www.jped.com.br
ORIGINAL
ARTICLE
Magnetic
resonance
enterography
in
pediatric
celiac
disease
夽
Gonca
Koc
a,∗,
Selim
Doganay
a,
Eylem
Sevinc
b,
Kemal
Deniz
c,
Govind
Chavhan
d,
Sureyya
B.
Gorkem
a,
Neslihan
Karacabey
e,
Mehmet
S.
Dogan
a,
Abdulhakim
Coskun
a,
Duran
Aslan
eaErciyesUniversityFacultyofMedicine,DepartmentofPediatricRadiology,Kayseri,Turkey
bKayseriResearchandTrainingHospital,Emel-MehmetTarmanChildren’sHospital,DepartmentofPediatricGastroenterology,
Kayseri,Turkey
cErciyesUniversityFacultyofMedicine,DepartmentofPathology,Kayseri,Turkey
dUniversityofToronto,TheHospitalforSickChildrenandMedicalImaging,DepartmentofDiagnosticImaging,Toronto,Canada eErciyesUniversityFacultyofMedicine,DepartmentofPediatricGastroenterology,Kayseri,Turkey
Received15June2016;accepted3November2016 Availableonline31January2017
KEYWORDS Celiacdisease; Magneticresonance enterography; Pediatrics
Abstract
Objective: Toassessifmagneticresonanceenterographyiscapableofshowingevidence/extent
ofdiseaseinpediatricpatientswithbiopsy-provenceliacdiseasebycomparingwithacontrol group,andtocorrelate themagnetic resonanceenterographyfindingswith anti-endomysial antibodylevel,whichisanindicatorofgluten-freedietarycompliance.
Methods: Thirty-onepediatricpatients(meanage11.7±3.1years)withbiopsy-provenceliac
diseaseand40pediatricpatientsasacontrolgroupwererecruitedinthestudy.Themagnetic resonanceenterographyimagesofbothpatientswithceliacdiseaseandthoseofthecontrol groupwereevaluatedbytwopediatricradiologistsinablindedmannerforthemucosal pat-tern,presenceofwallthickening,luminaldistentionofthesmallbowel,andextra-intestinal findings.Patientchartswerereviewedtonoteclinicalfeatures andlaboratoryfindings.The histopathologicreviewoftheduodenalbiopsieswasre-conducted.
Results: Themeandurationofthediseasewas5.6±1.8years(range:3---7.2years).In24(77%)
ofthe patients,anti-endomysialantibody levels wereelevated(mean 119.2±66.6RU/mL). Magneticresonanceenterographyrevealednormalfoldpatterninallthepatients.Ten(32%) patientshadenlargedmesentericlymphnodes.
夽
Pleasecitethisarticleas:KocG,DoganayS,SevincE,DenizK,ChavhanG, GorkemSB,etal.Magneticresonanceenterographyin pediatricceliacdisease.JPediatr(RioJ).2017;93:413---9.
∗Correspondingauthor.
E-mail:[email protected](G.Koc). http://dx.doi.org/10.1016/j.jped.2016.11.003
414 KocGetal.
Conclusion: Althoughamajorityofthepatientshadelevatedanti-endomysialantibody
lev-elsindicating poordietarycompliance,magnetic resonanceenterographydidnotshow any mucosal abnormality associated with the inability of magnetic resonance enterography to detectmild/earlychanges ofceliacdiseaseinchildren.Therefore,itmaynotbeuseful for thefollow-upofpediatricceliacdisease.
©2017SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/ 4.0/).
PALAVRAS-CHAVE Doenc¸acelíaca; Enterografiapor ressonância magnética; Pediatria
Aenterografiaporressonânciamagnéticanadoenc¸acelíacapediátrica
Resumo
Objetivo: Avaliarseaenterografiaporressonânciamagnéticaconseguecomprovar/mostrara
extensãodadoenc¸aempacientespediátricoscomdoenc¸acelíacacomprovadaporbiópsia com-parandocomumgrupodecontroleecorrelacionarosachadosdaenterografiaporressonância magnéticacomoníveldeanticorpoantiendomísioindicadordedietasemglúten.
Métodos: 31 pacientespediátricos (idade médiaentre11,7±3,1 anos)com doenc¸a celíaca
comprovadaporbiópsiae40pacientespediátricosemumgrupodecontroleforamrecrutados noestudo.Asimagensdaenterografiaporressonânciamagnéticadospacientescomdoenc¸a celíacaenogrupodecontroleforamavaliadaspordoisradiologistaspediátricosàscegaspara o padrão damucosa, presenc¸a de espessamento da parede, dilatac¸ão luminal do intestino delgadoeachadosextraintestinais.Osprontuáriosdospacientesforamrevisadosparaanotac¸ão de características clínicas e achadoslaboratoriais. A avaliac¸ão histopatológicadas biópsias duodenaisfoifeitanovamente.
Resultados: Adurac¸ãomédiadadoenc¸afoi5,6±1,8anos(faixade3-7,2anos).Em24(77%)dos
pacientes,osníveis anticorpoantiendomísioestavamelevados(média119,2±66,6RU/mL). A enterografiaporressonância magnéticarevelouum padrãodepregas normalem todosos pacientes.10(32%)dospacientesapresentaramgânglioslinfáticosmesentéricosaumentados.
Conclusão: Apesar de amaioria dos pacientespossuir níveis elevadosde anticorpo
antien-domísio,indicando umadietapobre, aenterografiaporressonânciamagnéticanão mostrou nenhumaanomalianamucosaassociadaàincapacidadedeaenterografiaporressonância mag-néticadetectaralterac¸õesleves/precocesdedoenc¸acelíacanascrianc¸as.Portanto,elapode nãoserútilnoacompanhamentodadoenc¸acelíacapediátrica.
©2017SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4. 0/).
Introduction
Celiac disease (CD), a malabsorption syndrome with an autoimmune origin, affects approximately 1% of the population.1,2 The incidenceofCD hasincreasedover the
decades,presumablyduetoincreasedexposuretogluten,
awarenessof thebroad spectrumofclinical presentation,
and the availability of sensitive and specific diagnostic
tools.3---6However,the‘icebergmodel’indicatestheextent
ofundiagnosedpopulationwithCD.7Thus,CDrepresentsa
substantialhealthproblemworldwide,affectingbothadults
andthepediatricpopulation.8
In genetically susceptible children, the disease is
triggeredbyexposuretogluten-containingfoods.It
predom-inantlyaffects the duodenumand jejunum; however, the
entiresmallbowelcanbeinvolved.Themucosalchangesare
characterizedby villous atrophy,crypt hyperplasia,
thick-ening of the basement membrane under the surface of
epithelium, reducednumber of goblet cells, and signs of
inflammation.9Theclinicalfeaturesarebroadand
nonspe-cific.The spectrum of clinical presentation in CD maybe
classifiedas:(a)classicalform,relatedwithintestinal
symp-toms and predominantly diagnosed in pediatric patients;
(b) atypicalform,presentationoften withextra-intestinal
symptomssuchasirondeficiency;(c)silent form;and(d)
latentform,patientsareasymptomaticanddiagnosed
dur-ingscreeningduetopresenceoffamilyhistoryorCD-related
conditions, such as type 1 diabetes mellitus, Down
syn-drome,andjuvenileidiopathicarthritis.Inlatentform,the
serologictestsarepositivewhenaccompaniedwitheitherno
histopathologicchangeintheintestineoronlyanincreasein
intraepithelial lymphocytes(Marshstage1).Thepositivity
oftheserologicaltestsincludinganti-endomysial(EMA)and
anti-tissuetransglutaminase(tTG)antibodiesinthecourse
of exposure to gluten-containing food and both
serologi-calandclinicalimprovementfollowinggluten-freedietaid
in making the diagnosis of CD. The definitive diagnosis is
establishedbyendoscopicduodenalorjejunalbiopsy.10
Thecharacteristic imagingfindingof CDis smallbowel
mucosalfoldabnormality,whichincludesbluntingoffolds,
reductioninthenumberofjejunalfolds,andincreaseinthe
numberofilealfoldsdependingontheextentanddegreeof
involvement.Thesemucosalfoldchangeshavetraditionally
been evaluated usingbarium studies. Magnetic resonance
enterography(MRE)isarelativelynewbutwell-established
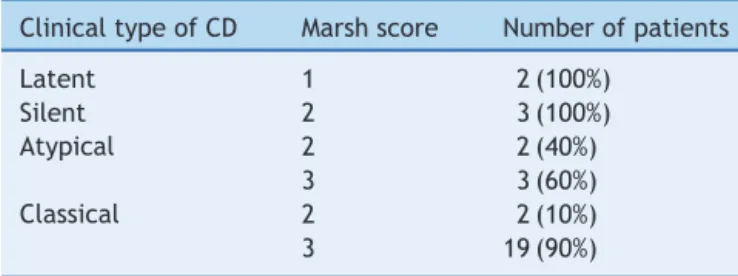
Table1 PatientgroupsaccordingtoMarshclassification.
ClinicaltypeofCD Marshscore Numberofpatients
Latent 1 2(100%)
Silent 2 3(100%)
Atypical 2 2(40%)
3 3(60%)
Classical 2 2(10%)
3 19(90%)
CD,celiacdisease.
ininflammatoryboweldisease.11,12SinceMREenables
visu-alization of theentire small bowel,it has been shown to
bebeneficialindeterminingtheextentofthedisease,
CD-relatedcomplicationsincludingulcerativejejunoileitisand
malignancies,andrefractoryCDinpatientswithpersisting
symptomsdespitegluten-freediet.13---16 However,the
stud-iesfocusedonCDusingMREwereconductedparticularlyin
adultstudygroupsandthereisscarcityofsuchstudiesinthe
literatureevaluatingfindingsofCDbyMREinchildren.17
ThehistopathologicexaminationofthepatientswithCD
does not give sufficient information about the extent of
the disease, since it is confined to duodenum and
proxi-maljejunum.Thus,thepurposeofthisprospective,single
centerstudy wastodetermineifMREis capableof
show-ingextentof thediseaseinpediatric patientswithbiopsy
provenCDbycomparingwithacontrolgroupandcorrelating
theMREfindingswithanti-EMAlevel,whichisanindicator
ofgluten-freedietarycompliance.18
Materials
and
methods
Patients
This studywasapprovedbytheinstitutional reviewboard and is compatible with Declaration of Helsinki. Written informed consent was obtained from the parents of all patients.ItwasconductedbetweenJanuary2014and Jan-uary2015. Thepatients whowerebeingfollowedupwith thediagnosisofCDbythepediatricgastroenterologyclinics ofthisinstitutionwererecruitedinthestudy.Theinclusion criteriaincludedchildrenabove5yearsofagewiththe abil-itytocomplywithbreath-holdinginstructionsandstaystill throughout the procedurewithout need for sedation.The diagnosis of CDwas basedonthe criteriaoutlinedby the EuropeanSocietyforPaediatricGastroenterology, Hepatol-ogy,andNutrition.8
Patientchartreview
Patient charts were reviewed prior to MRE examinations for clinical features and laboratory findings, and subse-quently recorded by a pediatric gastroenterologist (E.S.). Thehistopathologicexaminationsofthepreviouslyobtained (atthetimeofdiagnosis)duodenalbiopsiesofthepatients werere-analyzedby apathologist(K.D.)whowasblinded toclinicalfeatures.Thepatientswerescoredandgrouped accordingtotheMarshclassification,whichisobtainedfrom the histopathologic examination and reflects the severity
of the disease (Table 1). Marsh classification consists of
fourstages(0---3)constructedbasedonseveralfeaturesof
biopsyspecimen:Stage0reflectsnormalbiopsy,whilestage
1,stage2,andstage3 arepredominantly associatedwith
increased intraepithelial lymphocytes, crypt hyperplasia,
andvillousatrophy,respectively.19,9
MRenterographytechnique
Patients were scanned by a 1.5T clinical scanner (Mag-netom, Aera --- Siemens Healthcare; Erlangen, Germany) withan 18-channel body coil. Prior to MRE examination, 24patientswithCD werenon-compliant,whileeightwere compliantwith gluten-freediet. The preparationfor MRE consistedoffastingfor 4---6handadministrationof manni-tolsolution(3%)asanoralcontrastmedium.MREperformed in supine position with the following sequences: Coronal T2-weightedhalf-Fourieracquisitionsingle-shotturbo spin-echo (HASTE) in order to evaluate the distension of the smallintestine,CINEimagingwithcoronalfastimagingwith steady-statefreeprecession(True-FISP),axial(withfat sat-uration)andcoronalTrue-FISP,coronalT2-weightedHASTE with fat saturation, axial single-shot fast spin-echo echo planardiffusionweightedimaging(b=50,400,800s/mm2), and prior to and following, intravenous gadolinium-based contrastmediuminjection(0.1mmol/kg)axialandcoronal 3DT1-weightedvolumetricinterpolatedbreath-hold exam-ination withfat saturation (VIBE). Hyoscine butylbromide (Buscopan;Boehringer ---Ingelheim,Germany)was admin-isteredintravenouslytwiceslowly over 2min at adose of 0.3mg/kg, with a maximum dose of 20mg to eliminate bowelmovementandcontraction;followingtheCINE imag-ingandpriortocontrastagentadministration.Thesequence parametersarepresentedinTable2.
Imageanalysis
TheMREexaminationsof40pediatric patients(meanage: 8.0±1.2years;agerange:5---8.4years),asacontrolgroup, whowerescannedwiththesuspicionofinflammatorybowel diseasebut had normal imaging findings, and thepatient groupwiththediagnosis ofCD wereanonymizedandsent backtoaclinicalpicture-archivingandcommunication sys-tembyapediatricradiologist(M.S.D.)whodidnottakepart intheimageevaluation.
416 KocGetal.
Table2 SequenceparametersofMRIacquisition.
Sequences Parameters
TR(ms) TE(ms) Slicethickness(mm) Gap(mm) FA Matrix
T2HASTE 2000 91 5 1 --- 320×320
True-FISP 3.21 1.04 4 1 50 256×256
T1VIBE 4.36 1.91 3 0 10 256×180
Cinetrue-FISP 3.21 1.04 4 1 50 256×180
Diffusion 6810 62 5 5 --- 256×256
MRI,magneticresonanceimaging;HASTE,half-Fourieracquisitionsingle-shotturbospin-echo;True-FISP,fastimagingwithsteady-state freeprecession;VIBE,volumetricinterpolatedbreath-holdexamination;TR,timeofrepetition;TE,timeofecho;FA,flipangle.
preventoverestimationofthethickness.True-FISPandVIBE sequenceswere notpreferred due tovulnerability tothe blackboundaryartifactthatwouldresultinincorrect mea-surements.The mesenteric lymphnodeswitha short-axis diametermeasuringgreater than1cmwereconsidered as pathologic.
Additionally, the radiologists were asked to rate the images of each patient with an incremental three-point scale(0=inadequate,1=moderate,2=adequate)forsmall boweldistention.
Results
Atotalof45pediatricpatientswiththediagnosisofCDwere recruitedinthestudy initially.Nineofthepatientswhose duodenalbiopsyandhistopathologicexaminationwere car-ried out in another center and five patients who could nottoleratetheMREacquisition(duetoassociatedchronic diseasessuchasIgAdeficiency,Turnersyndrome,type1 dia-betesmellitus,andDownsyndromethatmighthavecaused thepatientstobeincompatible)wereexcluded.
Finally, 31 children with CD (ten boys and 21 girls; meanage11.7±3.1yearsandagerange6---16years)were included.Twenty-one(68%)patientsoutof31were catego-rizedasclassical,five(16%)asatypical,two(6%)aslatent, andthree(10%)assilentCD.Thepresentingsymptomforall thepatientswithclassicalCDwaschronicdiarrhea, abdomi-naldistension,andpain.PatientswithatypicalCDpresented withconstipationandaccompanyingirondeficiencyanemia resistanttooralFe. Therewerenosigns/symptomsofthe patientswithlatentandsilentCD.Theywerediagnosedby screeningconductedduetoincreasedriskforCDbecauseof familyhistory.
The mean duration of the disease was 5.6±1.8 years (range3---7.2years).In24patientswhowerenon-compliant withthegluten-freediet,EMAlevelswereelevated(mean 119.2±66.6RU/mLandrange0---200RU/mL). Inthis insti-tution,anti-EMAlevelsof0---20RU/mLareconsideredtobe withinnormallimitswhilelevelsof21---200RU/mLare con-sideredelevated.Theaveragetimebetweenmeasurement oftheserumEMAlevelandMREexamination was12±3.0 days(range8---16days).PriortoMREexamination,patients withnon-elevatedEMAandtenoutof24patientswith ele-vated EMA were all free of symptoms. Fourteen patients withelevatedEMApresentedwitheitherabdominalpainor diarrhea.Patientdemographicsandlaboratoryfindingsare listedinTable3.
The tworadiologists rated all the examinations of the
patients with CD and the control group as ‘0’: fold
pat-tern wasinterpreted as normalin all the patients. There
wasnoduodenalfoldloss,ilealizationofthejejunum,
jeju-nization ofthe ileum,or global lossof valvulae.The wall
thickness waswithin normal limits (mean: 1.5±0.26 and
1.58±0.28mmforjejunumandileum,respectively).
Abnor-malenhancementordiffusionrestrictionofthebowelwall
wasnotencountered(Fig.1).
Ten patients out of 31 (32%) were detected to have
mesentericlymphnodeswith>1cmshort-axisdiameter.No
otherextra-intestinalabnormalitiesweredetected.
TheradiologistsratedtheimagesofpatientswithCDas
‘adequate’in25(81%)and27(87%)outofthe31
examina-tions(substantialinterreaderagreement,=0.73),andthe
imagesofcontrolgrouppatientsas‘adequate’in34(85%)
and32(80%)outof40,respectively(almostperfect
inter-readeragreement,=0.82),whiletherestwerescoredas
‘moderate’forsmallboweldistention.
Examinations were well tolerated and no significant
adverseeffectsoccurred.
Discussion
This studyperformed toassessMREfindings ofCD in chil-dren did not reveal any imaging abnormalities. Several studies have shown fold pattern abnormalities on imag-ing in patients with uncomplicated CD.20,21 The findings
include decreased number of jejunal folds (<three per
inch) and increasednumber of ileal folds (>five folds per
inch); the combination of these two findings is known as
‘reversedjejunoilealfoldpattern.’Theotherintestinal
find-ings included distention and increased wall thickness of
smallintestine,especiallyaffectingthejejunum.However,
Laghietal.17 andTomeietal.13 havereportedabsenceof
MREfindingsin29%and42%oftheirpatients,respectively,
including adultsand children with biopsy-proven CD. The
current study group, being exclusivelypediatric patients,
may not have developed the intestinal mucosal damage
observed in adult patients. This is supported by the fact
that29% (9/31)ofthe childrenhadmild mucosalchanges
reflectedbyMarshstage1and2,whichmaynotbeshown
byMRE.
Fiveout of 31 (16%) patients in the study group were
diagnosedwitheither latentor silentCD. The
histopatho-logicexaminationoftheduodenalbiopsiesofthesepatients
in
pediatric
celiac
disease
417
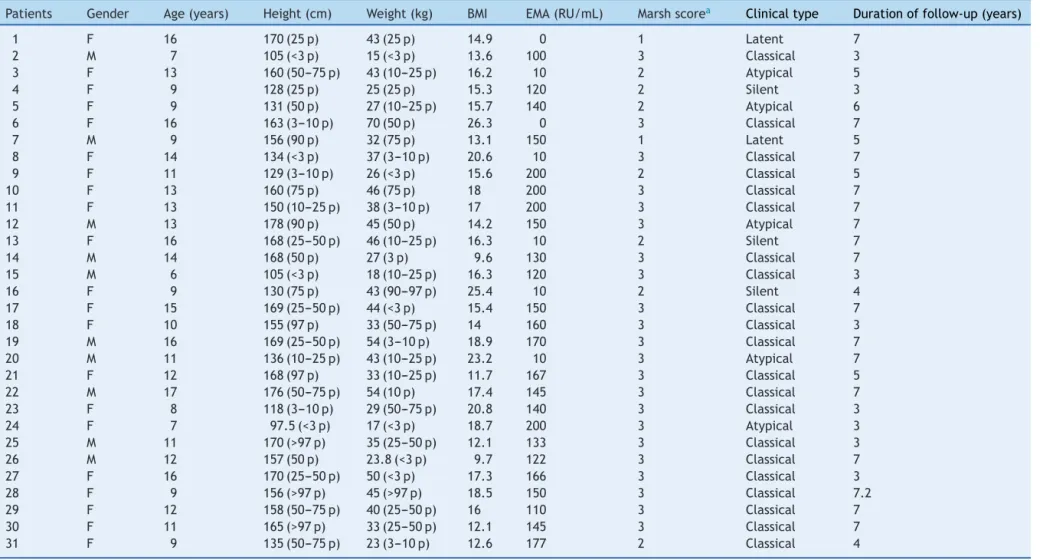
Table3 Clinicalandlaboratoryfeaturesofthestudygroup.
Patients Gender Age(years) Height(cm) Weight(kg) BMI EMA(RU/mL) Marshscorea Clinicaltype Durationoffollow-up(years)
1 F 16 170(25p) 43(25p) 14.9 0 1 Latent 7
2 M 7 105(<3p) 15(<3p) 13.6 100 3 Classical 3
3 F 13 160(50---75p) 43(10---25p) 16.2 10 2 Atypical 5
4 F 9 128(25p) 25(25p) 15.3 120 2 Silent 3
5 F 9 131(50p) 27(10---25p) 15.7 140 2 Atypical 6
6 F 16 163(3---10p) 70(50p) 26.3 0 3 Classical 7
7 M 9 156(90p) 32(75p) 13.1 150 1 Latent 5
8 F 14 134(<3p) 37(3---10p) 20.6 10 3 Classical 7
9 F 11 129(3---10p) 26(<3p) 15.6 200 2 Classical 5
10 F 13 160(75p) 46(75p) 18 200 3 Classical 7
11 F 13 150(10---25p) 38(3---10p) 17 200 3 Classical 7
12 M 13 178(90p) 45(50p) 14.2 150 3 Atypical 7
13 F 16 168(25---50p) 46(10---25p) 16.3 10 2 Silent 7
14 M 14 168(50p) 27(3p) 9.6 130 3 Classical 7
15 M 6 105(<3p) 18(10---25p) 16.3 120 3 Classical 3
16 F 9 130(75p) 43(90---97p) 25.4 10 2 Silent 4
17 F 15 169(25---50p) 44(<3p) 15.4 150 3 Classical 7
18 F 10 155(97p) 33(50---75p) 14 160 3 Classical 3
19 M 16 169(25---50p) 54(3---10p) 18.9 170 3 Classical 7
20 M 11 136(10---25p) 43(10---25p) 23.2 10 3 Atypical 7
21 F 12 168(97p) 33(10---25p) 11.7 167 3 Classical 5
22 M 17 176(50---75p) 54(10p) 17.4 145 3 Classical 7
23 F 8 118(3---10p) 29(50---75p) 20.8 140 3 Classical 3
24 F 7 97.5(<3p) 17(<3p) 18.7 200 3 Atypical 3
25 M 11 170(>97p) 35(25---50p) 12.1 133 3 Classical 3
26 M 12 157(50p) 23.8(<3p) 9.7 122 3 Classical 7
27 F 16 170(25---50p) 50(<3p) 17.3 166 3 Classical 3
28 F 9 156(>97p) 45(>97p) 18.5 150 3 Classical 7.2
29 F 12 158(50---75p) 40(25---50p) 16 110 3 Classical 7
30 F 11 165(>97p) 33(25---50p) 12.1 145 3 Classical 7
31 F 9 135(50---75p) 23(3---10p) 12.6 177 2 Classical 4
418 KocGetal.
Figure1 16-Year-oldfemalepatientwithdiagnosisofceliacdisease;T2-weightedHASTE(A)andT1-weightedfat-saturatedVIBE (B)imagesacquiredfollowingintravenouscontrastadministrationrevealnofoldpatternabnormalitiesoftheintestines.HASTE, half-Fourieracquisitionsingle-shotturbospin-echo;VIBE,volumetricinterpolatedbreath-holdexamination.
that90%oftheirpatientsdiagnosedwithsilentCDhad nor-mal fold pattern. Although there is a limited number of studiesfocusingonMREfindingsofCD,thelargeexperience inCrohn’sdiseasehasrevealedtheinabilityofMREtoexhibit mucosalchanges,butforinflammatorywallinvolvement.22
In accordancewiththis fact, in the current study all the
patients diagnosedwith either silent or latent CD had no
fold pattern abnormalities on MRE. In fact, in this study
that consisted of a majority (68%) of children with the
classical form, no fold abnormalities were seen in any
patients.
Increased levels of EMA were detected in 77% of the
patientspriortoMREacquisition.The antibodiesincluding
EMAandtTGareessentialforthefollow-upofpatientswith
CDandhavebeenreportedtohaveagoodcorrelationwith
gluten-freedietarycomplianceinbothadultandpediatric
patients.23IncreasedlevelsofEMAindicatenon-compliance
of the patient, i.e., not strictly adhering to gluten-free
diet.24 van den Bosch et al. reported a good correlation
betweenresponsetogluten-freedietandenteroclysis
find-ings ascomparedtobiopsy in adultswith CD.23 However,
thereare no such studies related to MRE.An alternative
explanation,atleastinpart,forabsenceofimagingfinding
inpatientswithnormalanti-EMAlevelscouldbeprevention
ofmucosaldamagewithgluten-freediet.
TheextraluminalradiologicmanifestationsofCDinclude
enlarged mesenteric lymph nodes, mesenteric vascular
engorgement, and transient intussusceptions. Enlarged
(>1cmshort-axisdiameter)mesentericlymphnodesarethe
mostcommonextraluminalfindingassociatedwithCD,seen
in up to 42% cases.25 The size of lymph nodes decreases
with treatment with gluten-free diet and their
persis-tence should raise the suspicion of lymphoma.25,26 These
hypertrophiclymphnodesmayactasaninceptionpointfor
intussusception,whichcanbetheinitialpresentationin57%
ofthepatientswithCD.27Mesentericvascularengorgement
isanonspecificsignofthedisease.Whileenlarged
mesen-teric lymph nodes were the only and the most common
extraluminalfindinginthecurrentpatients,intussusception
andvascularengorgementwerenotdetected.
Thisstudyhasafewlimitations.Althoughthetotal
num-berofstudypatientswasrelativelyacceptable,thepatient
group wasdiverse, includingpatientswithclassical,
atyp-ical, silent, and latent CD. Since the both patients with
silentandlatentCDhadlowerMarshscoresassociatedwith
mild mucosal changesthat might have resulted in lack of
MREfindings,astudyconductedwithalarger,homogenized
patient group may be worth further investigation. Since
radiologicalfollow-upwasnotperformed,serialMREimages
acquired at the timeof diagnosis and following initiation
of gluten-freedietwould help assessradiological changes
inthecourseofdisease.Lastly,thehistopathologic
exam-inationoftheduodenal biopsywasperformed atthetime
of diagnosis. The comparisonof recentlyobtained biopsy
resultswithimagingfindingswould enablemaking amore
plausiblehypothesisontherelationofimagingfindingsand
histopathologicchanges.
In conclusion, despite elevated EMA levels in the
majority of children, indicating poor dietary compliance,
this study did not show any significant MRE findings in
biopsy-provenCD,indicatinginabilityofMREtodetectmild
and/or early mucosal damage (suggested by lower Marsh
score)seen inchildren withCD.Therefore,it maynotbe
usefulasadiagnostictestforCDorforfollow-up.However,
as indicated by some authors previously,17 MRE may be
asstrictureandlymphoma,evaluationofCDnon-responsive
togluten-freediet,andtoexcludealternativediagnoses.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.GujralN,FreemanHJ,ThomsonAB.Celiacdisease:prevalence, diagnosis,pathogenesisandtreatment.WorldJGastroenterol. 2012;18:6036---59.
2.DalgicB,SariS,BasturkB,EnsariA,EgritasO,BukulmezA,etal. PrevalenceofceliacdiseaseinhealthyTurkishschoolchildren. AmJGastroenterol.2011;106:1512---7.
3.Kelly CP, Bai JC, Liu E, Leffler DA. Advances in diagno-sis and management of celiac disease. Gastroenterology. 2015;148:1175---86.
4.RiddleMS,MurrayJA,PorterCK.Theincidenceandriskofceliac diseaseinahealthyUSadultpopulation.AmJGastroenterol. 2012;107:1248---55.
5.VilppulaA, KaukinenK, LuostarinenL, KrekeläI,Patrikainen H,ValveR,etal.Increasingprevalenceandhighincidenceof celiacdiseaseinelderlypeople:apopulation-basedstudy.BMC Gastroenterol.2009;9:49.
6.LohiS,MustalahtiK,KaukinenK,LaurilaK,CollinP,Rissanen H,etal. Increasingprevalenceofcoeliacdiseaseover time. AlimentPharmacolTher.2007;26:1217---25.
7.FasanoA,CatassiC.Currentapproachestodiagnosisand treat-mentofceliacdisease:anevolvingspectrum.Gastroenterology. 2001;120:636---51.
8.HusbyS,KoletzkoS,Korponay-SzabóIR,MearinML,PhillipsA, ShamirR,et al. EuropeanSocietyfor Pediatric Gastroenter-ology,Hepatology,andNutritionguidelinesforthediagnosisof coeliacdisease.JPediatrGastroenterolNutr.2012;54:136---60. 9.DicksonBC,StreutkerCJ,ChettyR.Coeliacdisease:anupdate
forpathologists.JClinPathol.2006;59:1008---16.
10.CiclitiraPJ,KingAL,FraserJS.AGAtechnicalreviewonCeliac Sprue.AmericanGastroenterologicalAssociation. Gastroenter-ology.2001;120:1526---40.
11.GrandDJ, GuglielmoFF, Al-HawaryMM. MR enterography in Crohn’sdisease:currentconsensus onoptimal imaging tech-niqueandfutureadvancesfromtheSARCrohn’sdisease-focused panel.AbdomImaging.2015;40:953---64.
12.GücerFI,SenturkS,ÖzkanliS,YilmabasarMG,KörogluGA,Acar M.EvaluationofCrohn’sdiseaseactivitybyMRenterography: derivation and histopathological comparison of an MR-based activityindex.EurJRadiol.2015;84:1829---34.
13.TomeiE,DiacintiD,StagnittiA,MariniM,LaghiA,Passariello R,etal.MRenterography:relationshipbetweenintestinalfold
patternandtheclinicalpresentationofadultceliacdisease.J MagnResonImaging.2012;36:183---7.
14.VanWeyenbergSJ,MeijerinkMR,JacobsMA,vanKuijkC, Mul-derCJ,vanWaesbergheJH.MRenteroclysisinrefractoryceliac disease:proposalandvalidationofaseverityscoringsystem. Radiology.2011;259:151---61.
15.Masselli G, Picarelli A, Gualdi G. Celiac disease: MR enterography and contrast enhanced MRI. Abdom Imaging. 2010;35:399---406.
16.TomeiE,SemelkaRC, BragaL,LaghiA, PaolantonioP,Marini M,etal.Adultceliacdisease:whatistheroleofMRI?JMagn ResonImaging.2006;24:625---9.
17.LaghiA,PaolantonioP,CatalanoC,DitoL,CarboneI,BarbatoM, etal.MRimagingofthesmallbowelusingpolyethyleneglycol solutionasanoralcontrastagentinadultsandchildrenwith celiacdisease:preliminaryobservations.AJRAmJRoentgenol. 2003;180:191---4.
18.Rubio-Tapia A, Murray JA. Classification and management of refractorycoeliacdisease.Gut.2010;59:547---57.
19.MarshMN.Gluten,majorhistocompatibilitycomplex,andthe smallintestine.Amolecularandimmunobiologicapproachto thespectrumofglutensensitivity(‘celiacsprue’). Gastroen-terology.1992;102:330---54.
20.Soyer P, Boudiaf M, Dray X, Fargeaudou Y, Vahedi K, Aout M, et al. CT enteroclysis features of uncomplicated celiac disease: retrospective analysis of 44 patients. Radiology. 2009;253:416---24.
21.MullerWF.Adultceliacdisease.In:SellinkJL,MillerRE,editors. Radiologyofthesmallbowel:modernenteroclysistechnique andatlas.TheHague,TheNetherlands:Nijhoff;1982. 22.TillackC,SeidererJ,BrandS,GökeB,ReiserMF,SchaeferC,
etal.Correlationofmagneticresonanceenteroclysis(MRE)and wirelesscapsuleendoscopy(CE)inthediagnosisofsmallbowel lesionsinCrohn’sdisease.InflammBowelDis.2008;14:1219---28. 23.SugaiE,NachmanF,VáquezH,GonzálezA,AndrenacciP,Czech A, et al. Dynamics of celiac disease-specific serology after initiationof agluten-free diet anduse intheassessmentof compliancewithtreatment.DigLiverDis.2010;42:352---8. 24.vandenBoschHC,Tjon aThamRT,GooszenAW,
Fauquenot-NollenJM,LamersCB.Celiacdisease:small-bowelenteroclysis findingsinadultpatientstreatedwithagluten-freediet. Radi-ology.1996;201:803---8.
25.LohanDG,AlhajeriAN,CroninCG,RocheCJ,MurphyJM.MR enterographyofsmall-bowellymphoma:potentialfor sugges-tionofhistologicsubtypeandthepresenceofunderlyingceliac disease.AJRAmJRoentgenol.2008;190:287---93.
26.Lucey BC, Stuhlfaut JW, Soto JA. Mesenteric lymph nodes seen at imaging: causes and significance. Radiographics. 2005;25:351---65.