RevBrasAnestesiol.2015;65(5):417---420
REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiology www.sba.com.brCLINICAL
INFORMATION
Life-threatening
acute
subdural
haematoma
after
combined
spinal---epidural
anaesthesia
in
labour
Bulent
Bakar
a,∗,
Esra
Ozer
b,
Ismail
Hakki
Tekkok
caDepartmentofNeurosurgery,FacultyofMedicine,KirikkaleUniversity,Kirikkale,Turkey bDepartmentofAnaesthesiologyandReanimation,TOBB-ETUHospital,Ankara,Turkey cDepartmentofNeurosurgery,TOBB-ETUHospital,Ankara,Turkey
Received7February2013;accepted9July2013 Availableonline16October2013
KEYWORDS
Combined spinal---epidural anaesthesia; Labour;
Subduralhaematoma
Abstract
Backgroundandobjectives: Onlyfewreportsinliteraturehavepointedouttothepossibility ofacranialsubduralhaematomaformation associatedwith duralpuncture duringspinal or epidural analgesia. We herein describe such arare case who was diagnosedto have acute subduralhaematomaaftercombinedspinal---epiduralanaesthesiausedinlabour.
Casereport: A34-year-old,primigravidwomenwithagestationof38weeksunderwent cae-sarean sectionundercombinedspinal---epiduralanaesthesiaandgavebirthtoahealthyboy. Thirty-twohoursafterdelivery,hermoderateheadacheprogressedtoasevereheadache asso-ciatedwithnauseaandvomitingandlaterwasmorecomplicatedwithageneralizedtonic---clonic seizureandensuinglethargy.Computedtomographyofthebraindemonstratedaright-sided fronto-temporo-parietalacutesubduralhaematomawithdiffusecerebraloedema.She under-went urgentFTP craniotomyandevacuationofthehaematoma.Early postoperativecranial computedtomography showedacleanoperativesite. Eightdaysafter subduralhaematoma surgery,shebecamelethargicagain,andthistimecranialcomputedtomographydisclosedan extraduralhaematomaundertheboneflapforwhichshehadtoundergosurgeryagain.Two dayslater,shewasdischargedhomewithKarnofskyperformancescoreof90/100.At follow-upexam,shewas neurologicallyintactandhercranialcomputedtomographyandmagnetic resonancewerenormal.
Conclusions: Asconclusion,withtheuseofthiscombinedspinal---epiduralanaesthesia,itshould bekeptinmindthatheadachedoesnotalwaysmeanlowpressureheadacheassociatedwith spinalanaesthesiaandthatacatastrophiccomplicationofsubduralhaematomamayalsooccur. © 2013SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](B.Bakar).
0104-0014/$–seefrontmatter©2013SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
418 B.Bakaretal.
PALAVRAS-CHAVE
Anestesiacombinada raqui-peridural; Parto;
Hematomasubdural
Hematomasubduralagudopotencialmentefatalapósanestesiacombinada raqui-periduralemparto
Resumo
Justificativaeobjetivos: Apenasalgunsrelatosnaliteraturamencionaramapossibilidadede formac¸ão de hematoma subduralcraniano associada à punc¸ãodurante araquianestesia ou anestesiaepidural.Opresenterelatodescreveumcasotãoraroquefoidiagnosticadocomo hematomasubduralagudoapósanestesiacombinadaraqui-periduralusadaemparto.
Relatodecaso:Pacienteprimípara,34anos,com38semanasdegestac¸ão,submetidaà cesar-ianasobanestesiacombinadaraqui-peridural,deuàluzummeninosaudável.Após32horasdo parto,adordecabec¸amoderadadapacienteprogrediuparadordecabec¸aintensaassociada anáuseaevômitoesecomplicousubsequentementecomcriseconvulsivageneralizada tônico-clônica econsequente letargia.Tomografiacomputadorizada docérebro revelouhematoma subduralagudodolado direitoem região frontotemporoparietal(FTP) comedemacerebral difuso.Apaciente foisubmetidaàcraniotomiaFTPdeurgênciaeevacuac¸ãodohematoma. Tomografiacomputadorizadadocrânionopós-operatórioprecocemostrouumsítiooperatório limpo.Oitodiasapósacirurgiadohematomasubdural,apacientevoltouaficarletárgicae, dessavez,atomografiacomputadorizadarevelouumhematomaextraduralsoboretalhoósseo queexigiuoutracirurgia.Doisdiasdepois,apacienterecebeualtahospitalarcomclassificac¸ão dedesempenhoKarnofskyde90/100.Aoexamedeacompanhamento,apacienteapresentou-se neurologicamenteintactaesuatomografiacomputadorizadaeressonânciamagnéticaestavam normais.
Conclusão:Aousaraanestesiacombinadaraqui-periduraldeve-seterem mentequedorde cabec¸anemsempresignificadordecabec¸ahipotensivaassociadaàraquianestesiaequeuma complicac¸ãocatastróficadehematomasubduraltambémpodeocorrer.
©2013SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Today, many anaesthesiologists prefer combined spinal---epidural(CSE)anaesthesiatoavoidfromthepainoflabour. However,this technique bears some unique risks such as itching,nausea,vomiting,maternalhypotension,headache, convulsion, meningitis, toxicity, and even cardiac arrest. Additionally,fewbutrecentreportshavepointedouttothe possibilityofcranial subdural haematomaassociated with duralpunctureduringthespinaland/orepidural anaesthe-siainlabour.1---3Ourcasestudyalsodescribedararecasewho
underwent urgent surgery for acute subdural haematoma occurring32hafterCSEanaesthesiausedinlabour.
Case
history
A 34-year-old, primigravid woman with a gestation of 38 weeks underwent caesarean section for cephalopelvic disproportion and foetal distress. Preoperative laboratory investigationwasnormalexceptrelativethrombocytopenia (90,000/mm3)attotalbloodcount.Surgerytookplaceunder
theCSEanaesthesia,andshegavebirthtoahealthyboy.To performtheCSEanaesthesia,18GTuohyand27Gspinal nee-dlewereinsertthroughtheL4-5interspinousspaceandthen 10mgbupivacaineand25gfentanilwasinfused intrathe-cally.Earlypostoperativeperiodwasuneventfulexceptfor minimal vaginalstaining.Next day, thirty-two hoursafter hersurgery,sheexperiencedaprogressiveheadachearound theneck.Whensheattemptedtomobilizeoutofbed,she
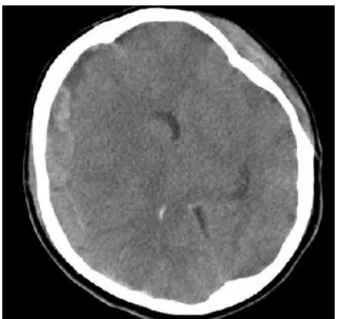
vomitedandsufferedageneralizedtonic---clonicseizureand fellbackonherbed.Aftertheseizure,shebecamelethargic withnoeyeorverbalresponsetopainfulstimuli(Glasgow Coma Score (GCS) E1M5V1-Total 7/15) andthe right pupil was found to be dilated while her breathing was ataxic; and her cardiac rhythm is bradicardic (45min−1). There wasno historyof a previous trauma or a drop attack. An emergent braincomputed tomography (CT)demonstrated aright-sidedfronto-temporo-parietal(FTP)acutesubdural haematomawithdiffuse oedemaof the surroundingbrain (Fig.1).SheunderwenturgentFTPcraniotomy;andacute haematoma was evacuated (Fig. 2). Postoperatively, the patientwassedatedandmechanicallyventilatedfor48hat intensivecareunit(ICU).AtICU,becausethepostoperative controlbloodcountresultshowedseverethrombocytopenia (50,000/mm3),repeateddosesofthestandardplateletwere
Acutesubduralhaematomaaftercombinedspinal---epiduralanaesthesia 419
Figure 1 Preoperative brain computed tomography scan demonstratestherightfronto-temporo-parietalacutesubdural haematomawithdiffusecerebraloedema.
Figure2 Photographtakenintraoperativelyshowstheacute subduralhaematoma.
fullycapable,functional andneurologicallyintactpatient (Karnofsky performance score 100/100). Cranial CT and magneticresonance(MR)scanswerenormal(Fig.3).
Discussion
Thesafetyofthespinalandepiduralanaesthesiaas sepa-ratetechniques hasbeenwell documented.Nevertheless, thereare reports that have pointed tothe fact that CSE anaesthesia during labour may cause hypotension as its immediatecomplication.Thishypotensionthatisprobably causedbyundesiredeffectsofeitherintrathecalopioidsor epidurallocalanaestheticsmayhavetriggeredasecondary intracranialhypotension.4,5 On top of this, as withspinal
and/orepiduralanaesthesia,anintendedoraninadvertent dural puncture may well provoke leakage of the cere-brospinalfluid(CSF) intotheepiduralspace.This leakage alsocauses intracranialhypotension.6 This leakage hence
causescaudal displacement of thecerebral and stretches thebridgingcerebralvessels(especiallythecerebralveins and venules). The walls of these bridging veins are very thinwhentheycoursethroughthesubduralspacealthough theyhave thickerwalls while in the subarachnoidspace. So,itispossiblethateitherhypotensionorthegravitational forcesthat have separated the cortexfromthe overlying duracouldhavecausedaninitialtearwhichcouldhavebeen repairedwitha normalcoagulationsystem.3 On theother
hand,cerebralsubduralhaematomasmayalsooccur spon-taneouslyinparturientwomenwithoutduralpunctureasa consequenceofarapidintracranialpressuredropafterthe Valsalvamanoeuvre.6,7
Acute subdural haematomas have been described as lesions causing signs or symptoms within less than 7 days after the initiation of bleeding.1 Cerebral atrophy,
dehydration,excessiveCSFleakage originatingfromdural puncture(s), anticoagulants, and arteriovenous malforma-tions(AVM) arethoughttobethecontributingfactors for subduralhaematomaformation. Ontheotherhand,itcan be argued that only the largest spinal needle may cause a significant CSF leakage, but Zeidan et al. has reported that mortality was not related to the size of the spinal needleused in CSE and epiduralspinal anaesthesia.8 Our
420 B.Bakaretal.
patient did not use anticoagulant; and her postoperative cranialMRwithgadoliniumrevealednocerebralAVMand/or aneurysm. Furthermore, the anaesthesiologist who per-formed the CSE anaesthesia to our patient reported no excessiveCSFleakageorunexpectedeventduringthe pro-cedures.Additionally,wecouldnotexplaintheaetiologyof thethrombocytopeniainourpatient.
In most cases, a nonpostural headache, changes in headache characteristics (such as resistant headache, retroorbital or frontal headache), vomiting, seizure, and lethargyarealertingsigns.Inthosepatientsincludingthese symptoms, aetiology should be well differentiated; and postduralpunctureheadache,pre-eclampticandeclamptic headache, simple tension or migraine headache, subdu-ral/subarachnoidhaemorrhage,stroke,tumour,meningitis, and cerebral vein thrombosis should be all excluded.1,5
In our patient, headache occurred rapidly within two days after delivery, and it was rapidly complicated with seizure. Differential diagnosis of the seizure in present caseincludeseclampsia,intracranialhaemorrhage,embolic episodes and local anaesthetic toxicity.1 Eclampsia was
excluded,becausenoothersymptomsexceptseizurewere present in our patient.Toxicity could be excluded asthe seizure occurred on the second day. The history wasnot suggestive of the cortical vein thrombosis; and meningi-tiswasexcluded byabsent of neutrophilia,neck stiffness and fever.Additionally, rapid development of the serious neurologicalsymptoms,andtheemergentcranial CTscan performedbyalertedmedicalstaffsconfirmedtheclinical diagnosis.
Treatmentof thesubduralhaematomaincludes conser-vative(medical observation, anti-oedema medication), or surgical(intracranialpressuremonitoring,external ventri-cularCSF drainage,singleor multiple burr-holedrainage, and craniotomy/craniectomy) techniques. Haematomas less than 10mm in width often resolve spontaneously. However, thicker haematomas complicated with reactive cerebraloedemaoftencauseseriousneurologicalsymptoms andrequiresurgical evacuation.Preoperativeneurological conditioncorrelateswiththepostoperativeoutcome.1,5In
ourpatient,wecouldnotclarifytheexactcauseofthe sub-dural haematoma.Surely some CSFleakage occurred and most probably caused a relative intracranial hypotension leadingtostretchingofthebridgingveins.Yettherewasno
Valsalvamanoeuvrelikeinanormallabourthatwouldhave contributed to the increasing volume of the haematoma. Whatever the reason,her subdural haematomawas thick anddenseenoughtobeconsideredforsurgery.
Conclusion
Thiscasedemonstratesanacutesubduralhaematomaafter CSEanaesthesiainapatientwithoutriskfactorsfor bleed-ing.Asconclusion,withtheuseofthisCSEanaesthesia,this rarebutcatastrophiccomplicationofsubduralhaematoma shouldbealwayskeptinmind.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Vaughan DJ, Stirrup CA, Robinson PN. Cranial subdural haematoma associated with dural puncture in labour. Br J Anaesth.2000;84:518---20.
2.KayacanN,AriciG,KarsliB,etal.Acutesubduralhaematoma afteraccidentalduralpunctureduringepiduralanaesthesia.Int JObstetAnesth.2004;13:47---9.
3.BisinottoFM,DezenaRA,FabriDC,etal.Intracranialsubdural hematoma:ararecomplicationfollowingspinalanesthesia:case report.RevBrasAnestesiol.2012;62:88---95.
4.NorrisMC,GriecoWM,BorkowskiM,etal.Complicationsoflabor analgesia:epiduralversuscombinedspinal---epiduraltechniques. AnesthAnalg.1994;79:529---37.
5.AbbinanteC,LautaE,DiVenosaN,etal.Acutesubdural intracra-nialhematomaaftercombinedspinal---epiduralanalgesiainlabor. MinervaAnestesiol.2010;76:1091---4.
6.SharmaS,HalliwellR,DexterM,etal.Acutesubduralhaematoma inthepresenceofanintrathecalcatheterplacedforthe preven-tionofpost-duralpunctureheadache.Anaesth IntensiveCare. 2010;38:939---41.
7.Ramos-ApariciR,Segura-PastorD,Edo-CebolladaL,etal.Acute subdural hematoma after spinal anesthesia in an obstetric patient.JClinAnesth.2008;20:376---8.