Revista
Portuguesa
de
Cardiologia
Portuguese
Journal
of
Cardiology
www.revportcardiol.org
CASE
REPORT
Short
QT
syndrome
presenting
as
syncope:
How
short
is
too
short?
Guilherme
Portugal
∗,
Mário
Martins
Oliveira,
Pedro
Silva
Cunha,
Filipa
Ferreira,
Ana
Lousinha,
António
Fiarresga,
Manuel
Nogueira
da
Silva,
Rui
Cruz
Ferreira
Servic¸odeCardiologia,HospitaldeSantaMarta,CentroHospitalarLisboaCentralEPE,Lisboa,Portugal
Received22October2013;accepted17May2014 Availableonline22October2014
KEYWORDS Syncope; ShortQTsyndrome; Suddencardiac death; Ventricular arrhythmia
Abstract Wereportthecaseofa52-year-oldmanwhopresentedtoouremergency depart-ment (ED) after threeepisodesofsyncope inthe sevenhours before admission. Duringhis stayintheEDhehadrecurrentventriculartachycardia(VT)requiringexternalelectrical car-dioversion.A12-leadelectrocardiogram(ECG)showedashortQT(SQT)interval(270ms,QTc 327ms),withfrequentR-on-TextrasystolestriggeringsustainedpolymorphicVT.After exclu-sionofotherprecipitatingcauses,thepatientwasdiagnosedashavingSQTsyndrome(SQTS) accordingtotheGollobcriteria.Toourknowledge,thisisthefirstknowndocumentationofan SQT-causedarrhythmicepisodeona12-leadECG,aswellasthefirstreportedcaseofSQTSin Portugal.Thepatientreceivedanimplantablecardioverter-defibrillatorandwasdischarged. Atafollow-upassessment14monthslaterhewassymptom-free,interrogationofthedevice showednoarrhythmicevents,andtheECGshowedaQTintervalof320ms(QTc347ms). © 2013SociedadePortuguesade Cardiologia.Publishedby ElsevierEspaña,S.L.U.Allrights reserved. PALAVRAS-CHAVE Síncope; SíndromeQTcurto; Mortesúbita cardíaca; Arritmiaventricular
QuandoointervaloQTécurtodemais:síncopecausadaporsíndromeQTCurto
Resumo Osautoresapresentamocasodeumhomemcom52anosquerecorreuaoServic¸o de Urgência(SU)portrêsepisódios sincopaisocorridos nasúltimassetehoraspré-admissão hospitalar.DuranteaestadianoSU,objetivaram-seperíodosdetaquicardiaventricular(TV) recorrente,comnecessidadedecardioversãoelétricaexterna,tendoodoentesidotransferido paraaunidadedecuidadosintensivoscardíacosparamonitorizac¸ãoeorientac¸ãoclínica.O el-ectrocardiogramade12derivac¸ões(ECG)registadonocontextodeumdosepisódiosrevelava um intervalo QT curto (260 ms, QTc 327 ms) em ritmo sinusal, com fenómeno de R-on-T desencadeando TVpolimórficamantida.Apósexclusãodecausasprecipitantes,odoentefoi
∗Correspondingauthor.
E-mailaddress:[email protected](G.Portugal). http://dx.doi.org/10.1016/j.repc.2014.05.005
classificado como tendoSíndrome QT Curto (SQTC),de acordo comos critérios de Gollob. Tantoquantoédonossoconhecimento,estaéaprimeiradocumentac¸ãonoECGdeum episó-dioarrítmicocausadoporSQTCeaprimeiradescric¸ãodeumcasodeSQTCemPortugal.Foi submetidoaimplantac¸ãodecardioversor-desfibrilhadorimplantável(CDI)monocameraleteve alta hospitalar.Noseguimento aos14mesespós-implantac¸ão,odoente negavarecorrência dasintomatologia,ainterrogac¸ãodoCDInãomostrou novosepisódiosarrítmicos, enoECG persistiaumintervaloQTde320ms(QTc347ms).
©2013SociedadePortuguesadeCardiologia.PublicadoporElsevierEspaña,S.L.U.Todosos direitosreservados.
Listofabbreviations ECG electrocardiogram ED emergencydepartment
ICD implantablecardioverter-defibrillator PVC prematureventricularcontractions PVT polymorphicventriculartachycardia QTc correctedQT
SQT shortQT
SQTS shortQTsyndrome VT ventriculartachycardia
Case
report
A52-year-oldmanpresentedtoouremergencydepartment (ED)duetothreeepisodesofsuddentransientlossof con-sciousnessinthesevenhoursbeforehospitaladmission.The firsteventoccurredat2:00am,whilethepatientwaslying in bed, recurring at 4:00 am and 7:00 am. He reported malaise,butdeniedprodromes,chestpain,palpitationsor dyspnea.Hiswife,whowitnessedtheepisodes,described themaslastingforaboutfiveminutes,withspontaneousand complete recovery.Therewasnoevidence of seizure-like activity.
Thepatienthadnohistoryofknowncardiovascular dis-easeand norecollection of previous episodesofsyncope. Hisfatherdied at38yearsofage duetosuddendeathof undeterminedorigin,withnootherrelevantfamilyhistory. His medicalhistory wasnotable for depression (managed atan outpatientclinic), duodenal pepticulcer(five years previously),andhypercholesterolemia.Hisregular medica-tionconsistedofmirtazapine30mgdaily,alprazolam0.5mg daily,bupropion300mgdailyandfenofibrate200mgdaily. He had no clinical allergies and denied smoking, alcohol intakeoranykindofaddiction.
Physicalexaminationshowedawell-nourishedmanwith noexternalsignsofdistress.Atadmission,hewasafebrile, with blood pressure of 112/65 mmHg, heart rate of 76bpmandoxygensaturationof98%bypulseoximetry. Car-diacexaminationshowedanirregularheartrhythmwithno murmurs.The rest of the physical examination was unre-markable.
During his assessment in the ED, he suffered a new episodeofsyncopewithspontaneousrecovery,andcardiac
monitoring during the event showed a polymorphic ven-triculartachycardia(PVT). Despiteintravenousinfusion of amiodarone and magnesium sulphate, there was recur-rence of the cardiac arrhythmia requiring a total of five externalelectricalcardioversions.A12-lead electrocardio-gram(ECG)recordedduringonesucheventispresentedin
Figure1.
Abloodchemistrypanelshowednormalserumpotassium and magnesium, withno hypocalcemia. Cardiac biomark-ers were negative, and other laboratory investigations were unremarkable. The patient was transferred to our cardiacintensivecareunitforfurtherassessmentand treat-ment.
CarefulreviewofECGrecords(Figures1and2)showed a shortQTinterval(280ms,QTc 329msaccording tothe Bazettformula).GiventhesettingofaPVTstormcoronary angiographywasperformed,whichruledoutcoronaryartery diseaseoranomalouscoronaryorigin(Figures3and4),with normal wall motion and left ventricular ejection fraction (70%).Transthoracicechocardiographicexaminationshowed anormalheartwithgoodleftventricularsystolicfunction andnosignsofstructuraldisease.
Intheabsenceofothercauses,apresumptivediagnosisof shortQTsyndrome(SQTS)wasmade,andquinidinetablets wererequestedfromthehospitalpharmacy.Thepatientwas classifiedashigh-probabilitySQTSaccordingtotheGollob criteria,1withascoreof5(Table1).
In-patient 24-hour Holter monitoring was performed and showed infrequent dimorphic premature ventricular contractions(PVCs), withnorepetitivepatterns. An elec-trophysiologicstudywasperformedandwasnotableforthe induction of self-limited PVT with hemodynamic collapse (inductionprotocol: S1400/S2200ms,pacingattheright ventricular apex). The measured right ventricular refrac-toryperiodwasshortened(200ms).Noattemptwasmade toinduceatrialfibrillation.Themeasuredatrialrefractory periodwas350msintherightatriumand200msintheleft atrium(asmeasuredinthedistalcoronarysinus).
In accordance with the ACCF/AHA/HRS guidelines for device-basedtherapy,2thepatientreceivedanimplantable cardioverter-defibrillator (ICD) as secondary prevention indicated for SQTS,repeatedsyncopes andinducible PVT. There were noprocedural complications and he was dis-chargedonhispreviousmedicationandquinidine.
At a follow-up visit 14 months later, the patient was feeling well and had had no new episodes of syncope or palpitations. Physical examination was unremarkable. ICD deviceinterrogationshowednoshocksorarrhythmicevents,
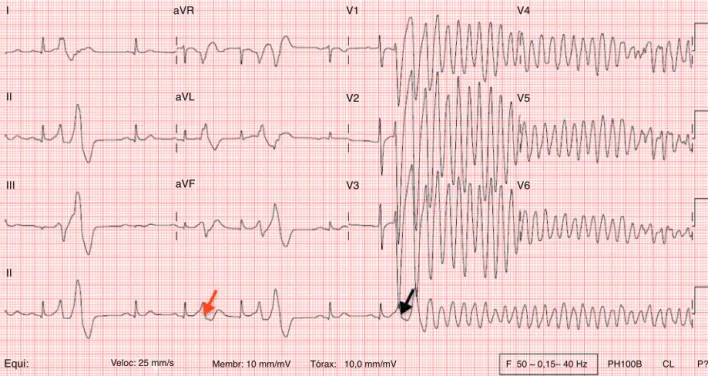
I aVR aVL aVF V1 V2 V3 V4 V5 V6 II III II
Equi: Veloc: 25 mm/s Membr: 10 mm/mV Tórax: 10,0 mm/mV F 50 ~ 0,15– 40 Hz PH100B CL P?
Figure1 This12-leadECGrecordedduringasyncopalepisodeshowssinusrhythmwithaheartrateof83bpm.Thetracingshows ashortenedQTinterval(320ms)withfrequentprematureventricularcontractions(PVCs)causingR-on-Textrasystoles(redarrow). OnePVC(blackarrow)triggerspolymorphicventriculartachycardiawhichcausedlossofconsciousness.
Table 1 Proposed diagnostic criteria for short QT syndrome. Criterion Points QTc,ms <370 1 <350 2 <330 3 Jpoint-Tpeakinterval<120ms 1 Clinicalhistory
Historyofsuddencardiacarrest 2 DocumentedpolymorphicVTorVF 2 Unexplainedsyncope 1 Atrialfibrillation 1
Familyhistory
First-orsecond-degreerelativewith high-probabilitySQTS
2 First-orsecond-degreerelativewith
autopsy-negativesuddencardiacdeath
1 Suddeninfantdeathsyndrome 1
Genotype
Genotypepositive 2 Mutationofundeterminedsignificance
inaculpritgene
1
QTc:correctedQT;SQTS: shortQTsyndrome;VF:ventricular fibrillation;VT:ventriculartachycardia.High-probabilitySQTS:4 points;intermediate-probabilitySQTS:3points;low-probability SQTS:2points.
AdaptedfromGollobetal.1
RR=0.68 s
QT = 270 ms
Figure2 Electrocardiographic recording,lead V2, showing shortenedQTinterval(270ms)withRRintervalof0.68s.The QTcintervalaccordingtotheBazettformula12is327ms.
andrepeatECGassessment(Figure4)showedaQTinterval of320ms(QTc347ms).
Genetic testing was performed, and screening of the
KCNJ2, KCNH2 and KCNQ1 genes by polymerase chain
reactionwasnegativeforshortdeletionsormissense muta-tions.
Totheauthors’knowledge,thisisthefirstreportedcase ofSTQSinPortugal,whichisinagreementwiththeverylow prevalenceofthiscondition.Asanindexcase,ECGscreening offamilymembersisunderway.
Figure3 Coronaryangiographyoftheleftandrightcoronarycirculationshowednosignificantdisease.
Figure4 ECGrecordingatfollow-up.
Discussion
Suddencardiacdeathisoneoftheleadingcausesofdeathin theindustrializedworld,andventriculararrhythmiashave longbeenrecognizedasoneofthecausativemechanisms. Whiletheseusuallyoccurinthesettingofstructuralheart disease,theymayalsobea consequenceofan acute pro-cessoraninheritedpredispositionofanindividual’scardiac tissuetolife-threateningarrhythmias.
These primary cardiac electrical diseases, although uncommon,areusuallydetectedinyounger3andotherwise healthyindividuals,oftenwithtragicconsequences.
SQTSisarecentlydescribedentityincludedinthegroup of inherited primary electric disorders. As originally pro-posedbyGussak in2000,4it involved theassociation ofa significantlyshortenedQTcintervalonthesurfaceECGwith atrialfibrillationandsuddencardiacdeath.
Since itsdescription in two families,5 our understand-ingofthisrareentityhasevolved,buttherearestillmany questionstoanswer,particularlyregardingitsincidenceand prognosis.
OurpatientwasinitiallyassessedintheEDwitha clini-caldiagnosisofsyncope.Whilethisisacommoncomplaint in the ED, representing up to 3% of all visits, its causes range frombenign vasovagal reactions to life-threatening cardiacarrhythmias.Inthisclinicalsetting,thepresentation of recurrentsyncope at rest,without knownprecipitating events,suggestedapotentiallyseriousunderlyingprocess.
After documentation of an arrhythmic cause, the patient’ssevereelectricalinstabilitycouldhavebeen asso-ciatedwithanacutemyocardialischemicprocess,butthis wasruledoutbypersistentlynegativeserumtroponinanda normalcoronaryangiogram.Intheabsenceofother precip-itating causes,withECGsshowingashortenedQTinterval withoutstructuralheartdisease,apresumptivediagnosisof SQTSwasmade.To ourknowledge,thisis thefirstknown documentationona12-leadECGofR-on-Textrasystolesin ashortQT-relatedarrhythmicepisode.
IncontrastwithlongQTinterval,whichmaybebrought on by external factors, including certain drugs, there is no known association between medication and a short-ened QT interval. However, due to an overlap of QTc
Table2 AssociationbetweengenotypeandphenotypeinshortQTsyndrome.
Type Geneinvolved Chromosomelocus
SQTS1 KCNH2---potassiumvoltage-gatedchannel,subfamilyH(eag-related),member2 7q36.1 SQTS2 KCNQ1---potassiumvoltage-gatedchannel,KQT-likesubfamily,member1 11p15.5-p15.4 SQTS3 KCNJ2---potassiuminwardly-rectifyingchannel,subfamilyJ,member2 17q24.3 SQTS4 CACNA1C---calciumchannel,voltage-dependent,Ltype,alpha1Csubunit 12p13.3 SQTS5 CACNB2---calciumchannel,voltage-dependent,beta-2subunit 10p12.33-p12.31 SQTS6 CACNA2D1---calciumchannel,voltage-dependent,alpha-2/deltasubunit1 7q21.11
AdaptedfromComellietal.13
values between healthy population cohorts and patients withSQTS,6,7 hyperkalemia,hypo-or hypercalcemia,sinus tachycardia,hypothermia,acidosisordigoxintherapymust beexcluded.AcaseofshortQTrelatedtoprolonged resus-citationeffortsandhypothermiahasalsobeendescribed,8 butthiswasnotthecaseinourpatient.
SimilarlytothelongQTsyndrome,thereappearstobe significant overlapof QTcvaluesbetween healthy popula-tioncohorts and patients withSQTS.6,7 This suggests that an abbreviatedQTintervalisnotin itselfthecauseofan increasedrisk of arrhythmia, butmay bea surface surro-gateforthearrhythmogenicsubstrateinSQTSpatients.As such,adiagnosisofshortQTsyndromeshouldonlybe con-sideredfollowingcarefulassessmentofthe12-leadECG,in anappropriateclinicalsetting(historyofsyncopeoraborted suddencardiacdeath,positivefamilyhistory),assuggested bytheGollobscore.
As the QTinterval isheart-rate dependent, use of the BazettformulaallowsestimationoftherealQTinterval(as measuredat60bpm)atanyheartrate.Somecautionmust beusedinitsapplication,astheformulahasbeenreported toundercorrect(yieldingerroneouslyhighQTcintervals)at heart rates above 90 bpm.14 However,measuring the QT intervalataheartrateof60bpmisnotalwaysfeasiblein clinicalpracticeasitmayrequiretheuseofbeta-blockers or Holter monitoring, and the Bazett formula remains an acceptablysimpleandeffectivetoolatthebedside.
The described cellular mechanism behind idiopathic shortQTintervalisusuallyrelatedtogain-of-function muta-tions in potassium channels; these lead to a shortened action potential duration through accelerated cardiomy-ocyte repolarization. So far, six different genotypes have been conclusively associated with SQTS (Table 2), but genetictestingwasnegativein71%ofthereportedcases,1 suggestingthatothergeneticmutationsremaintobe iden-tified.
Althoughgenetictestinghassofarshownalowdiagnostic yield,ahereditarycomponentwasfoundin71.9%ofindex casesinthestudybyGollobetal.2However,applicationof a diagnostic scoreto familymembers may underestimate theprevalenceofSQTSduetotheincompletepenetrance ofinherited cardiacelectricaldisorders.ECG screeningof familymembersappearstobeapracticalandcost-effective tool.
The ideal long-term management of this rare clinical entityhasyettobeestablished.Intheory,pharmacological therapywithaQT-prolongingdrugshouldbeeffectivein cor-rectingtheshortQTinterval;however,mostQT-prolonging
drugs,suchasflecainideorsotalol,areineffectiveinthese patients.9RecentdatashowthatmostQT-prolongingdrugs have the highest affinity for the inactivated state of the potassiumchannelKv11.1.10Curiously,inSQTS,Kv11.1 inac-tivationisusuallyabolished,conferringrelativeresistance to the action of these drugs. An exception is quinidine, whichbinds withequal affinitytoboth the activatedand inactivatedstates of Kv11.1, and has proved effective in prolongingtheQTintervaluptonormalinthesepatients.9,7 Arecentreporthasshown thatthearrhythmiceventrate in SQTS patients taking hydroquinidine during long-term follow-up was lower than if no drug was used (0.0% vs. 4.9%/year),althoughthisdifferencewasnotstatistically sig-nificant,probablyowing tothesmallsample size.11 Thus, quinidinemaybeauseful treatment forselectedpatients withSQTS,suchasthosewithcontraindicationtoorrefusing ICDimplantation.
Current guidelines2 recommend ICD implantation for patients with genetic arrhythmia syndromes (including SQTS)andpriorcardiacarrestorsyncope,andalsoforthose withafamilyhistoryofsuddencardiacdeathandinduction ofventriculartachyarrhythmias,astheyareconsidered to beat highrisk forrecurrentmalignantarrhythmicevents. Implantationforprimarypreventionmaybeconsidered in patientsclassifiedashighprobabilityonthebasis oftheir Gollobscore.1
Inourpatient,noarrhythmicevents or relevant symp-tomswererecordedduringa14-monthfollow-up.Thisisin agreementwiththereportedlowincidenceofevents ina cohortof SQTSpatients,13 withan event rateof 3.3%per year.Specifically,inthesubsetofpatientspresentingwitha historyofsyncope,onlyoneeventwasobserved,inapatient withahERGmutation(SQTS1)whoreceivedanappropriate shockforventricularfibrillation.
Among the causes of sudden cardiac death in young people, SQTS is a relatively recent entity. The recogni-tionof this rare syndrome has allowed reclassification of individuals who would previously have been classified as having idiopathic ventricular fibrillation, as is the case with our patient. Any suspected cases of SQTS should be referred to specialized centers where they can be offered a multidisciplinary approach and disease-specific therapeuticinterventions,suchasquinidineorICD implan-tation,accordingtoSQTSriskstratification. Inthefuture, further advances in our knowledge of inherited chan-nelopathieswillhopefullyhelpintheearlyrecognitionand prevention of arrhythmic events in this high-risk popula-tion.
Ethical
disclosures
Protection of human and animal subjects.The authors declarethat the proceduresfollowed were in accordance withtheregulationsoftherelevantclinicalresearchethics committeeandwiththoseoftheCodeofEthicsoftheWorld MedicalAssociation(DeclarationofHelsinki).
Confidentialityofdata.Theauthorsdeclarethattheyhave followedtheprotocolsoftheirworkcenteronthe publica-tionofpatientdata.
Righttoprivacyandinformedconsent.Theauthorshave obtainedthe written informed consentof the patients or subjectsmentionedinthearticle.Thecorrespondingauthor isinpossessionofthisdocument.
Conflicts
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
References
1.GollobM,RedpathC,RobertsJ.TheshortQTsyndrome--- pro-poseddiagnosticcriteria.JACC.2011;57:802---12.
2.Tracy CM, Epstein AE, Darbar D, et al. American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society 2012. ACCF/AHA/HRSFocused Update incorporatedinto the ACCF/AHA/HRS2008 Guidelinesfor Device-BasedTherapy of CardiacRhythmAbnormalities.JACC.2013;61:e6---75.
3.LiberthsonRR.Suddendeathfromcardiaccausesinchildren andyoungadults.NEnglJMed.1996;334:1039---44.
4.GussakI,BrugadaP,BrugadaJ,etal.IdiopathicshortQT inter-val:anewclinicalsyndrome?Cardiology.2000;94:99---102. 5.Gaita F, Giustetto C, Bianchi F, et al. Short QT syndrome:
a familial cause of sudden death. Circulation. 2003;108: 965---70.
6.AnttonenO,JunttilaMJ,RissanenH,etal.Prevalenceand pro-gnosticsignificanceofshortQTintervalinamiddle-agedFinnish population.Circulation.2007;116:714---20.
7.Gallagher MM, Magliano G, Yap YG, et al. Distribution and prognostic significance of QT intervals in the lowest half centile in12,012 apparently healthypersons. Am JCardiol. 2006;98:933---5.
8.OkishigeK,SugiyamaK,MaedaM,etal.Abortedsudden car-diacdeathassociatedwithshortQTsyndrome.JArrhythmia. 2009;25:214---8.
9.GaitaF,GiustettoC,BianchiF,etal.ShortQTsyndrome: phar-macologicaltreatment.JAmCollCardiol.2004;43:1494---9. 10.Perrin MJ, Kuchel PW, Campbell TJ, et al. Drug binding to
theinactivated stateisnecessarybutnotsufficientfor high-affinitybindingtohumanether-à-go-go-relatedgenechannels. MolPharmacol.2008;74:1443---52.
11.GiustettoC,SchimpfR,MazzantiA, etal.Long-term follow-up of patients with short QT syndrome. J Am Coll Cardiol. 2011;58:587---95.
12.BazettHC.Ananalysisofthetime-relationsof electrocardio-grams.Heart.1920;7:353---70.
13.ComelliI,LippiG, MossiniG,et al.ThedarksideoftheQT interval.TheshortQTsyndrome:pathophysiology,clinical pre-sentationandmanagement.EmergCareJ.2012;3:41---7. 14.WernickeJF,FariesD,BreitungR,etal.QTcorrection
meth-ods in children and adolescents. Cardiovasc Electrophysiol. 2005;16:76---81.