REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
Official Publication of the Brazilian Society of Anesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Bacterial
colonization
due
to
increased
nurse
workload
in
an
intensive
care
unit
Ilker
Onguc
Aycan
a,∗,
Mustafa
Kemal
Celen
b,
Ayhan
Yilmaz
c,
Mehmet
Selim
Almaz
d,
Tuba
Dal
e,
Yusuf
Celik
f,
Esef
Bolat
gaDepartmentofAnestesiologyandReanimation,DicleUniversityHospital,Diyarbakir,Turkey bDepartmentofInfectionDiseases,DicleUniversityHospital,Diyarbakir,Turkey
cDepartmentofAnestesiologyandReanimation,WomenHealthandGynecologicalHospital,Diyarbakir,Turkey dAnestesiologyandReanimation,LiceStatesHospital,Diyarbakir,Turkey
eDepartmentofMicrobiology,DicleUniversityHospital,Diyarbakir,Turkey fDepartmentofBiostatistic,DicleUniversityHospital,Diyarbakir,Turkey
gDepartmentofAnestesiologyandReanimation,BozokUniversityHospital,Yozgat,Turkey
Received7April2014;accepted2May2014
Availableonline2June2014
KEYWORDS
Understaffing; Workload; Nurse; Multiresistant bacteria
Abstract
Introduction:Theratesofmultiresistantbacteriacolonizationorinfection(MRB+)development inintensive care unitsarevery high. The aimofthis study was todetermine thepossible associationbetweentheriskofdevelopmentofnosocomialinfectionsandincreaseddailynurse workloadduetounderstaffinginintensivecareunit.
Methods:Weincluded168patients.Intensityofworkloadandappliedprocedurestopatients werescoredwiththeProjectdeRecherchéenNursingandtheOmegascores,respectively.The criteriausedforinfectionswerethosedefinedbytheCentersforDiseaseControl.
Results:Ofthe168patients,91(54.2%)werefemaleand77(45.8%)weremalepatients.The meanageoffemaleandmalewas64.9±6.2yearsand63.1±11.9years,respectively.Themean durationofhospitalizationinintensivecareunitwas18.4±6.1days.Multiresistantbacteria wereisolatedfromculturesof39(23.2%)patients.ThedevelopmentofMRB+infectionwas correlatedwithlengthofstay,Omega1,Omega2,Omega3,TotalOmega,dailyPRN,andTotal PRN(p<0.05).TherewasnocorrelationbetweendevelopmentofMRB+infectionwithgender, ageandAPACHE-IIscores(p>0.05).
Conclusion:Theriskofnosocomialinfectiondevelopmentinanintensivecareunitisdirectly correlated with increasednurseworkload,applied intervention,and lengthofstay. Under-staffing in the intensive care unit is an important health problem that especially affects care-needingpatients.Nosocomialinfectiondevelopmenthaslaidaheavyburdenonthe econ-omyofmanycountries.Tocontrolnosocomialinfectiondevelopmentintheintensivecareunit, nurseworkload,staffinglevel,andworkingconditionsmustbearranged.
©2014SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](I.O.Aycan). http://dx.doi.org/10.1016/j.bjane.2014.05.005
PALAVRAS-CHAVE
Faltadepessoal; Cargadetrabalho; Enfermagem; Bactérias multirresistentes
Colonizac¸ãobacterianaporcausadoaumentodacargadetrabalhodaequipede
enfermagememunidadedeterapiaintensiva
Resumo
Introduc¸ão: Astaxasdedesenvolvimentodeinfecc¸ãooucolonizac¸ãoporbactérias multirre-sistentes(BMR+)emunidadesdeterapiaintensivasãomuitoelevadas.Oobjetivodesteestudo foideterminarapossívelassociac¸ãoentreoriscodedesenvolvimentodeinfecc¸õeshospitalares eoaumentodacargadetrabalhodiáriadaequipedeenfermagemdevidoàinsuficiênciade pessoalemunidadedeterapiaintensiva.
Métodos: Centoesessentaeoitopacientesforamincluídos.Ovolumedacargadetrabalhoeos procedimentosrealizadosempacientesforamavaliadoscomousodeinstrumentosdemedidas como oProjetodePesquisaem Enfermagem(ProjectdeRecherchéenNursing)eoOmega, respectivamente.Oscritériosusadosparadefinirinfecc¸õesforamosdefinidospelosCentrosde ControledeDoenc¸as.
Resultados: Dos168pacientes,91(54,2%)eramdosexofemininoe77(45,8%)dosexo mas-culino. As médias das idades de mulheres e homens foram 64,9±6,2 e 63,1±11,9 anos, respectivamente. A média do tempo de internac¸ão em unidade de terapia intensiva foi de 18,4±6,1dias. As bactérias multirresistentesforamisoladas apartir de culturasde 39 (23,2%)pacientes.Odesenvolvimentodeinfecc¸ãoporBMR+foicorrelacionadocomtempode internac¸ão,Omega1,Omega2,Omega3,Omegatotal,PPEdiárioePPEtotal(p<0,05).Não houvecorrelac¸ãoentredesenvolvimentodeinfecc¸ãoporBMR+egênero,idadeeescoresno APACHE-II(p> 0,05).
Conclusão:Oriscodedesenvolvimentodeinfecc¸ãohospitalaremunidadedeterapia inten-sivaestádiretamenterelacionadocomoaumentodacargadetrabalhodeenfermagem, as intervenc¸õespraticadaseotempodeinternac¸ão.A faltadepessoalemunidade deterapia intensiva é um problema de saúde importante que afeta principalmente os pacientesque requeremcuidados.Ainfecc¸ãohospitalarcolocouumfardopesadosobreaeconomiademuitos países.Paracontrolarodesenvolvimentodeinfecc¸ãohospitalaremUTI,acargadetrabalho deenfermagem,acomposic¸ãodopessoaleascondic¸õesdetrabalhodevemserorganizadas. ©2014SociedadeBrasileira deAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Nosocomialinfections(NIs)arecommonlyobservedin inten-sivecareunits(ICUs).Recommendedconductstoavoidand control the spread of NI have been published, including measurestomakeitasmultiresistantbacteria(MRB).1,2NI
havewell-documentedadverseeffectsonattributable mor-talityandmorbidity,lengthofstay(LOS),andhospitalcosts. Fewerdataareavailableontheeffects ofNIonworkload of nurses. Moststudies of extra costs relatedto personal charges based their cost estimates on the attributable excessofhospitalLOS.3---7AlthoughtheincreaseinLOS
asso-ciatedwithNI is an importantprovenance ofextra costs, itfailstoreflecttheeffectsofNIonthedailyworkloadof nursesandthereforeisnotenoughfordeterminingstaffing requirements.
EvaluationoftheeffectsofNIonnurseworkloadis dif-ficultbecausetherelationbetweenthesetwoparameters is complex. Understaffing and a compact nurse workload can be viewed as a risk factor for NI or as an effect of NI.
Ononehand,excessivenurseworkloadshavebeenshown tocontributetorecurrentNIoutbreaks;moreover,ina cer-tainpatients,apersistentlyhighleveloftherapeuticactivity maybearisk factor forNI.8---10 On theother hand,NI can
increase the severity of illness in the patient, and con-sequently the level of therapeutic activity, and requires stepped-upinfection control procedures, especially when thecausativeorganismisanMRB,bothaddingtothenurse workload.10 These aspectsofthedailyworkloadshouldbe
consideredwhenthequestistomatchstaffingpatternsto boththenumberofpatientsandthelevelofcare ineach patient.Thescoringsystemsableofmeasuringtheseaspects areneeded.
Theaimofthisstudywastodeterminethepossible asso-ciationbetweentheriskofdevelopmentofNIsandincreased daily nurse workload due tounderstaffing in ICU, and to findoutthe risk factors in developmentof MRB coloniza-tion in patients withand without MRB colonization using Omegascore10 andProjectdeRecherchéenNursing(PRN)
systems.11
Methods
Table1 TheOmegascoringsystem.
Items Points
Category1
Tracheotomy 6 Chesttubes 6 Trainingforhomemechanicalventilation 6 Centralvenouscatheter 3 Arterialline 3 Pulmonaryarterycatheter 6 Temporarycardiacpacing 3 Nasotrachealororotrachealintubation 6 Cardioversionanddefibrillation 3 Cardiacarrest 10 Vasoactivedruginfusion 6 Fibrinolysis 10 Inrta-aorticballoonandcounterpulsation 10 Infusionsofbloodproducts 10 Gastriclavage 1 Parenteralnutrition 6 Balloontamponadeofgastroesophageal
varices
3 Enteralnutrition 3 Ascitesreinstallation 10 Arteriovenousbypass 10 Ureteralcatheter 3 Percutaneouscystostomy 1 Complexorthopedictraction 6 Neurologicalexamination 1 Lumbarpuncture 1 Intracranialpressuremonitoring 3 Infusionofsedativedrugs 6 Peritoneallavage 3
Category2
Hemodialysis,extracorporealcirculation 10 Plasmapheresis 10 Bronchoscopy 3 Gastrointestinalendoscopy 3 Ultrasonography 3 Angiography 10 Scintigraphy 6 Intrahospitaltransport 3 Preparationforout-of-hospitaltransport 1 Preparationforandtransporttothe
operatingroom
6
Category3
Continuousintensivecareunit surveillance
4 Mechanicalventilation 10 Continuoushemofiltration 10 Peritonealdialysis 10 Digestivefluidreinstallation 6 Complexsurgicaldressings 6 Isolation 10
wasapproved (14.07.2013/141) by the Ethical committee ofBozokUniversity.AllpatientsadmittedtotheICUduring the6-monthstudyperiod.168patients[91(54.2%)female, 77(45.8%)male]wereincludedinthestudy.
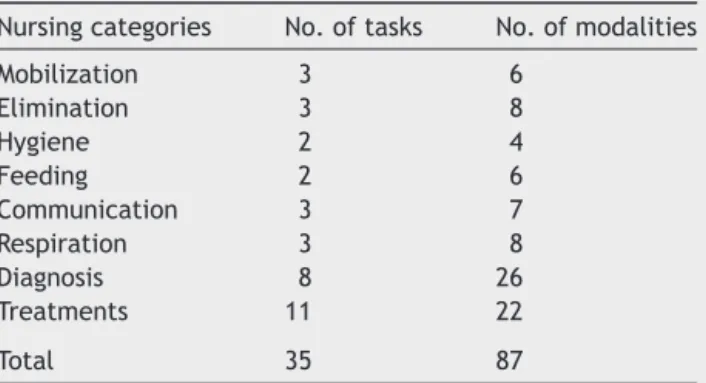
Table 2 The Simplified PRN for intensive care unit patients.
Nursingcategories No.oftasks No.ofmodalities Mobilization 3 6
Elimination 3 8 Hygiene 2 4 Feeding 2 6 Communication 3 7 Respiration 3 8 Diagnosis 8 26 Treatments 11 22 Total 35 87
Modalities:ineachnursingcategory,theweightofagiventask mayvaryaccordingtothenumberoftimesthetaskisperformed eachdayandthenumberofnursesneededtoperformthetask.
Patientswereseparatedintotwogroups,basedonMRB colonization or infection. MRB colonization (MRB+ group) wasdefinedasrecoveryofanMRBfromanyclinicalsiteat admissionorduringtheICUstay.Thecriteriausedfor infec-tionswerethosedefinedbytheCentersforDiseaseControl. MRBaredefinedasmicroorganismsthatarepredominantly bacteria,thatareresistanttooneormoreclassesof antimi-crobial agents(ceftazidime-resistantPseudomonas aerogi-nosa and Acinetobacter baumannii, methicillin-resistant Staphylococcusaureus,methicillin-resistantStaphylococcus spp., vancomycin-resistantEnterococcus,andbeta-lactam producingEnterobactericeae,etc.).NIsweremonitoredby a Nosocomial infection control team. Periodic screening cultures wereperformed on all patients at ICU admission andweeklythereafter.Consequently,itisunlikelythatany episodeofMRBcolonizationorinfectionweremissed.The patients whowere admitted to the ICU during the study periodandwhohadnegativetestsforMRBsconstitutedthe MRB(−)group.
For each patient, the following data were recorded: socio-demographicdata,primarydiagnosis,anddatesofICU admissionanddischarge.Theseverityofillnesswas evalu-atedbasedontheAPACHE-IIcalculatedduringthefirst24h ofICUstay.Nursesworkintwoshifts---nightanddayshifts ---generallyintheICU.Twonursesworkintheday-timeshift (between 8:00AM and 4:00PM) and onein the night-time shift(4:00PMand8:00AM).
TherapeuticandnursingactivityduringthecompleteICU staywasestimatedusingtheOmegascoreandthePRN sys-tem.Moreover,weperformedaspecificfunctionalanalysis ofrecommendedproceduresformanagingMRBnosocomial colonizationorinfection.
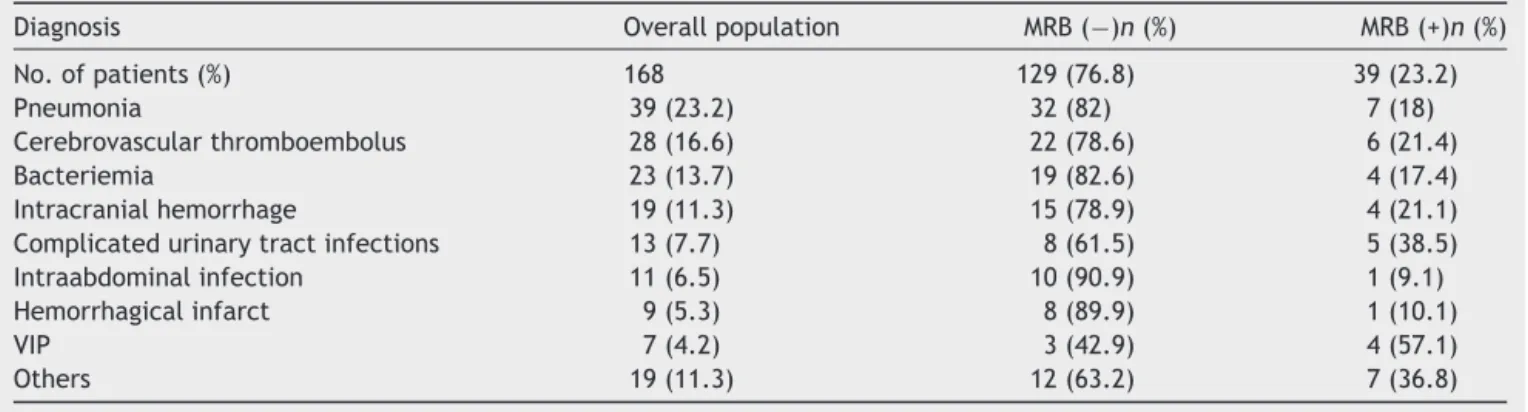
Table3 Primarydiagnosisinthestudypopulation.
Diagnosis Overallpopulation MRB(−)n(%) MRB(+)n(%) No.ofpatients(%) 168 129(76.8) 39(23.2) Pneumonia 39(23.2) 32(82) 7(18) Cerebrovascularthromboembolus 28(16.6) 22(78.6) 6(21.4) Bacteriemia 23(13.7) 19(82.6) 4(17.4) Intracranialhemorrhage 19(11.3) 15(78.9) 4(21.1) Complicatedurinarytractinfections 13(7.7) 8(61.5) 5(38.5) Intraabdominalinfection 11(6.5) 10(90.9) 1(9.1) Hemorrhagicalinfarct 9(5.3) 8(89.9) 1(10.1) VIP 7(4.2) 3(42.9) 4(57.1) Others 19(11.3) 12(63.2) 7(36.8)
MRB,multiresistantbacterialcolonization.
carefully individualized,described, and weighted. Afixed valueisassignedtoeachtask(onepointisequalto5min). Thetimeneededtocompleteeachtaskrightlywas deter-minedbyDelphiconsensus.Thetimesforroutineinfection controlpracticesusedin allpatientsareincluded ineach task.Itemsareenteredeitherdailyor eachtimetheyare carriedout.
Data management and analysis were done using SPSS 11.5 software (SPSS Inc., Chicago, IL, USA). Results wereexpressedasmeans±standarddeviations.Continuous variablesinthetwounmatchedgroupswerecomparedusing theunpairedStudent’sttest.Fordatathatwerenot nor-mally distributed, the nonparametric Mann---Whitney test wasused.p valuesless than0.05 wereconsidered as sig-nificant.
Results
Ofthe168patientscontainedinthestudy91(54.2%)were femaleand77(45.8%) weremalepatients. Themeanage ofthe femaleandmalepatientswas64.9±6.2 yearsand 63.1±11.9 years, respectively. The mean times of hospi-talizationperiodinICUwere18.4±6.1days.Thepatient’s primary diagnosis and indication for hospitalization are demonstratedin Table 3. Foreach patient, thescreening testsandculturesofblood,urine,feces,andendotracheal tubewereperformedafteradmissiontoICUandeachweek thereafter.In39(23.2%)culturestakenfromthepatients, MRB(+)weredemonstrated(Table3).
The mean timeof LOS for MRB-colonized andMRB (−) patients in ICU was 22.3±10.8 days and 14.2±7.1 days, respectively.ThusthedevelopmentofMRBcolonizationwas correlatedwithLOS(p=0.001).
Total Omega score was 21±9.1 in the MRB-colonized patient group, while in MRB (−) patient group it was 10.3±2.1(p=0.003).TotalPRNscoreinMRB-colonizedand MRB(−)patientgroupwasfoundas1519±103and719±52, respectively(p=0.012).
The developments of MRB(+) colonization or infection inpatientswerecorrelatedwithLOS,Omega 2,Omega3, TotalOmega,dailyPRN,andTotalPRN(p<0.05).Therewere nocorrelationsbetweenthedevelopmentofMRB(+) infec-tionwithgender, age, andAPACHE-II andOmega 1 scores (p>0.05).InthePRNsystem,thecomparisonofthe work-loadofnurses revealedthat intheMRB colonizedpatient grouptheworkloadof nurseswassignificantlyhigherthan theoneintheMRBpatient(−)group(p<0.001)(Table4).
PNR score consist of four parts that the nurse should practice:
1. Isolationofthepatient
2. Cleaningwithantisepticsolution 3. Changingbedcovers
4. Collection of blood, urine and other specimens for culture
On the whole,the functionalanalysis showedthat the amountoftimeneededeachdaytocarryoutMRB(−)driven
Table4 ComparisonbetweentheMRB(−)andMRB(+)groups.
No.ofpatients MRB(−)(n=129) MRB(+)(n=39) p
Age 63.1±11.8 64±9.4 0.078 APACHE-II 22±8.9 24±6.1 0.054 LOS(days) 14.2±7.1 22.3±10.8 0.013 Omega1 3.5±0.9 4.9±1.6 0.081 Omega2 6.1±1.1 9.4±4.2 0.022 Omega3 0.9±0.3 3.1±2.1 0.009 TotalOmegascore 10.4±1.2 17.2±7.4 0.017 TotalPRNscore 719±52 1519±103 0.039 DailyPRNscore 50±3.4 68±8.9 0.041
taskswas88minperpatient.Mostofthetimewasspenton isolationprecautionsandantisepticbaths.InourICU,three nurses,twoduringthedaytimeandoneduringthenight, areondutyeachday.Themeancaretime,nursesspentfor MRB(−)patients, was88min, where asit was62min for MRB-colonizedpatients.
Discussion
Toavoidhighratesofnosocomialcolonizationorinfections withresistantbacteriaobservedinICUs,themechanismof infectiondevelopmentshouldbeinvestigated.Eradication ofinfection developmentseemsreasonable than manage-mentofNIinfectionsasNIdevelopmentincreasesmorbidity andmortalityaswellasLOS andincreasesthecosts. The understaffingandincreasedworkloadof nursesis afactor thatconcomitantlyincreasestheNI.
In literature there arefew studies on the relationship betweennurseworkloadandNIdevelopment.Manystudies havedeterminedthatinclinedLOSratherthanstaffsalaries layaheavyburdenonthecountries’economy.The appro-priate numberof nurses staffing in the ICU would reduce NIdevelopmentandthecostsinthelongerterm.Increased intensityofworkloadofthenursesandunderstaffingisalso ariskfactorforNI.Excessworkloadwouldcausedelaysin patient-carewhichresultsinanincreaseindevelopmentof hospitalinfections.Haleyis thefirstonethatemphasized onthistopic. Hehaddetermined thatstaphylococcal epi-demicininfantsintheICUisrelatedtostaffinsufficiency. InanotherstudyTauntonetal.demonstratedacorrelation betweenurinarytractandsepsisinemergencyroomandICU withincreasedworkloadduetonurse’sabsenteeismwithout excuse.12
In a study which has been conducted on 177 patients during an eightmonths period,13 interventionsapplied to
thesepatientswereevaluatedwithOmega 1,2and 3.As aresult,therelationshipbetweenMRB(+)NIdevelopment andOmega2,3andtotalOmegascores werefound tobe statisticallysignificant(p<0.05).13Inourstudywealsoused
Omegascoretoassesstreatment andinterventionapplied to patients. We found out that there was a statistically significant correlation between MRB (+) NI development andOmega2,3andTotalOmega(p=0.001).Interventions appliedto patients were found to be a risk factor for NI development.
Girou et al.14 determined a relationship between NI
development with LOS and inclined treatment activity. Treatmentactivityandtreatmentandinterventionapplied topatients wereevaluated withTherapeuticIntervention ScoringSystem(TISS)andOmegascore.
Fridkin showed that in central venous catheter-associated bloodstream infection risk is related to patient/nurse ratio.15 In our study 26 (18.8%) of the 138
patients demonstrated MRB-colonization in neurology ICU relatedtoincreased nurse workload.Increase in NIs with MRB-colonizationwererelatedwiththeperiodofincreased workloadofnurses,elongatedLOSandincreasednumberof interventions.
PRN system is an effective activity in assessment of nurseworkload.InhisstudyPittetdemonstratedthat dur-ing periods when the nurse workload increased or when
there was understaffing of nurses, NI frequency was also increased.16Therearemanyscoringsystemsforassessment
ofhealthstaffworkload.InourstudyweusedPRNsystem. The staffnurses were listed. The dutiesfor each patient werenoted.InthePRNsystem,maximumcaretimeforeach patient in optimal circumstances wassuggested tobe up to745min.
Saulnieretal.13 reportedthatmeancaretimeforeach
patient was245min. In the same study,there wasa sta-tistically significant correlation between daily and Total PRN with MRB (+) NI development. It was seen that MRB (+) NI development increased while total and daily PRN incline. Likewiseinourstudy therewasdirectcorrelation betweentotalanddailyPRNandMRB(+)NIdevelopment. Duringinclination periodin PRN,MRB (+)NI development was increased too (p=0.001). It was seen that as the nurseworkloadincreased,thecareperiodforeachpatient decreased.
Robertet al. examined nosocomial bloodstream infec-tions in surgery intensive care related to increasednurse workload for a period of eight months. In this study, 28 patients withNI werecompared withthe data of control group composedof 90 patientswho werehospitalizedfor more than3 daysin thesame ICU. Elongatedintravenous catheter usage, total parenteral support and declined nurse/patient ratio were found to be correlated with NI development.17Likewise,inourstudy,timesofnurse
under-staffinginourICUwerecorrelatedwithincreaseintherisk ofNI.
Onthewhole,theTISSandOmegascoresassessthenurse workloadassociatedwithtechnicalproceduresandare sen-sitivetoapossibleincreaseintheseverityofillnessdueto MRB NI.The PRN system, butnot theTISS or the Omega, takesintoaccountroutineinfectioncontrolproceduresand basiccare.Thesethreetoolsunderestimatethedaily work-loadrelated tonursing proceduresnowrecommendedfor MRBinfected ICU patients.This workloadcan beassessed byafunctionalanalysisofcare,asillustratedinthisstudy. Theresultsmayvaryacrossunits;inparticular,theymaybe sensitivetostudydesignandequipment.
As reported fromthe studies, in orderto offera high qualityserviceinICU,toreachanadequate nursestaffing level and a standard ratio of nurse/patient is mandatory. Theroleofnurseunderstaffinginnosocomialviral gastroin-testinalinfections onageneralpediatricswardnursewas evaluatedin onestudy and determinedthat nurse absen-tees ina neonatalICUmay yieldNI epidemics.18 Similarly
inanotherstudyinEngland,ithasbeendemonstratedthat thequalityofservicetocare-neededpatientswasincreased withinclinedstaffinglevelsanddeclineinnurseworkload. Inclinedstaffinglevelsanddeclineinnurseworkloadwould contributeincontrollingNI.19
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.GarnerJS, the Hospital Infection Control Practices Advisory Committee.Guideline for isolation precautions in hospitals. InfectControlHospEpidemiol.1996;24:24---52.
2.Hospital Infection Control Practices Advisory Committee (HICPAC).Recommendationsforpreventingthespreadof van-comycinresistance. Infect Control HospEpidemiol. 1995;16: 105---13.
3.Spengler RF, Greenough WB. Hospital costs and mortality attributedtonasocomialbacteremias.JAMA.1978;240:2455---8. 4.LandrySL,KaiserDL,WenzelRP.Hospitalstayand mortality attributedtonoscomialenterococcalbacteremia:acontrolled study.AmJInfectControl.1989;17:323---9.
5.Durand-ZaleskiI.Estimatingthecostofintensivecare.Intensive CareMed.1994;20:538---9.
6.Coello R, Gleinster H, Fereres J, et al. The cost of infec-tion in surgical patients: case---control study. J Hosp Infect. 1993;25:239---50.
7.KappsteinI,SchulgenG,BeyerU,etal.Prolongationofhospital stay and extra costs due to ventilator-associated pneumo-niainanintensivecare unit.EurJClinMicrobiolInfect Dis. 1992;11:504---8.
8.SaulnierF,GrandbastienB,PoissonC,etal.Consequencesde lamulti-resistancebacterienneenReanimation srladureede sejouretlachargeensoins.ReanUrg.1997;6:213---22. 9.Haley RW, Cushion NB, Tenover FC, et al. Eradication of
endemicmethicilin-resistantStaphylococcusaureusinfections
fromaneonatalintensivecareunit.JInfectDis. 1995;171:614---24.
10.Sociétéderéanimationdelalanguefranc¸aise.Scored’activité Oméga.GuidedesOutilsd’évaluationenRéanimation.Paris, France:Arnette;1995.p.39---44.
11.SaulnierF,DuhammelA,DescampsJM,etal.Indicateursimplifié delachargeensoinsspécifiquealaréanimation:lePRNréa. ReanUrg.1995;4:559---69.
12.TauntonRL,KleinbeckSVM,StaffordR,etal.Patientoutcomes. Aretheylinkedtoregisterednurseabsenteeism,separation,or workload?JNursAdm.1994;24:48---54.
13.SaulnierF,HubertH,OnimusT,et al.Assessingexcessnurse workloadgeneratedbymultiresistantnasocomialbacteriain intensivecare.InfectControlHospEpidemiol.2001;22:273---8. 14.GirouE,StephanF,NovaraA,etal.Riskfactorsandoutcomeof nosocomialinfections:resultsofamatchedcase---controlstudy ofICUpatients.AmJRespirCritCareMed.1998;157:1151---8. 15.FridkinSK,PearSM,WilliamsonTH,etal.Theroleof
under-staffing in central venous catheter-associated bloodstream infections.InfectControlHospEpidemiol.1996;17:150---8. 16.Pittet D,TouveneauS, PaccaudU, etal. Infectionsacquises
enreanimationetsurchargeensoins.In:7emeCongressde I’AssociationLatinepourI’analysedessystemesdeSante.1996. p.301---4.
17.RobertJ,FridkinSK,BlumbergHM,etal.Theinfluenceofthe compositionofthenursingstaffonprimarybloodstream infec-tionratesinasurgicalintensivecareunit.InfectControlHosp Epidemiol.2000;21:12---7.
18.StegengaJ,BellE,MatlowA.Theroleofnurseunderstaffingin nosocomialviralgastrointestinalinfectionsonageneral pedi-atricsward.InfectControlHospEpidemiol.2002;23:133---6. 19.Hurst K. Relationships between patient dependency, nursing