28
Correlac¸ão Concordância
r
e
s
u
m
o
Introduc¸ão: ODiseaseActivityScore28(DAS28)eversõestêmsidousadosparamedir
ativi-dadedaartritereumatoide(AR),masnãoexisteconsensosobrequaléomelhor.
Objetivos: Determinaracorrelac¸ãoentreosíndices(DAS28VHS,DAS28PCR,SDAIeCDAI)e
avaliaraconcordânciadosestratosdeatividadecomousodediferentespontosdecorte.
Métodos: PacientescomARforamavaliadostransversalmentecomcoletadedadospara
cálculodoDAS28(VHSePCR),SDAIeCDAI,comousodepontosdecortesdiferentespara definic¸ãoderemissão,atividadeleve,moderadaealta.Correlac¸õesdePearsonforam calcu-ladasparamedidascontínuaseconcordância(testedekappa)paraosestratos(remissão, atividadeleve,moderadaealta).
Resultados: De111pacientesincluídos,108forammulheres,médiade55,6anos,tempode
doenc¸ade11anos.DAS28(VHS)foisignificantementemaiordoqueDAS28(PCR)(4vs.3,5; p<0,001)eosvalorespermanecerammaioresapósestratificac¸ãoporidade,sexo,tempo doenc¸a,fatorreumatoideeHAQ.Correlac¸õesentreíndicesvariaramde0,84a0,99,com melhorcorrelac¸ãoentreSDAIeCDAI.Concordânciasentreestratosdeatividadevariaram de46,8%a95,8%.DAS28(PCR)compontodecortepararemissãode2,3subestimou ativi-dadedadoenc¸aem45,8%quandocomparadocomDAS28(VHS).SDAIeCDAIapresentaram concordânciade95,8%.Osquatroíndicesmostraramassociac¸ãocomtempodedoenc¸ae HAQ.
Conclusões:Emboraosíndicesdeatividadeapresentemboacorrelac¸ão,mostram
discrepân-ciasnosestratosdeatividade.Tornam-senecessáriosmaisestudosparadefinirmelhor índiceemelhorespontosdecorte.
©2015ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Themaingoalstobeachievedduringthetreatmentofpatients withrheumatoid arthritis(RA)are painreliefandthestrict controlofthejointinflammatoryprocess.Aimingathavinga moreadequateevaluationoftheinflammatoryactivityin clin-icaltrials,theAmericanCollegeofRheumatology(ACR),the EuropeanLeagueAgainstRheumatism(EULAR)andtheWorld Health Organization/InternationalLeagueAgainst Rheuma-tism(WHO/ILAR)proposedasetofvariables(coresets),which includedthenumberoftenderandswollenjoints, measure-ment ofpain, global assessmentof disease activity bythe physicianand patient,acute phasereactantandfunctional measure.1–3
In the early 90s another index to measure RA activity in clinical practice was proposed, and was called Disease Activity Score (DAS), which considers the number of ten-derandswollenjoints,erythrocytesedimentationrate(ESR) and assessmentperformed bythe patientof global health
orofdiseaseactivity.4ThisoriginalDASusesRitchie
articu-larindex(26joint regions)toassess thenumberofpainful joints, and 44 joints to evaluate the swollen ones. Later, the proposedDAS28started usingonly28joints for count-ingtheswollenandtenderjoints5andallowedtheoptional
use ofC-reactiveProtein(CRP)insteadofESRasan inflam-matory marker.6 Sincethen,DAS28was themostcommon
measureusedtoevaluatetheinflammatoryactivity,bothin clinical trials and in clinical practice. However, this index requires acomplexformulaincludingsquarerootof Nape-rianlogarithm,requiringatechnologytoolforitscalculation. Therefore, moresimple indexeswere later proposed: Sim-plified Disease Activity Index (SDAI)7 and Clinical Disease
ActivityIndex(CDAI).8SDAIisameasureproposedbySmolen
et al.,7 theresult ofwhichis thesimple sumofthe
Table1–Cut-offpointsofindexesDAS28,SDAI,andCDAItodefinestatesofdiseaseactivity.
Indexes Diseaseremission Mildactivity Moderateactivity Highactivity
OriginalDAS28(ESR)5 <2.6 2.6–3.2 >3.2–5.1 >5.1
DAS28(ESR)Aletahaetal.16 <2.4 2.4–3.6 >3.6–5.5 >5.5
DAS28(CRP)Inoueetal.17 <2.3 2.3–2.7 >2.7–4.1 >4.1
DAS28(CRP)Castrejónetal.18 <2.3 2.3–3.8 >3.8–4.9 >4.9
DAS28(CRP)Fujiwaraetal.11 <1.72 1.72–2.98 >2.98–4.77 >4.77
SDAI7 <3.3 3.3–11 >11–26 >26
CDAI8 <2.8 2.8–10 >10–22 >22
DAS28,Disease ActivityScore(28joints);SDAI,SimplifiedDiseaseActivityIndex;CDAI,ClinicalDiseaseActivityIndex;ESR,erythrocyte sedimentationrate;CRP,C-reactiveprotein.
takeCRPintoaccount,onlythefirstfourmeasures.Although indexesshow good correlation with each other,7–11 DAS28
isthe mostvalidated indexfor measuringdisease activity. AnotheradvantageisthatitispossibletousebothESRand CRPasaninflammatorymarker,butuseofthislattermarker stillrequiresfurtherstudy,sincediscrepanciesbetweenESR andCRPhavebeenreportedinsomepatientswithRA,with a trend toward higher values of ESR and lower values of CRP.12,13
Alltheseindexes(DAS28,SDAIandCDAI)measuredisease activity on acontinuous scale,and also allowcategorizing thepatient inactivitystrata, usingdifferentcut-off points: remission,mild,moderateandhighactivity.Withthe emer-genceofseveralnewdrugsinthelast15yearstotreatRA, diseaseremissionisagoalthatshallbesought.Theindexes cut-offpointsthatdefinediseaseremissionvaryinthe litera-ture.Forexample,theoriginalDAS28establishedthatclinical remissionwasdefinedwhenDAS28(ESR)was<2.6.5In2005,
Aletahaet al.proposedtolowerthecut-off pointto<2.4.14
Asto thebest cut-off point todefine remission when CRP isusedinthe calculationofDAS28, avaluebelow2.3was alreadysuggested.15,16In2013,FujiwaraandKita’sstudy
con-cludedthat thebest indextodefineclinical remissionwas DAS28measuredbyCRPwiththeconventionalcut-offof2.3 reducedto1.72.10Thecut-offpointsforotheractivitystrataof
thediseasealsovaryamongtheindexesandthiscanleadto inconsistencyintheclassificationofdiseaseactivity,resulting indifferentpractices,alsoaffectingthecomparisonofstudies whenusingdifferentcriteria.
Another very important point is that the possibility of patients’ethnicorigininfluencestheactivityindexes,making thegeneralizationofstudies’resultsinadequate.Differences ingeneticpolymorphismthatinfluencesCRPlevels,aswell asothergeneticandculturalfactorsofeachpopulation,can influencediseaseactivitymeasures,requiringthatstudieson thesubjectaredevelopedindifferentpopulationsto estab-lishthebestindex. Studiescomparingdifferentversionsof DAS28wereperformedpredominantlyinEuropeandAsiaand insomeAfrican-AmericanandblackAfricanpopulations.
Theobjectivesofthisstudyweretodetermineacorrelation amongthemostpopularindicatorsformeasuringactivityof rheumatoidarthritis(DAS28calculatedwithESR,DAS28 cal-culatedwithCRP,SDAIandCDAI)andassesstheagreementof diseaseactivitystatesdefinedbytheindexesusingdifferent cut-offpointsofDAS28inasampleofpatientsinnortheastern Brazil.
Methods
Patients withRAdiagnosis accordingtoACR criteria17who
werefollowedintheoutpatient’softheRheumatologyservice of the University Hospital Walter Cantidio at the Federal University ofCearáwere sequentiallyinvitedtoparticipate in the study.The presenceofother autoimmune diseases, except secondary Sjogren’ssyndrome, were excluded. The studydesignwascross-sectional.Datacollectiontookplace fromJanuarytoDecember2013.Demographicdata(gender, age,race,educationlevel),clinicaldatarelatedtoRA(disease durationsincediagnosis,presenceofextra-articular manifes-tations,rheumatoidfactor,medicationsused),werecollected frommedicalrecords.
Tocalculatetheactivityindexesofthedisease(DAS28,SDAI andCDAI),therheumatologistonthedayofconsultation col-lectedthefollowingdata:countofthenumberofpainfuland swollenjointsin28joints(shoulders,elbows,wrists, metacar-pophalangeal,proximalinterphalangeal,knees),globalhealth assessment(scale0–100)bythepatient,assessmentofdisease activity bythe patientand physician(0–10) and inflamma-toryactivitymarkerscarriedoutwithinamaximumperiod of 2 weeks before the consultation (ESR and CRP). If the patient’s condition had changed after the completion of inflammatory markers, these were not considered and a new assessment was scheduled. Patients with categorical CRPresults(positiveornegative;<or>)werenotconsidered forcalculation ofindexesthattake CRPinto account. Lab-oratory tests were performed at the Central Laboratory of HUWC and the methodsemployedwere:ESR(Sedi-System Automation)andCRP(immunoturbidimetryROCHECOBAS). DAS28 was calculated with software for specific calcula-tion ofDAS,using bothESRandCRP(mg/dl), globalhealth assessment bythe patient, and the number oftender and swollenjoints(28joints).SDAIwascalculatedbyaddingthe number of swollen joints (0–28), number of tender joints (0–28), evaluation of disease activity by the patient (0–10), evaluation ofdisease activity bythe doctor(0–10) and the value of CRP (0.1–10mg/dL). The result of the CDAI was thesumofthefourpreviousclinicalmeasurementswithout CRP.
Thecut-offpointsconsideredtodefinetheinflammatory activitystatesareshowninTable1.FortheDAS28calculated withESR,weusedthecut-offpointsoftheoriginalstudy5and
weusedthecut-offpointsproposedbyInoueetal.,15
Castre-jonetal.16 andFujiwaraetal.10 Thephysicalfunctionwas
assessedusingtheHealthAssessmentQuestionnaire(HAQ)18
withscoreof0–3,with0scoremeaningnolossofphysical function,3,fulldisability.
Statistics
PaireddataofcontinuousvariablesasDAS28(ESR)andDAS28 (CRP) and SDAI and CDAI were compared using paired t -test.Toestimatecorrelationbetweenthecontinuousvalues ofDAS28(ESR),DAS28(CRP),SDAI,CDAIandHAQPearson’s correlation coefficient was used. Tocompare the averages, Kruskal Wallis and Mann Whitney tests were used. The agreementbetweentheinflammatoryactivitystates (remis-sion,mild, moderate andhigh activity) wasdetermined by kappa test. The level of statistical significance was 0.05. Statisticalanalysis wasperformed usingSTATA version 9.0 software.
Results
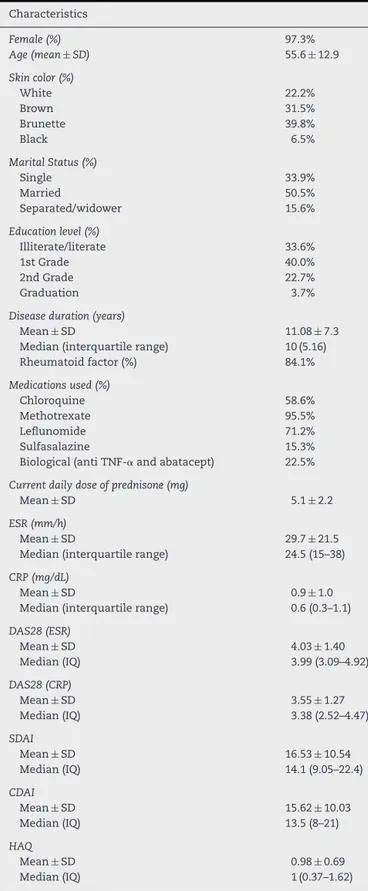
Atotalof111patientswere studied,predominantlyfemale (108womenand3men),mostofthemofwhite/brownrace (62%)withameanageof55.5years(SD=12.9)andduration ofdiseaseof11.08years(SD=7.3)(Table2).Rheumatoid fac-torwaspositivein84.1%ofthesampleandmostmadeuse ofmethotrexateand/orleflunomide(95.5%and 71.2%).The mean(±SD)and median(interquartilerange25–75) values ofDAS28(ESR),DAS28(CRP),SDAI,CDAI and HAQare also showninTable2.MeanDAS28(ESR)wasstatisticallyhigher thanmeanDAS28(CRP)(p<0.001)andalsothatofSDAIwas statisticallyhigherthan CDAI (p<0.001).The calculationof theindexesusingCRPwasdonewith96ofthe111patients because15patientsdidnotgettheproperdosageofCRP,only ofESR.
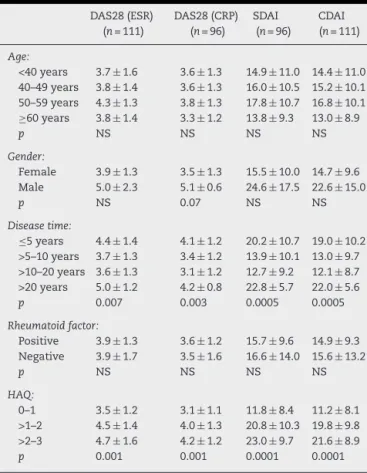
The mean DAS28 (ESR), DAS28 (CRP), SDAI and CDAI were also evaluated by age strata (<40, 40 to <50, 50 to <60 and ≥60 years), disease duration (≤5, >5–10, >10–20, >20 years), gender, rheumatoid factor (positive, negative), and HAQ(0–1,>1–2, >2–3)(Table3).Thevalues ofthe four activity indexes were statistically different for each stra-tum ofdisease duration, with the highest values after 20 years of disease, and then with ≤5 years of disease. The averagevalueswerealsosignificantlydifferentforHAQ stra-tum,withprogressivelyincreasingvaluesasHAQscorerange increased.
Correlations between DAS28 (ESR), DAS28 (CRP), SDAI and CDAI were all statistically significant (p<0.0001). Very strongcorrelations(>0.90)wereobservedamongDAS28(ESR) andDAS28(CRP)(0.92),DAS28(CRP)and SDAI(0.93),DAS28 (CRP) and CDAI (0.92) and between SDAI and CDAI (0.99). Strong correlations (between 0.6 and 0.9) were observed when comparing DAS28 (ESR) with SDAI and CDAI (0.84). Regularcorrelations(0.3–0.6)wereobservedcomparingHAQ withDAS28(ESR) (0.50),DAS28(CRP) (0.48),SDAI and CDAI (both0.53).
Whenindexeswere categorized byactivity strataofthe disease (remission, mild, moderate and high activity), the
Table2–Characteristicsofpatientswithrheumatoid arthritis.
Characteristics
Female(%) 97.3%
Age(mean ± SD) 55.6± 12.9
Skincolor(%)
White 22.2%
Brown 31.5%
Brunette 39.8%
Black 6.5%
MaritalStatus(%)
Single 33.9%
Married 50.5%
Separated/widower 15.6%
Educationlevel(%)
Illiterate/literate 33.6%
1stGrade 40.0%
2ndGrade 22.7%
Graduation 3.7%
Diseaseduration(years)
Mean± SD 11.08± 7.3 Median(interquartilerange) 10(5.16) Rheumatoidfactor(%) 84.1%
Medicationsused(%)
Chloroquine 58.6%
Methotrexate 95.5%
Leflunomide 71.2%
Sulfasalazine 15.3%
Biological(antiTNF-␣andabatacept) 22.5%
Currentdailydoseofprednisone(mg)
Mean± SD 5.1± 2.2
ESR(mm/h)
Mean± SD 29.7± 21.5 Median(interquartilerange) 24.5(15–38)
CRP(mg/dL)
Mean± SD 0.9± 1.0
Median(interquartilerange) 0.6(0.3–1.1)
DAS28(ESR)
Mean± SD 4.03± 1.40 Median(IQ) 3.99(3.09–4.92)
DAS28(CRP)
Mean± SD 3.55± 1.27 Median(IQ) 3.38(2.52–4.47)
SDAI
Mean± SD 16.53± 10.54 Median(IQ) 14.1(9.05–22.4)
CDAI
Mean± SD 15.62± 10.03 Median(IQ) 13.5(8–21)
HAQ
Mean± SD 0.98± 0.69 Median(IQ) 1(0.37–1.62)
ESR,erythrocytesedimentationrate;CRP,C-reactiveprotein;DAS28 (ESR),diseaseactivityscoreusingESR;DAS28(CRP),disease activ-ityscoreusingCRP;SDAI,SimplifiedDiseaseActivityIndex;CDAI, ClinicalDiseaseActivityIndex;HAQ,healthassessment question-naire.
Table3–Values(median±SD)ofDAS28(ESR),DAS28 (CRP),CDAIandSDAIbystrataofage,diseasetime, rheumatoidfactorandsex.
DAS28(ESR) (n=111)
DAS28(CRP) (n=96)
SDAI (n=96)
CDAI (n=111)
Age:
<40years 3.7± 1.6 3.6± 1.3 14.9± 11.0 14.4± 11.0 40–49years 3.8± 1.4 3.6± 1.3 16.0± 10.5 15.2± 10.1 50–59years 4.3± 1.3 3.8± 1.3 17.8± 10.7 16.8± 10.1 ≥60years 3.8± 1.4 3.3± 1.2 13.8± 9.3 13.0± 8.9
p NS NS NS NS
Gender:
Female 3.9± 1.3 3.5± 1.3 15.5± 10.0 14.7± 9.6 Male 5.0± 2.3 5.1± 0.6 24.6± 17.5 22.6± 15.0
p NS 0.07 NS NS
Diseasetime:
≤5years 4.4± 1.4 4.1± 1.2 20.2± 10.7 19.0± 10.2 >5–10years 3.7± 1.3 3.4± 1.2 13.9± 10.1 13.0± 9.7 >10–20years 3.6± 1.3 3.1± 1.2 12.7± 9.2 12.1± 8.7 >20years 5.0± 1.2 4.2± 0.8 22.8± 5.7 22.0± 5.6 p 0.007 0.003 0.0005 0.0005
Rheumatoidfactor:
Positive 3.9± 1.3 3.6± 1.2 15.7± 9.6 14.9± 9.3 Negative 3.9± 1.7 3.5± 1.6 16.6± 14.0 15.6± 13.2
p NS NS NS NS
HAQ:
0–1 3.5± 1.2 3.1± 1.1 11.8± 8.4 11.2± 8.1 >1–2 4.5± 1.4 4.0± 1.3 20.8± 10.3 19.8± 9.8 >2–3 4.7± 1.6 4.2± 1.2 23.0± 9.7 21.6± 8.9 p 0.001 0.001 0.0001 0.0001
ESR,erythrocytesedimentationrate;CRP,C-reactiveprotein;DAS28 (ESR),diseaseactivityscoreusingESR;DAS28(CRP),diseaseactivity scoreusingCRP;SDAI,SimplifiedDiseaseActivityIndex;CDAI, Clin-icalDiseaseActivityIndex;HAQ,healthassessmentquestionnaire.
proportionsofpatientsineachcategoryaccordingtothe cut-off points adoptedto calculate DAS28using ESR (original5
andAletaha14),ofDAS28usingCRP(Inoue,15Castrejón16and
Fujiwara10)andSDAIandCDAIarepresentedinTable4.
Reduc-ing the cut-off point from 2.6 to 2.4 in the calculation of DAS28(ESR)proposedbyAletahareducesthepercentageof patientsconsideredtobeinremissionfrom15.6%to13.5%. CalculatingtheDAS28withCRPandcut-offof2.3proposed byInoueandCastrejon,thepercentageofpatientsin remis-sioncategorizedasinremissionincreasesabout2.1%and4.2% comparedtooriginalDAS28criteria(ESR)andAletaha, respec-tively(Table4).Thereductionofthecut-offto1.72proposed byFujiwaramakesthiscriterionmorestringentfor consider-ingremissionbecauseitreducesfrom15.6%(DAS28ESR)to 6.3%inthiscategory.Ofalltheindexeswereanalyzedand presentedinTable4,thecut-offpointsofSDAIandCDAIto defineclinicalremissionarethemoststringent,reducingfrom 15.6%throughoriginalDAS28(ESR)calculationto4.2%.The absenceofCRPinthe calculationofCDAI doesnotchange anythingatallintermsofremissioncriteriawhencompared to the SDAI. The percentage of patients in the categories ofmildand moderateactivity hasgreater variationamong indexesthancategoriesattheextremes(remissionandhigh activity).
The agreements amongactivity strata(remission, mild, moderateandhighactivity)ofdifferentindexesandonusing differentcut-offpointsareshowninTable5.Thebest agree-ment of categories observed was between SDAI and CDAI (95.8%). Only one patient was in a lower category when CDAI definition was used. When original DAS28 (ESR) was compared with the original DAS28 (ESR) proposed by Ale-taha,agreementofactivity stratawasobservedin83.3%of patients (80/96) with 14 patients (14.6%) falling toa lower category(underestimatedactivity)whenusingAletaha crite-ria(Table6).WhenoriginalDAS28(ESR)wascomparedwith DAS28(CRP)byInoue,CastrejonandFujiwara,thebest agree-ment waswithFujiwaracriteria(67.7%).Thecut-off points suggestedbyCastrejónunderestimatedtheactivityinalmost halfofthepatients(45.8%),whilethosebyInoueandFujiwara underestimatedby16.6%.Theproportionsofoverestimated categoriesbyCastrejon,InoueandFujiwarawere,respectively, 7.3%,20.8%and14.6%.ComparingindexesthatuseCRPto cal-culatetheDAS28,thebestagreementwasthatbetweenwhat wasproposed byInoue andFujiwara(71.8%),withFujiwara overestimatingthestratain11patients(11.4%)and underes-timatingin16patients(16.7%).Theotheragreementsbetween multiple comparisons performed ranged from 46.8% to 67.7%.
Discussion
Withthegrowingandurgentneedforassessmentof rheuma-toid arthritis activity not only inclinical practice but also in the evaluation of efficacy of new treatments in clinical trials,itisincreasinglyimportanttohaveinstrumentsto mea-surediseaseactivityasaccuratelyaspossible.Someindexes have been proposed in recent decades; however, they still havepropertiesthatneedbettervalidation,sincetheywere testedinspecificpopulations.4–16 Therearetwomainways
tocomparetheratesbetweenthem:(1)ascontinuous meas-ures,comparing means and mediansinthe same patients and (2) as categorical measures (remission, mild, moder-ateandhighactivity)andcomparingtheagreementamong strata.
Inthepresentstudy,weanalyzedDAS28calculatedwith ESR and CRP, SDAI and CDAI as continuous variables, and alsocomparedthefourstratatoeachotheraccordingtothe criteriaoriginallyproposed5andmorerecentlybyAletaha14
for the calculation of DAS28 using ESR; the criteria were proposed for DAS28 using CRP according to three studies (Inoue,15 Castrejón16 and Fujiwara10) and SDAI and CDAI.
The firstobservation inthis study, corroborated byseveral otherstudies,8,13,16,19–21isthatthevaluesofDAS28withESR
are higher than the values of DAS28 by CRP, even when stratified byage groups, disease duration, rheumatoid fac-tor, gender and HAQ score. Therefore, the activity of the disease may be underestimated when using DAS28 with CRP instead of DAS28 with ESR. The excellent correlation between the indexes observed in our study was also reg-istered byother authors.13,15,21–23 Althoughthe correlation
Table4–Proportionofpatientsinremission,mild,moderateandhighactivityaccordingtothescoresofDAS28(ESR), DAS28(CRP),SDAIandCDAI.
Remission Mildactivity Moderateactivity Highactivity
OriginalDAS28(ESR) 15.6% 12.5% 50.0% 22.9%
DAS28(ESR)Aletahaetal. 13.5% 28.1% 36.5% 21.9%
DAS28(CRP)Inoueetal. 17.7% 13.5% 37.5% 31.3%
DAS28(CRP)Castrejónetal. 17.7% 43.7% 21.9% 16.7%
DAS28(CRP)Fujiwaraetal. 6.3% 30.2% 43.7% 19.8%
SDAI 4.2% 30.2% 48.9% 16.7%
CDAI 4.2% 31.3% 44.8% 19.7%
ESR,erythrocytesedimentationrate;CRP,C-reactiveprotein;DAS28(ESR),diseaseactivityscoreusingESR;DAS28(CRP),diseaseactivityscore usingCRP;SDAI,SimplifiedDiseaseActivityIndex;CDAI,ClinicalDiseaseActivityIndex.
Table5–ProportionsofagreementandkappacoefficientsamongDAS28(ESR),DAS28(CRP),SDAI,andCDAIbystrataof diseaseactivity.
Kappacoefficient Agreement
OriginalDAS28(ESR)vs.DAS28(ESR)Aletaha 0.76 83.3% OriginalDAS28(ESR)vs.DAS28(CRP)Inoue 0.46 62.5% DAS28(ESR)originalvs.DAS28(CRP)Castrejón 0.31 46.8% OriginalDAS28(ESR)vs.DAS28(CRP)Fujiwara 0.53 67.7%
OriginalDAS28(ESR)vs.SDAI 0.46 63.5%
OriginalDAS28(ESR)vs.CDAI 0.44 61.5%
DAS28(CRP)Inouevs.DAS28(CRP)Castrejón 0.42 55.2% DAS28(CRP)Inouevs.DAS28(CRP)Fujiwara 0.61 71.8%
DAS28(CRP)Inouevs.SDAI 0.38 56.2%
DAS28(CRP)Inouevs.CDAI 0.42 58.3%
DAS28(CRP)Castrejónvs.DAS28(CRP)Fujiwara 0.45 60.4%
DAS28(CRP)Castrejónvs.SDAI 0.38 55.2%
DAS28(CRP)Castrejónvs.CDAI 0.35 53.1%
SDAIvs.CDAI 0.93 95.8%
ESR,erythrocytesedimentationrate;CRP,C-reactiveprotein;DAS28(ESR),diseaseactivityscoreusingESR;DAS28(CRP),diseaseactivityscore usingCRP;SDAI,SimplifiedDiseaseActivityIndex;CDAI,ClinicalDiseaseActivityIndex.
rangedfrom46.8%to62,5%ofpatients.Therefore,an
excel-lentcorrelationdoesnotnecessarilymeangood agreement
betweenthecategoriesofactivity.For instance,thecriteria proposedbyCastrejónetal.underestimatethelevelof
activ-ity in almost half of the patients. The study by Tamhane
etal., comparingoriginalDAS28(ESR) withDAS28(CRP) by InoueandCastrejon,alsofoundanunderestimationof dis-easeactivity in40% ofpatients whenthe CRPwas used.13
Thiscanbeexplainedbyloweringofthecut-off pointand expansionoftherangeofmildactivityandreductionofthe
cut-offforhighactivity,causingagreaternumberofpatients to migrate from higher categories to lower ones. Impor-tantly,Castrejónetal.16 estimatedthesecut-off pointsina
population ofpatients withrecent-onsetRA(median dura-tionofdiseaseinthefirstvisit:6months;IQ3.6–9months). Thepopulationtestedinthisstudywasofpatientswith long-termRA(mean:11.08±7.3years;median:10years;IQ:5–16 years)andthestudybyTamhaneetal.13hadanaverageof
6.6±9.3years(median:1.8years;IQ:0.8–9.3).Whenwe cate-gorizethetimeofdiseaseingroups(≤5years,>5–10years;
Table6–AgreementbetweenoriginalDAS28(ESR)andDAS28(ESR)byAletahaetal.
Remission (Aletaha)
Mildactivity (Aletaha)
Moderateactivity (Aletaha)
Highactivity (Aletaha)
Totalpatients
Remission(original) 13 2 0 0 15
Mildactivity(original) 0 12 0 0 12
Moderateactivity(original) 0 13 34 0 47
Highactivity(original) 0 0 1 21 22
Total 13 27 35 21 96
>10–20yearsand >20 years)the averagevaluesofall eval-uated indexeswere statisticallydifferent, with the highest values at the extremes of age. We can conclude that the durationofdiseasecaninfluencethediseaseactivityindexes and therefore validation of a particular index should take thetimeofthediseaseintoconsideration.Thecut-offpoints proposed by Castrejon et al.16 may not apply to patients
withlong-termdisease.Thecut-offsofDAS28(CRP)byInoue and Fujiwara were established in a population ofpatients withlong-standing RA(about 10 years) and both underes-timatedthe level ofactivity in only16.6%when compared withoriginalDAS28(ESR),and overestimatedin20.8% and 14.6%,respectively.Analyzingtheseproperties,itappearsthat the reduction of all cut-off points for the four strata pro-posed by Fujiwara is closer to the original DAS28 criteria (ESR).
SDAIand CDAIcorrelated withDAS28(ESR)of0.84,and the firsttwo witheach other of 0.99.Inthe original study of SDAI the correlation with DAS28 (ESR) was 0.90.7
Sta-tistical validity excluding CRP from SDAI was very much tested in the original study of CDAI.8 In several analyses
madebetweenSDAIandCDAI,thevaluescorrelatedalmost perfectlyand the correlations between SDAI or CDAI with originalDAS28(ESR)rangedfrom0.87to0.90.AlthoughCRP showed no significant colinearity with other SDAI meas-ures, only 5% of the SDAI remained unexplained when it excludedCRP;inDAS28(ESR),ESRonlycontributedtoabout 15%.MeanCDAIvaluesareobviouslysmallerthantheSDAI, sincethevalueofCRPissuppressedinthecalculation.The degreesofagreementofthis study oforiginal DAS28(ESR) with the original SDAI and CDAI were low, but the agree-ment of SDAI with CDAI was almost perfect (95.8%). This highagreementreinforcesthattheexclusionofCRPforthe calculationofCDAIalmostdoesnotchangeanythinginthe assessmentofdiseaseactivitylevelcomparedtoSDAI.Only 4ofthe96 patientsanalyzed disagreedregardingthe stra-tum.
Definingapatientasinremissioncanmeanreductionor evenwithdrawal ofsome drugs in use and, therefore, the criteria shall prevent that a patient with residual activity ceasestobeproperlytreated(underestimationofactivity),and shallalsopreventthepatientfrombeingovertreated(activity overestimation).Thedefinitionofhighactivityisimportant, especiallyfordefiningtheintroductionofbiologicalagents, andalsoforprognosticreasons,sincetheprobabilityofmore rapidprogressionisgreater inpatients thatkeepthe high-estactivity.Thecategorizationofhighdiseaseactivitylevels isalsoanimportantfactorforeligibilityofpatientsin clini-caltrials.Comparingtheratestestedinthisstudy,themost rigorous for the categoryof remission are SDAI and CDAI. While15.6% ofthe patients studied were classified inthis stratumbyoriginalDAS28(ESR),only4.2%wereatthislevel bySDAI and CDAI. Thecut-off point usedby Fujiwara for the remission of1.72,well below the cut-off points ofthe other indexes, classified 6.3% of patients as in remission. Regardingthedefinitionofhighactivity,theindexcovering morepatientsinthisstratumwasDAS28(CRP)byInoue(31.3%) andthelowestnumberwasSDAIandDAS28(CRP)byCastrejon (16.7%).So,forthedefinitionofhighactivity,DAS28(CRP)by
Inouewasthemostsensitiveinthepopulationtestedinthis study.
Anotherinterestingfindingofthisstudyisthatthemean values of the four indexesstudied increased progressively withtheincreaseofHAQandwerestatisticallydifferent.This can be explained because the physical function can influ-encetheglobalhealthassessmentandactivitymadebythe patientanddoctor.TheHAQcorrelationswithindexeswere very similartootherstudies.7,9,14 Age,sexand rheumatoid
factor did not influence the values of the indexes stud-ied inthe presentstudy. Althoughthe meanvalues ofthe four indexes were all numerically higher in men than in women,justforDAS28(CRP)therewasatrendtoward statis-ticaldifference(p=0.07).Thesmallnumberofmalepatients mayhaveinfluencedthestatisticaloutcome.Someauthors suggest thatthecalculationofDAS28considersthegender and age,13,21 but this has not been established and
vali-dated.
Inshort,whiletheindexesDAS28(ESR),DAS28(CRP),SDAI and CDAI correlated well witheach other, theyhad many discrepancies regarding the categories/strata of inflamma-toryactivity.Regarding the calculationofDAS28, thevalue of disease activity as measured using CRP was underesti-matedcompared tothe measureusingESR. Therefore, the definition of remission and activity by a particular index maynothavethesamemeaningwhenmeasuredbyanother index.
Theactivity ofthe disease evaluated bySDAI andCDAI showed excellentcorrelationand agreement,stressingthat theCRPdosageisnotindispensableforactivityclinical assess-ment.Therefore,CDAIcanbeusedinsteadofSDAIbecauseits simplicityallowsitsuseatanytime,andanywhere.Another interestingfactisthatalltheindexesevaluatedinthestudy to measureRAactivity were associatedwithdisease dura-tionandfunctionalcapacity,factorsthatshouldbetakeninto accountintheassessmentofdiseaseactivityasmeasuredby theindexesstudied.
Thestudy has somelimitations:small samplesize, dif-ferent evaluators to count number of tender and swollen joints,andpatients’culturalandethnicbackground.Alarger samplesizewould leadtomorepatientsinthefour strata of activity according to the cut-off points analyzed, which would increase the power of conclusion ofthe study.The countofpainfulandswollenjointsmayshowlittlevariability whenmadebydifferentevaluators.Ideally,allpatientsshould bealwaysexaminedbythesameobserver,orthe examina-tiontechniqueshouldbestandardizedbytheevaluatorsand trainedpreviously.Patientsinthestudywerefromapublic institution oftertiary care, withlow socioeconomic status, loweducationandlong-standingdisease,characteristicsthat mayinfluencethedegreeofresponseofthecomponentsto calculate the activity indexes,including the assessmentof healthandactivitystatusmadebypatientsandcountingof painfuljoints.
mayinterferewiththeassessmentofdiseaseactivity. Mean-while,the choiceof indexto be used willdepend on: the objectiveofassessment(whetherforuseindailypracticeor inclinical trials),thedesiredgoal(remissionortherapeutic change),thepracticecontext(availabilityoftechnology, lab-oratorytests,time)andpersonalclinicianpreferences.When analyzingpublishedstudies,weshouldconsiderwhichindex andwhichcut-offpointwereusedforcomparison.Inclinical practice,thesameindexwiththesamecomponentsfor calcu-lationshouldalwaysbeconsistentlyusedtoallowlongitudinal comparisonsindecision-making.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. FelsonDT,AndersonJJ,BoersM,BombardierC,ChernoffM, FriedB,etal.TheAmericanCollegeofRheumatology preliminarycoresetofdiseaseactivitymeasuresfor rheumatoidarthritisclinicaltrials.TheCommitteeon OutcomeMeasuresinRheumatoidArthritisClinicalTrials. ArthritisRheum.1993;36:729–40.
2. SmolenJS.TheworkoftheEularStandingCommitteeon InternationalClinicalStudiesIncludingTherapeuticTrials.Br JRheumatol.1992;31:219–20.
3. BoersM,TugwellP,FelsonDT,VanRielPL,KirwanJR, EdmondsJP,etal.WorldHealthOrganizationand
InternationalLeagueofAssociationsforRheumatologycore endpointsforsymptommodifyingantirheumaticdrugsin rheumatoidarthritisclinicaltrials.JRheumatol.1994;41 Suppl:86–9.
4. PrevooML,Van’tHofMA,VanRielPL,TheunisseLA,Lubberts EW,VanLeeuwenMA,etal.Judgingdiseaseactivityinclinical practiceinrheumatoidarthritis:firststepinthedevelopment ofadiseaseactivityscore.AnnRheumDis.1990;49:
916–20.
5. PrevooML,Van’tHofMA,KuperHH,VanLeeuwenMA,Vande PutteLB,VanRielPL.Modifieddiseaseactivityscoresthat includetwenty-eight-jointcounts.Developmentand validationinaprospectivelongitudinalstudyofpatientswith rheumatoidarthritis.ArthritisRheum.1995;38:
44–8.
6. WellsG,BeckerJC,TengJ,DougadosM,SchiffM,SmolenJ, etal.Validationofthe28-jointDiseaseActivityScore(DAS28) andEuropeanLeagueAgainstRheumatismresponsecriteria basedonC-reactiveproteinagainstdiseaseprogressionin patientswithrheumatoidarthritis,andcomparisonwiththe DAS28basedonerythrocytesedimentationrate.AnnRheum Dis.2009;68:954–60.
7. SmolenJS,BreedveldFC,SchiffMH,KaldenJR,EmeryP,Eberl G,etal.ASimplifiedDiseaseActivityIndexforrheumatoid arthritisforuseinclinicalpractice.Rheumatology(Oxford). 2003;42:244–57.
8. AletahaD,NellVP,StammT,UffmannM,PflugbeilS,Machold K,etal.Acutephasereactantsaddlittletocompositedisease activityindicesforrheumatoidarthritis:validationofa clinicalactivityscore.ArthritisResTher.2005:R796–806.
9. AletahaD,SmolenJ.TheSimplifiedDiseaseActivityIndex (SDAI)andtheClinicalDiseaseActivityIndex(CDAI):areview
oftheirusefulnessandvalidityinrheumatoidarthritis.Clin ExpRheumatol.2005;23Suppl39:S100–8.
10.FujiwaraM,KitaY.Reexaminationoftheassessmentcriteria forrheumatoidarthritisdiseaseactivitybasedoncomparison oftheDiseaseActivityScore28withothersimpler
assessmentmethods.ModRheumatol.2013;23: 260–8.
11.SingH,GuptaV,RayS,KumarH,TalapatraP,KaurM,etal. Evaluationofdiseaseactivityinrheumatoidarthritisby RoutineAssessmentofPatientIndexData3(RAPID3)anditis correlationtoDiseaseActivityScore28(DAS28)andClinical DiseaseActivityIndex(CDAI):anIndianexperience.Clin Rheumatol.2012;31:1663–9.
12.RosaNetoNS,DeCarvalhoJF,ShoenfeldY.Screeningtestsfor inflammatoryactivity:applicationsinrheumatology.Mod Rheumatol.2009;19:469–77.
13.TamhaneA,ReddenDT,McGwinGJr,BrownEE,WestfallAO, ReynoldsRJ4th,etal.Comparisonofthediseaseactivity scoreusingerythrocytesedimentationrateandC-reactive proteininAfricanAmericanswithrheumatoidarthritis.J Rheumatol.2013;40:1812–22.
14.AletahaD,WardMM,MacholdKP,NellVPK,StammT,Smolen JS.Remissionandactivediseaseinrheumatoidarthritis Definingcriteriafordiseaseactivitystates.ArthritisRheum. 2005;52:2625–36.
15.InoueE,YamanakaH,HaraM,TomatsuT,KamataniN. ComparisonofDiseaseActivityScore(DAS)28-erythrocyte sedimentationrateandDAS28-C-reactiveproteinthreshold values.AnnRheumDis.2007;66:407–9.
16.CastrejónI,OrtizAM,ToledanoE,Casta ˜nedaS,Garcia-Vadillo A,PatinoE,etal.Estimatedcutoffpointsforthe28-joint diseaseactivityscorebasedonC-reactiveproteinina longitudinalregisterofearlyarthritis.JRheumatol. 2010;37:1439–43.
17.ArnettFC,EdworthySM,BlochDA,McShaneDJ,FriesJF, CooperNS,etal.TheAmericanRheumatismAssociation 1987revisedcriteriafortheclassificationofrheumatoid arthritis.ArthritisRheum.1988;31:315–24.
18.FerrazMB,OliveiraLM,AraujoPM,AtraE,TugwellP.
Crossculturalreabilityofthephysicalabilitydimensionofthe HealthAssessmentQuestionnaire.JRheumatol.
1990;17:813–7.
19.MatsuiT,KugaY,KanekoA,NishinoJ,EtoY,ChibaN,etal. DiseaseActivityScore28(DAS28)usingC-reactiveprotein underestimatesdiseaseactivityandoverestimatesEULAR responsecriteriacomparedwithDAS28usingerythrocyte sedimentationrateinalargeobservationalcohortof rheumatoidarthritispatientsinJapan.AnnRheumDis. 2007;66:1221–6.
20.BathonJM,MartinRW,FleischmannRM,BinghamCO, WhitmoreJB,EickenhorstT.DiseaseactivityscoresusingCRP versusESRandtherelationshipbetweenEULARandACR responsesinpatientswithearlyrheumatoidarthritis.Ann RheumDis.2005;64Suppl3:173[abstract].
21.HensorEM,EmeryP,BinghamSJ,ConaghanPG.Discrepancies incategorizingrheumatoidarthritispatientsbyDAS-28(ESR) andDAS28(CRP):cantheybereduced?Rheumatology. 2010;49:1521–9.
22.CrowsonCS,RahmanMU,MattesonEL.Whichmeasureof inflammationtouse?Acomparisonoferythrocyte sedimentationrateandC-reactiveproteinmeasurements fromrandomizedclinicaltrialsofgolimumabinrheumatoid arthritis.JRheumatol.2009;36:1606–10.