w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Incidence
and
prevalence
of
systemic
sclerosis
in
Campo
Grande,
State
of
Mato
Grosso
do
Sul,
Brazil
Alex
Magno
Coelho
Horimoto
a,b,c,∗,
Erica
Naomi
Naka
Matos
c,d,e,
Márcio
Reis
da
Costa
c,
Fernanda
Takahashi
e,f,
Marcelo
Cruz
Rezende
g,
Letícia
Barrios
Kanomata
h,
Elisangela
Possebon
Pradebon
Locatelli
e,
Leandro
Tavares
Finotti
c,e,
Flávia
Kamy
Maciel
Maegawa
a,
Rosa
Maria
Ribeiro
Rondon
i,
Natália
Pereira
Machado
c,f,j,
Flávia
Midori
Arakaki
Ayres
Tavares
do
Couto
f,
Túlia
Peixoto
Alves
de
Figueiredo
b,
Raphael
Antonio
Ovidio
k,
Izaias
Pereira
da
Costa
c,iaUniversidadeFederaldeMatoGrossodoSul(UFMS),CampoGrande,MS,Brazil
bHospitalRegionaldeMatoGrossodoSul,Servic¸odeReumatologia,CampoGrande,MS,Brazil
cUniversidadeFederaldeMatoGrossodoSul(UFMS),HospitalUniversitário,Servic¸odeReumatologia,CampoGrande,MS,Brazil dUniversidadedeBrasília(UnB),Brasília,DF,Brazil
ePrefeituraMunicipaldeCampoGrande,AmbulatóriodeEspecialidadesMédicas,CampoGrande,MS,Brazil
fUniversidadeAnhanguera(Uniderp),FaculdadedeMedicina,AmbulatóriodeEspecialidadesMédicas,CampoGrande,MS,Brazil gSantaCasadeCampoGrande,Servic¸odeReumatologia,CampoGrande,MS,Brazil
hCaixadeAssistênciaaosServidoresdoMatoGrossodoSul(CASSEMS),AmbulatóriodeEspecialidadesMédicas,Coxim,MS,Brazil iUniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
jUniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
kUniversidadeFederaldaGrandeDourados(UFGD),HospitalUniversitário,Servic¸odeReumatologia,Dourados,MS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received12October2015 Accepted2May2016
Availableonline15October2016
Keywords: Systemicsclerosis Scleroderma Incidence Prevalence Brazil
a
b
s
t
r
a
c
t
Introduction:Systemicsclerosisisanautoimmunediseasewhichshowsextreme hetero-geneityinitsclinicalpresentationandthatfollowsavariableandunpredictablecourse. Althoughsomediscrepanciesintheincidenceandprevalenceratesbetweengeographical regionsmayreflectmethodologicaldifferencesinthedefinitionandverificationofcases, theymayalsoreflecttruelocaldifferences.
Objectives: Todeterminetheprevalenceandincidenceofsystemicsclerosisinthecityof CampoGrande,statecapitalofMatoGrossodoSul(MS),Brazil,duringtheperiodfrom JanuarytoDecember2014.
Methods:AllhealthcareservicesofthecityofCampoGrande–MSwithattendinginthe spe-cialtyofRheumatologywereinvitedtoparticipateinthestudythroughastandardizedform ofclinicalandsocio-demographicassessment.Physiciansofanyspecialtycouldreporta suspectedcaseofsystemicsclerosis,butnecessarilythedefinitivediagnosisshouldbe estab-lishedbyarheumatologist,inordertowarrantthestandardizationofdiagnosticcriteria andexclusionofotherdiseasesresemblingsystemicsclerosis.Attheendofthestudy,
∗ Correspondingauthor.
E-mail:[email protected](A.M.Horimoto). http://dx.doi.org/10.1016/j.rbre.2016.09.005
15rheumatologistsreportedthattheyattendedpatientswithsystemicsclerosisandsent thecompletedformscontainingepidemiologicaldataofpatients.
Results:TheincidencerateofsystemicsclerosisinCampoGrandefortheyear2014was11.9 permillioninhabitantsandtheprevalenceratewas105.6permillioninhabitants.Systemic sclerosispatientsweremostlywomen,white,withameanageof50.58years,showingthe limitedformofthediseasewithameandurationofthediseaseof8.19years.Regarding laboratorytests,94.4%werepositiveforantinuclearantibody,41.6%foranti-centromere antibodyand19.1%foranti-Scl70;anti-RNAPolymeraseIIIwasperformedin37patients, with16.2%positive.
Conclusions: ThecityofCampoGrande,thestatecapitalofMS,presentedalower inci-dence/prevalenceofsystemicsclerosisincomparisonwiththosenumbersfoundinUS studiesandclosetoEuropeanstudies’data.
PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Incidência
e
prevalência
de
esclerose
sistêmica
em
Campo
Grande,
Estado
de
Mato
Grosso
do
Sul,
Brasil
Palavras-chave: Esclerosesistêmica Esclerodermia Incidência Prevalência Brasil
r
e
s
u
m
o
Introduc¸ão: Aesclerosesistêmica(ES)éumaenfermidadeautoimune,extremamente het-erogêneanasuaapresentac¸ãoclínicaesegueumcursovariáveleimprevisível.Embora algumasdiscrepânciasnastaxasdeincidênciaeprevalênciaentreregiõespossam refle-tirasdiferenc¸asmetodológicasnadefinic¸ãoeverificac¸ãodoscasos,elastambémpodem refletirasverdadeirasdiferenc¸aslocais.
Objetivos: ConheceraprevalênciaeincidênciadaESnacidadedeCampoGrande,capital doEstadodeMatoGrossodoSul(MS),Brasil,dejaneiroadezembrode2014.
Métodos: Todososservic¸osdesaúdedeCampoGrande(MS)quetinhamatendimentosna especialidadedereumatologiaforamconvidadosaparticipardoestudopormeiodeficha padronizadadeavaliac¸ãoclínicaesociodemográfica.Médicosdequalquerespecialidade poderiamreportarum casosuspeito deES,masobrigatoriamenteodiagnóstico defini-tivodeveriaserfeitoporumreumatologista,paragarantira padronizac¸ãodoscritérios diagnósticoseexcluiroutrasdoenc¸asqueseassemelhamàES.Nofimdoestudo15 reuma-tologistasrelataramteratendidopacientescomdiagnósticodeESeenviaramosformulários preenchidoscomosdadosepidemiológicosdospacientes.
Resultados: AtaxadeincidênciadeESemCampoGrandeem2014foide11,9por mil-hão/habitanteseadeprevalênciafoide105,6pormilhão/habitantes.Ospacientescom ESeramprincipalmentemulheres,dacorbranca,médiade50,58anos,formalimitadada doenc¸aetempodeevoluc¸ãomédiodadoenc¸ade8,19anos.Emrelac¸ãoaosexames lab-oratoriais,observou-seapositividadede94,4%paraoANA,41,6%paraACAe19,1%para anti-Scl70,oanticorpoanti-POL3foifeitoemapenas37 pacientes,compositividadede 16,2%.
Conclusões: AcapitaldoEstadodeMatoGrossodoSul,CampoGrande,apresentoudados de incidênciae prevalênciadeESinferioresaosencontradosem estudosamericanose próximosaosdadosobservadosemestudoseuropeus.
PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Systemic sclerosis (SSc) is an autoimmune disease of the connectivetissue,extremelyheterogeneousinitsclinical pre-sentation, with the involvement of multiple systems and that follows a varied and unpredictable course.1 Its etiol-ogyremainsunknown;amultifactorialcausewassuggested, possiblytriggeredbyenvironmentalfactorsinagenetically predisposedindividual.2
TheclassificationofSSc patientstakesinto accountthe extension of skin involvement and the presence of over-lapping with certain characteristics of other autoimmune rheumaticdiseases.3–5
casespermillioninhabitantsperyear.3Astudyina south-ernstateinAustraliareported anannualincidenceof22.8 newcasesofSScpermillioninhabitantsandaprevalenceof 233casesper millioninhabitantsin1999,withvalues sim-ilar to those in American studies conducted in the same period.6
Morerecently,asystematicreviewstudyreportedsimilar prevalencesofSScobservedintheUKandJapan,with31and 38casespermillioninhabitants,respectively.7Itisnoteworthy that,inadditiontoregionalgeneticvariations,environmental exposurescanalsohaveaneffectontheprevalenceand inci-dencerates.Forexample,silicaexposureappearstoincrease theriskofdevelopingSSc;however,thistriggeringactionis onlyimportanttoasmallproportionofmalepatients.7
Interestingly,therehasbeenanincreaseinSScincidence ratesindifferentgeographicalregions,6,8 possiblyduetoan earlierdiagnosisandalsototheuseofnewclassification crite-ria.Forexample,intheUnitedStates,theratefornewcases increasedfrom 0.6 casesper million in 1947in Tennessee to19.0casespermillion in1991inthe Detroitarea.9 Like-wise,theprevalenceandincidenceofSScappeartobelarger in populations of European ancestry, and lower in groups ofAsiandescent.7 InTaiwan,theincidenceandprevalence rateswere10.9and56.3casespermillioncases/inhabitants, respectively.10
In epidemiology studies of SSc, different results are observed in different regions of the world, and this also occursinonesamecountryorcity.6–8,10SScprevalencedata inamulti-ethnicFrenchdistrictsuggestedthatthedisease appearstobemorefrequentandsevere inapopulationof non-Europeanorigin,whichspeaksinfavoroftheideathat theracecouldinfluencethesusceptibilitytothedevelopment ofSSc,andalsotheclinicalprofile.11Inthis sameline,the EuropeangroupofSScresearchpointedoutthat geographi-calvariationsinpatientswithSScmayalsohaveaninfluence withregardtoantibodyassociationsandintherateof occur-renceamongwomenandmen,butnoassociationsbetween raceswerefound.12
Therearenopublisheddataontheprevalenceand inci-dence of SSc in the Brazilian population, since this is a rarecondition.Thus,duetothescarcityofnationalstudies andthehighdegreeofmiscegenationfoundintheBrazilian population13weaimedtostudytheprevalenceandincidence ofsystemicsclerosisinthecityofCampoGrande,thestate capitalofMatoGrossodoSul,Brazil,duringtheperiodfrom JanuarytoDecember2014.
Objectives
Todeterminetheprevalenceandincidenceofsystemic scle-rosisinthecityofCampoGrande,MatoGrossodoSul,Brazil, duringtheperiodfromJanuarytoDecember2014.
Methods
AllhealthcareservicesinCampoGrande–MSwith Rheuma-tologyspecialtyparticipatedinthisprospectiveobservational study.
TheRheumatologyunitsinthecityaredistributedamong theMedicalSchoolTeachingHospitaloftheUniversidade Fed-eral de MatoGrosso doSul,the Regional Hospital ofMato GrossodoSul,SantaCasadeCampoGrande,theoutpatient clinicoftheMedicalSpecialtiesCenteroftheMunicipalityof CampoGrande,outpatientclinicsoftheMedicalSpecialties Center ofAnhanguera-UniderpMedicineSchool,outpatient clinics ofthe Caixade AssistênciadosServidoresde Mato GrossodoSul,andseveralprivateRheumatologyclinics.
Prior to starting this study, all rheumatologists were informed by e-mail and phone call about the procedures for data collection and objectives ofthis research. Period-ically, we asked (by e-mail or phone call) to all involved doctorstocompleteastandardizedformforcollecting demo-graphic and laboratory dataof all patients diagnosedwith systemic sclerosis and evaluated during the study period, regardlessofwhethertheywereneworoldcases.Any doc-torcouldreportasuspectedcaseofSSc(generalpractitioner, dermatologist, vascularsurgeon, gastroenterologist, pulmo-nologist,etc.),butthedefinitivediagnosisnecessarilyshould beestablishedbyarheumatologist,inordertoensurethe stan-dardizationofdiagnosticcriteriaandtoruleoutotherdiseases resemblingSSc,forexample,mixedconnectivetissuedisease (MCTD).
At the end of the study, 15 rheumatologists reported patients withSSc,andsent thecompletedformswith epi-demiologicaldataoftheirpatients;verbalorwrittenconsent from all patientswas requested.Thereasons forother MS rheumatologistsdidnotreportcaseswere:theydidnot exam-inepatientswithSScintheperiod,orthepatientsseendidnot liveinCampoGrande–MSorthepatientshadalreadybeen reportedbyanothercolleague(patient’s duplicity).Toavoid dataredundancyintheeventthatanindividualpatienthad beenassessedbymorethanarheumatologist,thesepatients wereidentifiedbytheinitialsoftheirnamesandtheirdateof birth.
PatientsdiagnosedwithSScandnon-residentsofCampo Grande–MSwerenotconsideredforincidenceandprevalence estimates.
Tobeselected,patientswithSScshouldmeetthefollowing criteria:
- Meetthe2013classificationcriteriaoftheACR/EULARfor SSc14;
- Inthecaseofabsenceofskinthickening,patientsshould meetthe2001criteriaofLeRoyandMedsgerforearlySSc.15
Stateoforigin,provenance,age,genderandrace/colordata, andtimeelapsedfromfirstsymptomstodiagnosis,disease duration, and clinical formofSSc were collected,and lab-oratory tests suchasantinuclear antibody(ANA) anti-DNA topoisomerase I antibody(antiScl70), anticentromere anti-body(ACA)andanti-RNApolymeraseIII(anti-RNAPIII)also wereconducted.
Themethodsusedinautoantibodysurveywere, respec-tively:
a. Antinuclearantibodies(ANA)survey
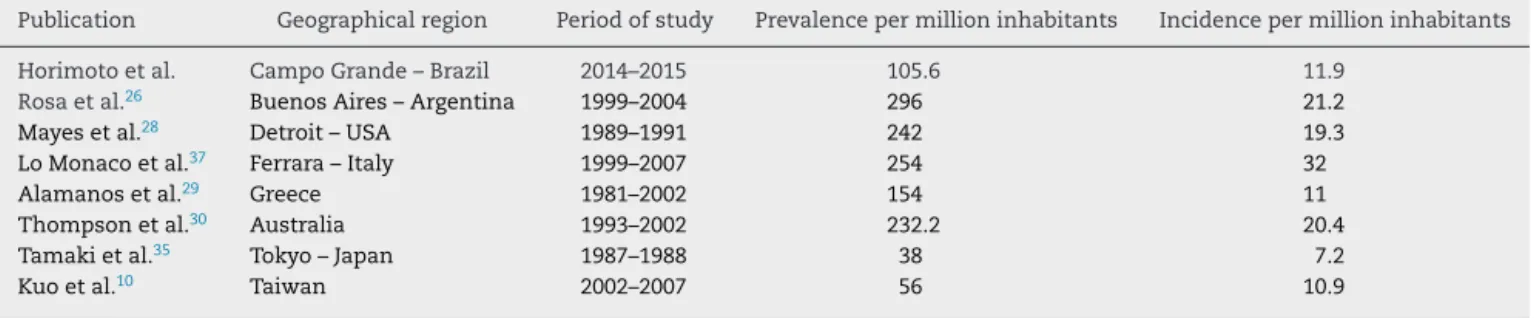
Table1–Comparisonofincidenceandprevalenceratesofpatientswithsystemicsclerosis(SSc)inseveralgeographical regions.
Publication Geographicalregion Periodofstudy Prevalencepermillioninhabitants Incidencepermillioninhabitants
Horimotoetal. CampoGrande–Brazil 2014–2015 105.6 11.9
Rosaetal.26 BuenosAires–Argentina 1999–2004 296 21.2
Mayesetal.28 Detroit–USA 1989–1991 242 19.3
LoMonacoetal.37 Ferrara–Italy 1999–2007 254 32
Alamanosetal.29 Greece 1981–2002 154 11
Thompsonetal.30 Australia 1993–2002 232.2 20.4
Tamakietal.35 Tokyo–Japan 1987–1988 38 7.2
Kuoetal.10 Taiwan 2002–2007 56 10.9
Theresultsareshowninnumberofcasespermillioninhabitantsperyear.
BrazilianConsensusonAntinuclearFactorinHep-2cells (2003)criteria16fortheinterpretationofresults.
Serawereconsideredpositivewithatiter≥1/160,with dilu-tionanegativefluorescence.
b. Anticentromere survey – Indirect immunofluorescence techniquewithHEp2cellsasasubstrate,accordingtothe IIBrazilianConsensusonAntinuclearFactorinHep-2cells (2003)criteria16fortheinterpretationofresults.
c. Anti-DNAtopoisomeraseI(antiScl70)survey– Immunoas-say technique17;thesamplewasconsiderednonreactive withvalues<20units,weaklyreactivebetween20and39 units, moderatelyreactive between40and 80 unitsand stronglyreactive(highervalues)withvalues>80units. d. Anti-RNA polymerase III Antibody survey – ELISA
technique18; the sample was considered negative with values<20units,weaklyreactivebetween20and39units, moderatelyreactivebetween40and80units,andstrongly reactive(highervalues)with>80units.
Statistical
analysis
IBGEdata19withestimatesoftheresidentpopulationinBrazil andinUnitsoftheFederationandwithareferencedateofJuly 1,2014,wereconsideredforthecalculationoftheincidence andprevalenceofSSc.
Data is presented in absolute and relative frequencies, meansandstandarddeviations,andwithaconfidence inter-valof95%andstatisticallysignificantvaluesforp<0.05.
Results
During2014,atotalof166patientswithsclerodermaor sys-temicsclerosisweretreatedinvariousoutpatientclinicsand RheumatologyUnitsinthecityofCampoGrande–MS. Eighty-ninepatientswholivedinthecityhadadefinitivediagnosis ofsystemicsclerosisandwereclinicallyexaminedinthatcity duringthestudyperiod.
Ofthistotal,10werenewcasesofSScdiagnosedduring the year2014and 79 patientshad already been previously diagnosed.Therefore,theincidencerateofSScinthecityof CampoGrande–MSduringtheyear2014was11.9per mil-lioninhabitantsandtheprevalenceratewas105.6permillion
inhabitants. Thedataare presentedin Table1, whichalso listscomparisonswithincidenceandprevalenceratesinother countriesandregions.
Resultsobservedinsystemicsclerosis
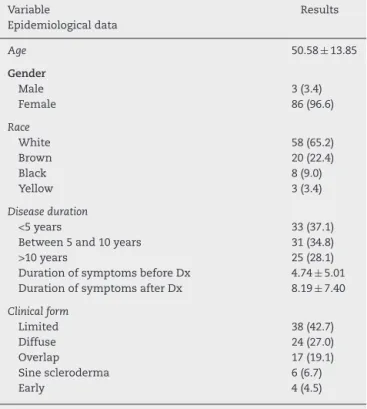
Amongthe89patientswithSSc,86werewomen(96.6%)and 3 were men (3.4%) with a mean age of 50.58±13.85 years (mean±standarddeviation).
Thirty-onepatients(34.8%)withSScwereborninthecityof CampoGrande;31patients(34.8%)wereborninthe country-sideofMT,and27patients(30.4%)wereborninotherstates.
Ofthe89patientswithSSc,58patients(65.2%)reported beingwhite,20patients(22.4%)hadabrowncolor,8patients (9.0%)wereblackand3patientsyellow(3.4%).
Regarding clinical forms of SSc, 38 patients (42.7%) showed the limitedform, 24patients (27.0%)exhibited the diffuse form, 17 patients (19.1%) show overlapping with other collagen diseases, 6 patients (6.7%) exhibited the sine scleroderma form and 4 patients (4.5%) had the early form. Among the 17 patients with the overlapped form, 8 patients (47.1%) concomitantly had systemic lupus erythe-matosus,5patients(29.4%)hadrheumatoidarthritis,and4 patients(23.5%)hadtheirSScassociatedwithinflammatory myopathies.
PatientswithSScwerealreadypresentingsymptomsfor 4.74±5.01yearsbeforetheirdiagnosis,andthedisease dura-tion,ingeneral,wasabout8.19±7.40years.
ANAwaspositivein84patientswithSSc(94.4%),andthe main patterns found inthese patients were: fine speckled nuclearpattern(30patients–36.6%),centromericpattern(29 patients – 35.4%) and quasi-homogeneousnuclear pattern, withmetaphaseplatestainingfor5–10points(12patients– 14.6%). Amongall patients,37 (41.6%)hadpositiveACA,17 (19.1%)werepositiveforanti-Scl70and1patient(1.1%)was simultaneouslypositiveforbothautoantibodies.Ontheother hand,theanti-RNAPIII wasperformedinonly37 patients, beingpositivein6ofthese(16.22%).
Table2–Distributionofpatientsevaluatedinthisstudy andresultsofepidemiologicaldatainpatientswith systemicsclerosis(SSc).
Variable Results
Epidemiologicaldata
Age 50.58±13.85
Gender
Male 3(3.4)
Female 86(96.6)
Race
White 58(65.2)
Brown 20(22.4)
Black 8(9.0)
Yellow 3(3.4)
Diseaseduration
<5years 33(37.1)
Between5and10years 31(34.8)
>10years 25(28.1)
DurationofsymptomsbeforeDx 4.74±5.01
DurationofsymptomsafterDx 8.19±7.40
Clinicalform
Limited 38(42.7)
Diffuse 24(27.0)
Overlap 17(19.1)
Sinescleroderma 6(6.7)
Early 4(4.5)
Dx,diagnosis.
Theresultsarepresentedasmean±standarddeviationoras abso-lutefrequency(relativefrequency).
Table3–Resultsofautoantibodiesinpatientswith systemicsclerosis(SSc).
Variable Results
ANA
Positive 84(94.4)
Negative 5(5.6)
ANApattern(n=84)
Nuclearfinespeckled 30(35.7)
Centromeric 29(34.5)
Nuclearquasihomogeneous 12(14.3)
Others 13(15.5)
Anti-Scl70
Positive 17(19.1)
Negative 72(80.9)
ACA
Positive 37(41.6)
Negative 52(58.4)
anti-RNAPIII(n=37)
Positive 6(16.2)
Negative 31(83.8)
ANA,antinuclearantibody;Scl70,anti-DNAtopoisomeraseI anti-body; ACA, anti-centromere antibody; anti-RNAP III, anti-RNA polymeraseIIIantibody.
Theresultsarepresentedinabsolutefrequency(relativefrequency).
Discussion
Inthis study,anunprecedentedand representativesample
oftheMidwestofBrazilwasdefined,havingbeen
character-izedbyaheterogeneousgroupofpatientswithvariousspectra
ofdiseaseanddifferentstagesofclinicalmanifestationsand
activitiesofthedisease,butthatisverysimilartowhatoccurs
inotherpopulationsofpatientsinthiscountryandevenfrom
otherlocations.3,13,20–23
Asystematicreviewof32articlespublishedfrom1969to 2006indicatedthattheincidencerateforSScvariedfrom0.6 to122casespermillioninhabitants;ontheotherhand,the prevalencerate forthesame disease rangedfrom 7to489 casespermillioninhabitants,9whichisconsistentwiththe ratesobservedinourstudy.Severalgeographicalvariations wereobserved,withahigherprevalenceofSScintheUnited States(276casespermillioninhabitants)andAustralia(233 casespermillioninhabitants)versusJapanandEurope,where onestillobservedanorth–southvariablegradient,withlower prevalenceratesinnorthernEuropeancountries.9,12
TheratesfoundforSScinourstudy(incidenceof11.9per millioninhabitantsandprevalenceof105.6permillion inha-bitants)aremoresimilartothoseforEuropeancountries.For example,theprevalenceofSScinaFrenchmulti-ethnic dis-trictwas158.3casespermillioninhabitantsin200111;inthe northofEnglandaprevalenceof88.0casespermillion inha-bitantsin2000wasfound.24ApeculiarityofthecityofCampo Grande–MSisthatitspopulationwasmainlycomposedof nationalimmigrantsandforeigners,whocamemainlyfrom thestatesofMinasGerais,RioGrandedoSul,Parana,andSao Paulo,and fromcountrieslikeGermany,Spain,Italy,Japan, Paraguay,Portugal,SyriaandLebanon.25
There are no Brazilian studies published on the inci-denceorprevalenceofSSc.InSouthAmerica,theincidence andprevalenceofSScobservedinBuenosAires–Argentina were 21.2 cases and 296 cases per million inhabitants, respectively.26 In the Caribbean, a lower incidence was observed, with a total of 17 cases of SSc observed in the Afro-descendantpopulationofBarbadosduringan observa-tionperiodof10years(1996–2006).27InNorthAmerica,the incidenceandprevalenceofSScobservedintheUnitedStates were higher, respectively 19.3 and 242.0 cases per million inhabitants.28
Althoughsomediscrepanciesintheincidenceand preva-lence of SSc between regions may reflect methodological differences inthe definition and verificationof cases,they canalsoreflecttruelocaldifferences.Theseregional differ-encescouldoccurduetothediversegeneticsusceptibilityto thedevelopmentofSSc,ortodifferentdegreesofexposureto environmentalfactorsincriminatedinthepathogenesis.6
(BarbadosandPuertoRico),theratesarerespectively26:127 and23:133;inNorthAmerica(USandCanada),theratesare respectively6.1:18and7.6:134;inAsia(TaiwanandJapan),the ratesare respectively 3.5:110 and 14:135; intheMiddle East (Iraq),therateis8.3:136;andinEurope(Italy,Germany,France andEngland),theratesarerespectively9.7:1,375:1,2111.5:1,11 and5.2:1.24
Regarding other demographic data found, the mean age of our patients with SSc (50.5 years) was almost consensus among the various studies in Brazil and overseas,6,11,13,20–24,28–31,33,34,36,37 with the diagnosis estab-lishedbetweenthefourthandfifthdecadesoflife;onlythe African-Caribbeanpopulation27 hadayoungermeanageat diagnosis (37.3years). Withregardto theraceinformed by the patient, there was a prevalence of white color in our patientswithSSc;however,onedonotrulesoutthe possi-bilityofabiasofracialclassification,duetothehighdegree ofmiscegenationfoundintheBrazilianpopulation.13Inthe South20 andSoutheast23 ofthiscountry,therewasahigher prevalenceofwhitepeoplewithSSc.Ontheotherhand,inthe Northeast38region,ahighprevalenceofmulattoesandblacks was observed, probably because the study was conducted inastatewithaknownpredominanceofAfro-descendants (Bahia).
In this same vein, the European researchgroup on SSc (EUSTAR)pointedoutthatgeographicalvariationsinpatients withSScmay alsohaveanimpactwithregardtoantibody associationsandintherateofoccurrencebetweenwomen andmen,12butthis,aswellasanotherstudy,foundno asso-ciationbetweenraces.12,39 Inthisstudy,mostpatientswith SScwereborninthesamestate(73.4%),andtheremaining patientswerefromdifferentlocations,butmainlyfromthe statesofSãoPaulo(13.44%)andParaná(5.04%).
In this study, the limited clinical presentation of SSc showedaslightpredominanceofthediffuseform,in accor-dance with other descriptions in the country13,20,23,37 and inmostotherpopulations.11,21,22,24,28,33,36However,thereare descriptionsinwhichthediffuseformismorecommon in populationsofBlacksvs.Caucasianpopulations,11,28,38 includ-ing,inthiscase,thoseofAfrican-Caribbeandescent,inwhich apredominanceofdiffuse(63%)overthelimited(37%)form wasobserved.27
Regardingthelaboratorytestsperformedinpatientswith SSc, antinuclear antibody (ANA) was present in 94.4% of patients–asimilar resulttomostnationalstudies13,20,23,37 and in other regions.11,21,28,36,40–42 The main patterns observedwere:finespecklednuclear,centromeric,and quasi-homogeneous nuclear patterns. Bernstein et al. described ANA positivity in 97% of patients with SSc, mainly repre-sentedbyfinespeckledandcentromericpatterns,besidesthe observationofanassociationwiththenucleolar(speckledand homogenous)patternin33%ofpatients.42Hesselstrandetal. reportedANApositivityin84%ofpatientswithSSc,andthe mostobservedpatterns were:finespeckled(41%), homoge-neous(25%),nucleolar(24%)andcentromeric(18%)patterns.40 RegardingspecificantibodiesforSScobservedinthisstudy, anti-centromere(ACA),anti-DNAtopoisomeraseI(antiScl70) and anti-RNA polymerase III (anti-RNAP III) positivity was observedin41.6%,19.1%and16.2%ofpatients,respectively, andthepercentageswerecomparabletothoseintwostudies
conductedinSouthernBrazil,13,20althoughMülleretal.had foundsurprisinglyhighlevelsofanti-RNAPIII(41.18%).20In thisstudy,60of89patients(67.4%)werepositiveforatleast oneofthosethreespecificautoantibodiestoSSc(anti-Scl70, ACA,oranti-RNAPIII).
Theliteraturereportsthattheprevalenceofhighlyspecific autoantibodiesassociatedwithSScorwithoverlapsyndromes withSSCfeaturesishighinpatientswithSSc,primarily repre-sentedbyACAandantiScl70,40–42hereincludingtheBrazilian population with SSc.13,20 Although the studies report that the coexistence of these specific autoantibodies is rare in patientswithSSc(1.6%),40–42 inthisstudy,weobservedtwo patients(2.2%)thatwereconcomitantlypositiveforspecific autoantibodies:onepatientwiththediffuseformpresented concomitant positivityforantiScl70 andACA,and another patientalsowiththediffuseformhadconcomitantpositivity forantiScl70andanti-RNAPIII.
Our conclusion is that the city of Campo Grande, the state capital of MatoGrosso do Sul, presented lower inci-denceandprevalenceofSScversusthosefoundinAmerican studies and similar to those observed in European stud-ies. This incidence, however, may still be underestimated, especiallyinpatientswiththelimitedformofSSc,because in these individuals only the Raynaud’s phenomenon is apparent formany years,withlittle systemicinvolvement; thus,theymaynotseekmedicalattention.Wesuggestthat epidemiologicalsurveysinSScareconductedinother Brazil-ian cities, in order to reflect possible regional differences and environmental influencesin the development ofboth diseases.
Conflict
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
We thankDr.Natalino Yoshinarifor hisencouragementto thisstudyandDr.AlbertSchiavetodeSouzaforthestatistical analysis.
r
e
f
e
r
e
n
c
e
s
1.VargaJ,AbrahamD.Systemicsclerosis:aprototypic multisystemfibroticdisorder.JClinInvest.2007;117: 557–67.
2.HerrickAL,WorthingtonJ.Geneticepidemiology
systemicsclerosis.ArthritisRes.2002;4:165–8. 3.VilasAP,VeigaMZ,AbecasisP.Esclerosesistémica–
perspectivasactuais.MedInt.2002;9:111–20.
4.DentonCP,BlackCM.Targetedtherapycomesofagein
scleroderma.TrendsImmunol.2005;26:596–602.
5.KayserC,AndradeLEC.Esclerosesistêmica.In:SatoE, editor.Guiasdemedicinaambulatorialehospitalar– reumatologia.SãoPaulo:Manole;2004.p.111–20.
6.MayesMD.Sclerodermaepidemiology.RheumDisClin
NAm.2003;29:239–54.
malignancy,andenvironmentaltriggers.CurrOpin
Rheumatol.2012;24:165–70.
8. FurstDE,FernandesAW,IorgaSR,GrethW,BancroftT. EpidemiologyofsystemicsclerosisinalargeUS
managedcarepopulation.JRheumatol.2012;39:
784–6.
9. ChifflotH,FautrelB,SordetC,ChatelusE,SibiliaJ. Incidenceandprevalenceofsystemicsclerosis:a systematicliteraturereview.SeminArthritisRheum. 2008;37:223–35.
10. KuoCF,SeeLC,YuKH,ChouIJ,TsengWY,ChangHC,
etal.Epidemiologyandmortalityofsystemicsclerosis:
anationwidepopulationstudyinTaiwan.ScanJ
Rheumatol.2011;40:373–8.
11. LeGuernV,MahrA,MouthonL,JeanneretD,CarzonM,
GuillevinL.PrevalenceofsystemicsclerosisinaFrench
multi-ethniccounty.Rheumatology.2004;43:1129–37.
12. WalkerUA,TyndallA,CzirjákL,DentonCP,
Farge-BancelD,Kowal-BieleckaO,etal.Geographical variationofdiseasemanifestationsinsystemic sclerosis:areportfromtheEULARSclerodermaTrials
andResearch(EUSTAR)groupdatabase.AnnRheum
Dis.2009;68:856–62.
13. SkareTL,LucianoAC,FonsecaAE,AzevedoPM.
Autoanticorposemesclerodermiaesuaassociac¸ãoao
perfilclínicodadoenc¸a.Estudoem66pacientesdosul doBrasil.AnBrasDermatol.2011;86:1075–81.
14. HoogenF,KhannaD,FransenJ,JohnsonSR,BaronM,
TyndallA,etal.2013classificationcriteriaforsystemic sclerosis:anAmericancollegeof
rhematology/Europeanleagueagainstrheumatism
collaborativeinitiative.AnnRheumDis. 2013;72:1747–55.
15. LeRoyEC,MedsgerTAJr.Criteriafortheclassificationof earlysystemicsclerosis.JRheumatol.2001;28:1573–6. 16. DellavanceA,GabrielAJr,CintraAFU,XimenesAC,
NuccitelliB,TabilertiBH,etal.IIConsensoBrasileirode
FatorAntinuclearemcélulasHep-2.RevBrasReumatol.
2003;43:129–40.
17. HildebrandtS,WeinerES,SenecalJL,NoellGS,
EarnshawWC,RothfieldaNF.Autoantibodiesto
topoisomeraseI(Scl-70):analysisbygeldiffusion,
immunoblot,andenzyme-linkedimmunosorbent
assay.ClinImmunolImmunop.1990;57:399–410.
18. CodulloV,MorozziG,BardoniA,SalviniR,Deleonardi G,PitàO,etal.Validationofanewimmunoenzymatic methodtodetectantibodiestoRNApolymeraseIIIin systemicsclerosis.ClinExpRheumatol.2007;25:373–7. 19. Estimativasdapopulac¸ãoresidentenoBrasile
unidadesdafederac¸ãocomdatadereferênciaem1◦de
julhode2014.RiodeJaneiro:IBGE;2014.Diretoriade Pesquisas(DPE),Coordenac¸ãodePopulac¸ãoe
IndicadoresSociais(Copis)(doi.http://www.ibge.gov.br/
home/presidencia/noticias/pdf/analiseestimativas
2014.pdf).
20. MüllerCS,PaivaES,AzevedoVF,RadominskiSC,Lima
FilhoJHC.Perfildeautoanticorposecorrelac¸ãoclínica
emumgrupodepacientescomesclerosesistêmicana
regiãosuldoBrasil.RevBrasReumatol.2011;51: 319–24.
21. HunzelmannN,GenthE,KriegT,LehmacherW,
MelchersI,MeurerM,etal.TheregistryoftheGerman
networkforsystemicscleroderma:frequencyofdisease
subsetsandpatternsoforganinvolvement.
Rheumatology.2008;47:1185–92.
22. FerriC,ValentiniG,CozziF,SebastianiM,MichelassiC, LaMontagnaG,etal.Systemicsclerosis:demographic,
clinical,andserologicfeaturesandsurvivalin1012 Italianpatients.Medicine(Baltimore).2002;81:139–53.
23.Sampaio-BarrosPD,BortoluzzoAB,MarangoniRG,
RochaLF,DelRioAPT,SamaraAM,etal.Survival, causesofdeath,andprognosticfactorsinsystemic sclerosis:analysisof947Brazilianpatients.J
Rheumatol.2012;39:1971–8.
24.AllcockRJ,ForrestI,CorrisPA,CrookPR,GriffithsID.A studyoftheprevalenceofsystemicsclerosisin
northeastEngland.Rheumatology.2004;43:596–602.
25.Revistadedivulgac¸ãodoarquivohistóricodeCampo
Grande–MS(ARCA)n◦13/2007.Tema:Campo
Grande–30anosdecapital.Oolhardahistóriaea perspectivadofuturo.Availableat:http://www.capital.
ms.gov.br/arca/canaisTexto?idcan=7304.
26.RosaJE,SorianoER,Narvaez-PonceL,delCidCC,
ImamuraPM,CatoggioLJ.Incidenceandprevalenceof
systemicsclerosisinahealthcareplaninBuenosAires. JClinRheumatol.2011;17:59–63.
27.FlowerC,NwankwoC.Systemicsclerosisinan
Afro-Caribbeanpopulation.Areviewofdemographic
andclinicalfeatures.WestIndianMedJ.2008;57:118–21.
28.MayesMD,LaceyJV,Beebe-DimmerJ,GillespieBW,
CooperB,LaingTJ,etal.Prevalence,incidence,survival, anddiseasecharacteristicsofsystemicsclerosisina largeUSpopulation.ArthritisRheum.2003;48:2246–55. 29.AlamanosY,TsifetakiN,VoulgariPV,SiozosC,
TsamandourakiK,AlexiouGA,etal.Epidemiologyof
systemicsclerosisinnorthwestGreece1981-2002.
SeminArthritisRheum.2005;34:714–20.
30.ThomsonPJR,WalkerJG,LuTY,EstermanA,Hakendorf
P,SmithMD,etal.SclerodermainSouthAustralia:
furtherepidemiologicalobservationssupportinga
stochasticexplanation.InternMedJ.2006;36:489–97.
31.RanqueB,MouthonL.Geoepidemiologyofsystemic
sclerosis.AutoimmunRev.2010;9:A311–8.
32.MayesMD.Classificationandepidemiologyof
scleroderma.SeminCutanMedSurg.1998;17:22–6.
33.RíosG,MayorAM.Clinicalandsociodemographic
featuresofPuertoRicanswithsystemicsclerosis.Ethn Dis.2010;20(S1):S185–9.
34.BasselM,HudsonM,TailleferSS,SchieirO,BaronM,
ThombsBD.Frequencyandimpactofsymptoms
experiencedbypatientswithsystemicsclerosis:results
fromaCanadianNationalSurvey.Rheumatology.
2011;50:762–7.
35.TamakiT,MoriS,TakeharaK.Epidemiologicalstudyof patientswithsystemicsclerosisinTokyo.Arch
DermatolRes.1991;283:366–71.
36.Al-AdhadhRN,Al-SayedTA.Clinicalfeaturesof systemicsclerosis.SaudiMedJ.2001;22:333–6.
37.LoMonacoA,BruschiM,LaCorteR,VolpinariS,Trotta F.Epidemiologyofsystemicsclerosisinadistrictof northernItaly.ClinExpRheumatol.2011;29(S65): S10–4.
38.JezlerSFO,SantiagoMB,AndradeTL,AraujoNetoC,
BragaH,CruzAA.Comprometimentodointerstício
pulmonaremportadoresdeesclerosesistêmica
progressiva.Estudodeumasériede58casos.JBras
Pneumol.2005;31:300–6.
39.NietertPJ,MitchellHC,BolsterMB,ShaftmanSR,Tilley BC,SilverRM.Racialvariationinclinicaland
immunologicalmanifestationsofsystemicsclerosis.J
Rheumatol.2006;33:263–8.
40.HesselstrandR,SchejaA,ShenGQ,WiikA,ÅkessonA.
involvementandsurvivalinsystemicsclerosis.
Rheumatology.2003;42:534–40.
41. MierauR,MoinzadehP,RiemekastenG,MelchersI,
MeurerM,ReichenbergerF,etal.Frequencyof
disease-associatedandothernuclearautoantibodiesin
patientsoftheGermannetworkforsystemic
scleroderma:correlationwithcharacteristicclinical features.ArthritisResTher.2011;13:R172.
42.BernsteinRM,SteigerwaldJC,TanEM.Associationof antinuclearandantinucleolarantibodiesinprogressive systemicsclerosis.ClinExpImmunol.1982;48: