ABSTRACT
INTRODUCTION
Patient recovery time after anesthesia depends on problem-oriented monitoring andindividualassessment.Thepost-anesthe-siacareunitprovidesstate-of-the-artsetup, equipmentandfacilitiestocareforpatients recoveringfromanesthesia.
Thetypeofanesthesiaadministeredhas littleinfluenceontheneedforpostanesthesia care.Thisimpliesthatthepost-anesthesiacare unitmaysometimesbeoverloaded,thereby imposingtheriskofjammingofthepatient flowthroughthishospitalunit.Inaddition, suchoverloadinginthisunitmaydelaythe hospital’s operating room schedule. Among thereasonsforlowbedavailabilityinthepost-anesthesiacareunitareclinicalassessmentsthat maybeslow-pacedandlowdischargeratesdue toreducednursingstaffavailability.1
Ideally, all the patients coming from thesurgicaltheatershouldbeindicatedfor recoverywithinthepost-anesthesiacareunit. Patient transportation and admission are undertheresponsibilityofanesthesiologists, whoperformafirstphysicalevaluationand give guidance to nursing staff for them to followclinicalrecoverypatterns,asindicated bytheAldrete-Kroulikmodifiedscale.2
Ponhold andVicenzi have shown that there was lower incidence of bradycardia duringrecoveryfromspinalanesthesiawhen patientswereallowedtostayinaposition with their trunk and legs elevated at 30 degrees(hammockposition).3Sinceastable
heartrateisoneofthedeterminantsoffull recovery from anesthesia within the post-anesthesiacareunit,itseemedreasonableto
considerwhetherthepatientpositioncould influencethedurationoftherecoveryduring thepost-anesthesiacareperiod.
The distinct supervision care adopted bysomeanesthesiologists,inrelationtothe post-anesthesiapatientposition,hascreateda naturalenvironmentforinvestigatingwheth-er different patient positions would give risetodifferencesinthetimerequiredfor recovery.Theobjectiveofthisstudywasto investigatewhethermodifyingthepatient’s position when recovering from anesthesia would shorten the postoperative recovery timeinthepost-anesthesiacareunit.
METHODS
ThepresentstudywasperformedatHos-pitaldasClínicas,UniversidadedeSãoPaulo, a tertiary-level public hospital.The study protocol was approved by the institution’s Ethics Committee.This investigation was designedasaretrospectivestudy,sincethere would not be any possibility of interven-tionregardingtherecoverypositionforthe patientsadmittedtothepost-anesthesiacare unit.Patientsadmittedtothepost-anesthesia careunithadtheirpost-anesthesiarecovery timerecordedbymeansofthenurse’sregis-teringsysteminthatunit.Onlythepatients keptinthesupinehorizontalpositionorwith theirtrunkandlegselevatedat30degrees (hammockposition)wereconsideredforthis study. Patients in any other position were notincluded.Pregnantwomenandpatients undertheageoftwelveyearsoldwerealso excluded.Allpatientsinthisunitwereposi-tionedonabedwithnopillow.
OriginalA
rticle
•OtávioOmati
•FábioElyMartinsBenseñor •JoaquimEdsonVieira
Elevationofapatient’strunk
andlegsdoesnotinfluence
lengthofstayinthepost-anesthesiacareunit
Post-anesthesiacareunit,HospitaldasClínicas,FaculdadedeMedicinada
UniversidadedeSãoPaulo,SãoPaulo,Brazil
CONTEXT: Patient recovery time after anesthesia depends on problem-oriented monitoring and individualassessment.
OBJECTIVE: To investigate the influence of patient positioningonpost-anesthesiarecoverytime.
TYPEOFSTUDY:Retrospective.
SETTING: Post-anesthesia care unit, Hospital das Clínicas,SãoPaulo.
METHODS: Datawereobtainedfrompatientsrecover-ingfromanesthesiainasupinehorizontalposition orwiththeirtrunkandlegselevatedat30degrees. Datawererecordedevery30minutes.Thestart timewasconsideredtobetheadmissiontothe unit,andthefinalmeasurementwastakenwhen thepatientreachedanAldrete-Kroulikindexof10. Thelengthoftimeuntildischargewasrecorded.
RESULTS: 442 patients recovering after general (n = 274) or regional anesthesia (n = 168) were assigned to be kept in a supine position orwiththeirtrunkandlegselevated.Therewas nodifferenceinthemediansfornon-parametric results,betweensupineposition(75min,n=229) andtrunkandlegselevated(70min,n=213); p=0.729.Patientsrecoveredfasterfromregional anesthesiawithtrunkandlegselevated(70min) thaninthesupineposition(84.5min),although notsignificantly(p=0.097).Therewasnodif-ferencebetweenpatientsrecoveringfromgeneral anesthesia, no matter the positioning (70 min; p=0.493).
DISCUSSION:Elevatedlegsmaysupposedlyimprove venous return and cardiac output since spinal anesthesia blocks sympathetic system and con-sideringleg-raisinghasbeenshowntoimprove cardiac output from hipovolemia. Our findings didnotsupportthishypothesis.Somelimitations includedaretrospectivecollectionofdatathatdid notallowrandomizationforrecoverypositionand theunregistereddurationoftheexposuretothe anestheticdrugs.
CONCLUSIONS: Therewasnodifferenceinanesthe-siarecoverytimeinrelationtopositioningpatients supinelyorwithtrunkandlegselevated.
KEYWORDS:Anesthesia.Supineposition.Anesthesia recovery period. Position modalities. General anesthesia.
SãoPauloMedicalJournal—RevistaPaulistadeMedicina
214
Patients’demographicdataandthetypeof anesthesiatheyhadbeengivenwererecorded. Therecoveryperiodwasdefinedastheperiod betweenadmissiontothepost-anesthesiacare unitandthetimewhenthedischargecriteria according to the Aldrete-Kroulik scale were reached. It did not include the period be-tweenreachingthedischargecriteriaandthe momentwhenthepatientlefttheunit.The nursingstaffassessedpatientsontheAldrete-Kroulik scale every thirty minutes. Patients receivedanalgesicsandintravenousfluidwhen indicatedbytheanesthesiologistresponsible forthepost-anesthesiacareunit.
Theidealdischargemomentwasconsid-eredtobewhenthepatientreachedalevelof 10,accordingtothemodifiedAldrete-Kroulik post-anesthesia recovery scale.This scoring systemincludesthefollowingfactors(scores indicatedinbrackets):
1. Limbmovements:nomovementinany ofthefourlimbs(0),nomovementin twolimbs(1),movementrestoredinall limbs(2);
2. Awareness response: not responding to his/her name (0), a response to his/her name(1),completelyawake(2); 3. Blood pressure measurement: less than
20%ofwhatwasrecordedbeforeanes-thetizing (0), between 20% and 50% (1),morethan50%ofthepre-anesthesia bloodpressure(2);
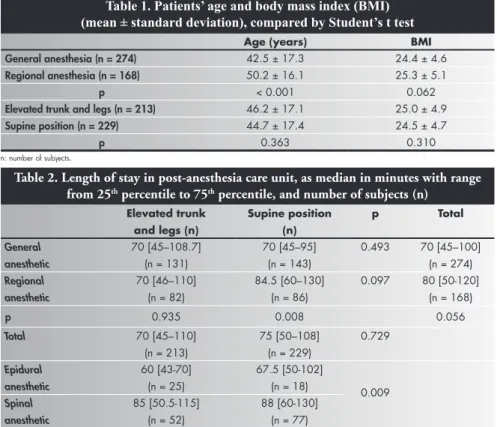
Table 1. Patients’ age and body mass index (BMI) (mean ± standard deviation), compared by Student’s t test
Age(years) BMI
Generalanesthesia(n=274) 42.5±17.3 24.4±4.6
Regionalanesthesia(n=168) 50.2±16.1 25.3±5.1
p <0.001 0.062
Elevatedtrunkandlegs(n=213) 46.2±17.1 25.0±4.9
Supineposition(n=229) 44.7±17.4 24.5±4.7
p 0.363 0.310
n:numberofsubjects.
Table2.Lengthofstayinpost-anesthesiacareunit,asmedianinminuteswithrange from25thpercentileto75thpercentile,andnumberofsubjects(n)
Elevatedtrunk andlegs(n)
Supineposition (n)
p Total
General anesthetic
70[45–108.7] (n=131)
70[45–95] (n=143)
0.493 70[45–100] (n=274)
Regional anesthetic
70[46–110] (n=82)
84.5[60–130] (n=86)
0.097 80[50-120] (n=168)
p 0.935 0.008 0.056
Total 70[45–110]
(n=213)
75[50–108] (n=229)
0.729
Epidural anesthetic
60[43-70] (n=25)
67.5[50-102]
(n=18) 0.009
Spinal anesthetic
85[50.5-115] (n=52)
88[60-130] (n=77)
4. Peripheral hemoglobin saturation: less than90%withoxygensupplyunderfacial mask (0), more than 90% with oxygen supplyunderfacialmask(1),morethan 90%inroomair(2);
5. Breathingpattern:apnea(0),hypoventila-tionordyspnea(1),deepbreathingand coughcapability(2).
ThesumoftheAldrete-Kroulikcriteria canreachamaximumoften,therebyestab- lishingapatient’sfinalconditionasfullyrecov-eredfromanesthesia.2However,thedischarge
criteriaalsoincludewell-establishedgeneral conditionssuchasabsenceofnauseaorvomit-ing,andalsogoodcontroloverpain.
The lengths of stay were compared via theMann-Whitneyranksumtest,sincethere wasnonormaldistributionfortherecovery time,andthesignificancelevelwassetat95%. For patients under regional anesthesia, the Kruskal-Wallisanalysisofvariance(ANOVA) ofranksandDunn’stestwereperformed.De-mographicdatawasevaluatedusingStudent’s ttest,withthesignificancelevelsetat95%. [whenpvalueis<0.05]
RESULTS
During the months of January through March 2002, approximately 1,050 patients wereadmittedtothepost-anesthesiacareunit
ofHospitaldasClínicas.Fromthistotal,442 patientswereincludedinthisstudyprotocol, ofwhom229werekeptinasupineposition and213withtheirtrunkandlegselevated.
Ofthese442patients,274hadunder-gone general anesthesia and 168 regional anesthesia(withbupivacaine).Thepatients whoreceivedregionalanesthesiaweresignifi-cantlyolder(50.2±16.1)thanthoseunder generalanesthesia(42.5±17.3),byStudent’s ttest(p<0.001;mean±SD).Therewasno differenceinbodymassindexbetweenpa-tientsunderregionalanesthesia(25.3±5.1) andthoseundergeneralanesthesia(24.4± 4.6)(p=0.062).Inrelationtotherecovery position utilized, there was no difference forage(p=0.363)orbodymassindex(p =0.310).Ageandbodymassindexdataare showninTable1.
Thedataonthelengthofstayinthepost- anesthesiacareunitwereconsideredtobenon-parametric.Thus,themedianstaywasutilized forthecomparisonofthesupinepositionwith elevatedtrunkandlegs,togetherwiththerange fromthe25thtothe75thpercentile.Theresults
showedthattherewasnodifferenceinlength ofstaybetweenpatientsinthesupineposition (median=75min;range:50-108)orwithel-evatedtrunkandlegs(70min;range:45-110), bytheMann-Whitneytest(p=0.729).
Patients recovered faster from regional anesthesia when the trunks and legs were elevated(70min;range:46-110)thanwhen they were in the supine position (84.5 min; range:60-130),althoughthiswasnotstatisti-callysignificant(p=0.097).However,there was no difference in patients’ recovery rate followinggeneralanesthesia,nomatterwhich positionwasutilized.Itisinterestingtonotice that,althoughtherecoverytimeinthesupine horizontalpositionwasfasterforgeneral(70 min;range:45-95)thanforregionalanesthesia cases(84.5min;range:60-130)(p=0.008), patients recovering from regional anesthesia seemedtorecoverfasterwiththeirtrunkand legselevated(p=0.009)(Table2).
DISCUSSION
In the present study, the patient’s body positionduringthepost-anesthesiacareperiod did not influence the recovery time at the post-anesthesia care unit.The patients who receivedregionalanesthesiawereolderthan thoseassignedforgeneralanesthesiainthis selectedsample.Thiscouldbeconsideredto betheresultofdifferencesindiseaseincidence. Regionalanesthesiaiscommonlyindicatedfor surgical procedures on the lower abdomen,
SãoPauloMedicalJournal—RevistaPaulistadeMedicina
215
OriginalA
rticle
suchasinthetreatmentofurogenitaldisease, forwhichtheprevalencemaybehigheramong theelderly.Nevertheless,theyoungerpatients didnotshowabetterrecoverytime,foreither positioninvestigated.Therewasnodifference intherecoverytimeaftergeneralanesthesia whenusingthesupinepositionorelevating the trunk and legs position (70 minutes in eachcase),buttherecoverywaslongerfollow- ingregionalanesthesiawhenthesupineposi-tionwasutilized.Thislongerrecoverytime mayhaveresultedfromthelargeproportion ofthesamplethatunderwentspinalanesthesia andwereassignedtothesupineposition.
Spinalanesthesiablocksthepre-gangli-onicsympatheticsystemandhencereduces cardiac output. This physiological effect comesfromthereducedstrokevolumeand veindilation.4Italsoreducesthereleaseof
catecholamines from the adrenal medulla whenablockadeofefferentautonomicpath-waysisachieved.5Thesepossibilitiesmight
add to the physiological supposition that elevated legs may improve venous return and cardiac output. It has been reported, however,thatneitherlegelevationnorthe Trendelenburgbodypositioninfluencesthe autonomic cardiac control among wakeful andnon-anesthetizedvolunteers.6
Passive leg-raising has commonly been usedfortheinitialtreatmentofhypovolemic shock.However,therearereportsthathave pointedoutthatthisdoesnotproduceany significantauto-transfusioneffect,including in patients with coronary artery diseases.7
Although the controversy may remain, the leg-raising maneuver may be capable of in-creasing stroke volume and cardiac output
in hypovolemic humans.8 In addition, the
strokeindexofapatientinaseatedposition doesnotdifferfromthesupinepositionwhen recoveringfromexercise,whenthesystemic vascular resistance index decreases.9 Since a
patientunderregionalanesthesiacanexperi-ence significant decrease in total peripheral resistanceinassociationwithreducedvenous return,itwouldbereasonabletoconsiderthat thepositionwithtrunkandlegselevatedcan addtotherecoveryofthepatient’shemody-namichomeostasis.
Itisimportanttonotethatthepatients intheregionalanesthesiagroupreceivedonly onelocalanesthetic(bupivacaine),adminis-teredeitherspinallyorepidurally.Thismakes the regional anesthesia group comparable. However, interestingly, it can at the same timebringsomelimitations.Theuseof20 mgof0.5%bupivacaineasaspinalblockade canresultinaperiodofupto380minutes forcompleteresolutionofanesthesia,while agreaterquantity(150mg)ofthesamesolu-tion,forepiduralblockade,canreachalonger blockadetimeofupto460minutes.10This
wouldcauseapatientwhoreceivedepidural anesthesiatotakelongertorecover,consider-ingtheAldrete-Kroulikcriteria.
Whenthepatientsthatreceivedregional anesthesiawereclassifiedaccordingtowhether they underwent a spinal or an epidural procedure, each subgroup was very small. Surprisingly, it was possible to observe that there were patients with a longer recovery timeafterreceivingspinalbupivacaine(Table 2).Notwithstandingtheseresults,patientsin thepost-anesthesiaunitwiththeirtrunkand legs elevated recovered faster than those in
thesupineposition,eitherafterspinalorafter epiduralanesthesia.
Therearesomelimitationsrelatingtothe retrospective method adopted.This design could have imposed a bias on the results, since the duration of the exposure to the anestheticdrugs,whichwouldprovidebetter controlovertheanesthesiatechnique,wasnot recorded.Toaddressthepossibilitythatthe quantityofanestheticdrugsmightinfluence recoverytime,aprospectiveandrandomized studywouldbringgreaterqualitytofurther investigation. Also, the retrospective collec-tionofdatadidnotallowrandomizationto beperformed,althoughthefinaldistributions ofpatients’positionswerecloseforthesame groupconsidered(regionalorgeneralanesthe-sia).Finally,thetimeintervalsformeasuring theAldrete-Kroulikindex(every30minutes), mighthaveimposedsomedegreeofimpreci-sionontheresults.Ashorterintervalwould allow a more precise determination of the timing of the anesthesia recovery.The fact thatthedatawereretrospectiveandcamefrom thenursingrecordsofAldrete-Kroulikindexes mayhavebluntedtheirprecision.
CONCLUSION
The patient’s body position during the post-anesthesiaperioddidnotinfluencethe recoverytimeatthepost-anesthesiacareunit. There was no difference in the duration of patients’post-anesthesiarecoveryinrelation tousingthesupinepositionorelevatingthe trunkandlegsat30degrees.Thefasterrecov-eryfromgeneralanesthesiacouldbeexpected, giventheAldrete-Kroulikcriteria.
1. TesslerMJ,MitmakerL,WahbaRM,CovertCR.Patientflow inthePostAnesthesiaCareUnit:anobservationalstudy.Can JAnaesth.1999;46(4):348-51.
2. AldreteJA,KroulikD.Apostanestheticrecoveryscore.Anesth Analg.1970;49(6):924-34.
3. PonholdH,VicenziMN.Incidenceofbradycardiaduring recoveryfromspinalanaesthesia:influenceofpatientposition. BrJAnaesth.1998;81(5):723-6.
4. WardRJ,BonicaJJ,FreundFG,AkamatsuT,DanzigerF,
EnglessonS.Epiduralandsubarachnoidanesthesia:Cardio-vascularandrespiratoryeffects.JAMA.1965;191(4):275-8. 5. KehletH.Influenceofregionalanaesthesiaonpostoperative
morbidity.AnnChirGynaecol.1984;73(3):171-6. 6. McHugh GJ, Robinson BJ, Galletly DC. Leg elevation
comparedwithTrendelenburgposition:effectsonautonomic cardiaccontrol.BrJAnaesth.1994;73(6):836-7. 7. KyriakidesZS,KoukoulasA,ParaskevaidisIA,etal.Doespassive
legraisingincreasecardiacperformance?AstudyusingDoppler echocardiography.IntJCardiol.1994;44(3):288-93. 8. WongDH,O’ConnorD,TremperKK,ZacariJ,Thompson
P,HillD.Changesincardiacoutputafteracutebloodlossand positionchangeinman.CritCareMed.1989;17(10):979-83. 9. Kilgour RD, Mansi JA, Williams PA. Cardiodynamic re-sponsesduringseatedandsupinerecoveryfromsupramaximal exercise.CanJApplPhysiol.1995;20(1):52-64. 10. BernardsCM.EpiduralandSpinalAnesthesia.In:BarashPG,
CullenBF,StoeltingRK,editors.ClinicalAnesthesia,4thEd. Philadelphia:LippincottWilliams&Wilkins,2001.Ch.26, p:1-43.AvailableatURL:http://pco.ovid.com/lrppco/index. html,accessedin2003(Aug28).
REFERENCES
SãoPauloMedicalJournal—RevistaPaulistadeMedicina
216
PUBLISHINGINFORMATION
Presented at the 49th Meeting of the Brazilian Society of
Anesthesiology,Joinville,SantaCatarina,2002.
Otávio Omati, MD.In-training resident physician, Anesthesiology Training Center, Hospital das Clínicas, FaculdadedeMedicinadaUniversidadedeSãoPaulo, SãoPaulo,Brazil.
FábioElyMartinsBenseñor,MD,PhD.Supervisorof post-anesthesiacareunit,AnesthesiologyDivision,Hospital dasClínicas,FaculdadedeMedicinadaUniversidadede SãoPaulo,SãoPaulo,Brazil.
JoaquimEdsonVieira,MD,PhD,TSA-SP.Attending physician,AnesthesiologyDivision,HospitaldasClínicas, andcollaboratingprofessor,InternalMedicineDepartment, FaculdadedeMedicinadaUniversidadedeSãoPaulo, SãoPaulo,Brazil.HolderofSuperiorTitleinAnesthesiology (TSA-SP),BrazilianSocietyofAnesthesiology.
Sourcesoffunding:Notdeclared
Conflictofinterest:None
Dateoffirstsubmission:September8,2003
Lastreceived:June22,2004
Accepted:June22,2004
Addressforcorrespondence:
JoaquimEdsonVieira
Av.Dr.Arnaldo,455—Sala1216 SãoPaulo(SP)—Brasil—CEP01246-903 Tel.(+5511)3066-7317
Fax(+5511)3085-0992 E-mail:[email protected]
COPYRIGHT©2004,AssociaçãoPaulistadeMedicina
Aelevaçãodotroncoemembrosinferioresnão influenciatempodepermanêncianaUni-dadedeRecuperaçãoPós-Anestésica
CONTEXTO: A recuperação após anestesia depende de monitorização padronizada e deavaliaçõesindividuais.
OBJETIVO: Investigar a influência do posi-cionamentodopacientesobreotempode recuperaçãopós-anestesiageraleregional.
TIPODEESTUDO:Retrospectivo.
LOCAL: UnidadedeRecuperaçãoPós-Anestési-ca,HospitaldasClínicasdeSãoPaulo. MÉTODOS:Pacientesreceberamcuidadosde
enfermagemsobsupervisãodeanestesiolo- gistanaUnidadedeRecuperaçãoPós-Anes-tésicaquandoemposiçãosupinaoucom troncoepernaselevadasem30grausacada 30minutos.Oiníciodacontagemdetempo foinaadmissãoàunidadeeaúltimamedida foitomadaquandopacienterecebeunota10 naescaladeAldrete-Kroulik.Operíodode tempoatéreceberaltafoiregistrado. RESULTADOS:442pacientesrecuperaram-se
apósanestesiageral(n=274)ouregional (n=168),posicionadosemsupinooucom troncoepernaselevadas.Amedianapara resultados não-paramétricos não mostrou
diferençanotempodepermanênciaquan-doemsupino(75min,n=229)oucom troncoepernaselevados(70min,n=213, p = 0,729). Pacientes recuperaram mais rapidamentedeanestesiaregionalquando comtroncoepernaselevadas(70min)do que em supino (84.5 min) embora sem significância estatística (p = 0,097). Não houvediferençanarecuperaçãodaanestesia geralemqualquerposiçãoinvestigada(70 min,p=0,493).
DISCUSSÃO:Aelevaçãodaspernasemposição supinapodeaumentaroretornovenosopois aanestesiadoneuro-eixobloqueiaosistema simpáticoeessamanobramostrou-secapaz depromovermelhordébitocardíacoduran-te hipovolemia. Os achados desdepromovermelhordébitocardíacoduran-te estudo nãocomprovamestahipótese.Noentanto, algumaslimitaçõesdesteestudoseaplicam, comoumacoletaretrospectiva,impedindo aleatorização dos grupos de recuperação, bemcomoaausênciaderegistrodotempo deexposiçãoaosanestésicos.
CONCLUSÕES:Nãohouvediferençaparao
tempoderecuperaçãopósanestesiaconside-randooposicionamentodopaciente. PALAVRAS-CHAVE: Anestesia. Período de
recuperação da anestesia. Modalidades de posição.Decúbitodorsal.Anestesiageral.
RESUMO