RevBrasAnestesiol.2017;67(1):110---113
REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologia www.sba.com.brLETTERS
TO
THE
EDITOR
Post-spinal
hyperacute
subdural
hematoma
Hematoma
subdural
pós-espinal
hiperagudo
DearEditor,
The development of intracranial subdural hematoma fol-lowing spinal anesthesia is a rare (1/1mil---1/1.5mil) and thisseriouscomplicationcan befatal.1,2 Continuous
leak-ageofcerebrospinalfluid(CSF) duetoduralinjuryduring puncture can leadto stretching,tearing, and bleedingin meningealvessels. The symptomsof intracranial subdural hematoma are predisposition to sleeping, disorientation, blurredvision,diplopia,corticalblindness,tinnitus,lossof hearing,scalpparesthesia,vertigo,vomiting,andepileptic convulsions.2,3However,themostcommonsymptomis
head-ache.Theprobabilityofheadachefollowingduralpuncture makesthediagnosisofsubduralhematomamoredifficult.4,5
Nevertheless, the presence of neurological symptoms is pathognomonicandhelpsestablishthedifferential diagno-sis.
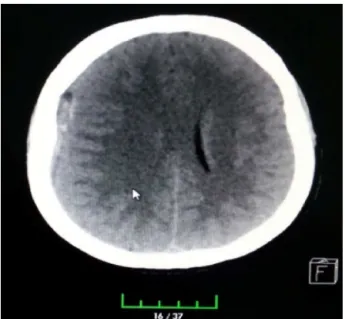
A 50 year-old femalepatient scheduled for totalknee prosthesis hadbeen onmethotrexate for 4 year withthe diagnosisofrheumatoidarthritis.Hemogram,biochemistry, andcoagulationparameterswerenormalwithouther posi-tivehepatitisCmarker.Theoperationwasperformedwith ASA II risk. Standard monitorization (electrocardiogram, pulseoximeter, noninvasive blood pressuremeasurement) was carried out. A 25G spinal needle was used, and the intrathecal space was entered on the second attempt at theL4---L5level, followed byadministration of12.5mgof heavy bupivacaine. The operation was carried out under spinalanesthesiaandlastedafter2h.Thepatientwasthen transferred to the orthopedics ward. The patient devel-opedsuddenlossofconsciousnessapproximately10hpost operation. Upon physical examination, the patient was unconscious,hereyeswereanisocoric,andspontaneous res-pirationwaspresent.GlasgowComaScore(GCS)was7(no responsetoverbalstimuli, localizespainful stimulus)and Babinski reflex was not present. BP was 170/100mmHg, oxygensaturation was 94%,and pulsewas 110bp/m. The patient’srelatives reported thatshe complainedof head-ache and dizziness after the operation. Emergency brain CT scan showed a right subdural hematoma as well as
brain edema and shifting(Fig.1).Emergency decompres-sionwascarriedoutbyneurosurgery(Fig.2).Hemodynamics were stableduring the operation. The patient was awak-ened without any problems. She wasthen extubated and transferred to intensive care. On her postoperative day-1 examination, GCS was 15, but the right eye remained ptotic.Thepatientwasdischarged1weeklater.The devel-opmentofsubdural hematomaafterspinalanesthesiais a rarebutseriouscomplicationofanesthesia.1,2CSFleakage
afterduralinjurycanleadtolowCSFpressureand intracra-nial hypotension, which can cause withdrawn onbridging veinsand,rarely,bleedingassociatedtheruptureof subdu-ralveinsvia thecompensatoryvasodilatationofsecondary veins.6,7Subduralveinsrupturemoreeasilyduetothe
struc-ture of thebridgingvein walls, which aremicroscopically morefragilethanotherveinwalls.
Factorssuchastheuseofanticoagulants,cerebral atro-phy,vascular anomalies,dehydration, pregnancy,multiple penetrationsofthedura,andthicknessoftheneedleused are associated with intracranial bleeding.8 In a series of
35caseswithpost-spinalsubduralhematoma,norisk fac-tor was determined in 15 cases.6 However, the use of a
25Gratherthana27Gspinalneedle,thepresenceof cere-bral vasculitisin rheumatoid arthritispatients rarely, and weakveinwallstructurewereassociated.9Onecasewhere
in thepatienthad norisk factorsand developedsubdural hematomawiththeuseofa27Gneedlehasbeenreported in theliterature.6 Althoughthemost commonsymptom is
headache,thepatientmayalsodevelop vomiting,blurred vision,predispositiontosleep,vertigo,tinnitus,lossof hear-ing,diplopia,andblindness.10Themostimportantfactorin
missedanddelayeddiagnosesofsubduralhematomaisthat itsmostcommonsymptomisheadacheandthemost com-moncomplicationofspinalanesthesiaispost-duralpuncture headache(PDPH).PosturalHeadacheispathognomonicfor PDPH.6 According to the International Headache Society
LETTERSTOTHEEDITOR 111
Figure1 CTscanshowedarightsubduralhematoma.
>5d.6Inastudyincluding640patients,posturalheadache
continuedfor15daysinonepatient,althoughnolesionwas visible in brainMR andthe headacheimproved afteronly twoepiduralpatches.6
In cases where headache is atypical, lasts long, is not associatedwithposture,andisaccompaniedby neurologi-calsymptoms,subduralhematomashouldbesuspectedand neuroimaging shouldbecarriedout fordiagnosis.6
Subdu-ral hematomas appear as hyperdense crescents between boneandbraininCTimaging.Asthedurationofhematoma increases,itsdensity decreases;whenitreachesthesame density asthe brain,diagnosiscan bemadewithMR.The durationofhematomaisdividedintofourgroups:(1) hyper-acute(first24h);(2)acute(2---3d); (3)subacute(3---14d); and(4)chronic(≥2weeks).11Ourcasehadhyperacute
sub-duralintracranialhematoma.
In a study by Amorimet al.,6 the period between the
onsetof symptoms anddiagnosis ranged4h to29 weeks, and themost common symptoms wereheadache (74.3%),
Figure2 Emergencydecompressionbyneurosurgery.
changes in consciousness (40%), vomiting (31%), hemiple-giaorhemiparesia(22%),diplopiaorn.abdusence paresia (14%),and speechdisorders. Inthe present case, diagno-siswasmade10hpost-surgery,andthepatient’ssymptoms wereheadache and loss of consciousness.In the work of Amorimetal.,6subduralhematomadevelopedina
hypera-cutemannerinonlythreecases,andlossofconsciousness occurred in only one of these. Subacute hematoma with loss of consciousness developed in three cases. Subdural intracranial hematoma may spontaneously resorb or may requiresurgicaldecompression orburr-holedrainage.12 Of
21subduralhematomacasesreportedbyKayacanetal.,13
15required surgicaldecompressionandtwopatientswere lost.In a case reported by Ezriet al.,14 chronic subdural
hematomawasspontaneouslyresorbed.Inthepresentcase, surgicaldecompressionwasalsocarriedout.
The most commoncomplication of spinal anesthesiais PDPH.Thedevelopmentofintracranialsubduralhematoma following spinal anesthesia, though rare, is a serious complication that can be fatal if left untreated. Both complicationspresent withheadache,renderingdefinitive diagnosis difficult.2,3 In cases where theheadache is long
induration,is notpostural,andisaccompanied by neuro-logicalsymptoms,subduralhematomashouldbesuspected andneuroimagingshouldbecarriedout.CTorMRIshould beordered dependingon thedurationof theheadache.10
Toavoidmisseddiagnosisofsubduralhematomainthe5---7 daysperiodwhenpost-spinalheadacheispresent,headache shouldbe investigated thoroughly andthe patientshould bemonitoredfor neurologicalsymptoms.Despitethevery lowincidenceofsubdural hematoma,headachesfollowing spinalanesthesiashouldbefullyexaminedandthe possibil-ityofsubduralhematomashouldnotbeunderestimated.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Zeidan A, Farhat O, Maaliki H, et al. Does postdural punc-ture headache left untreated lead to subdural hematoma? Casereportandreviewoftheliterature.IntJObstetAnesth. 2006;15:50---8.
2.Turnbull DK, Shepherd DB. Post-dural puncture headache: pathogenesis, prevention and treatment. Br J Anaesth. 2003;91:718---29.
3.KelsakaE,SarihasanB,BarisS,etal.Subduralhematomaasa latecomplicationofspinalanesthesia.JNeurosurgAnesthesiol. 2003;15:47---9.
4.Blake DW, Donnan G, Jensen D. Intracranial subdural haematomaafterspinal anaesthesia.AnaesthIntensiveCare. 1987;15:341---2.
5.EvansRW.Specialreport:complicationsoflumbarpunctureand theirpreventionwithatraumaticlumbarpunctureneedles52nd AnnualMeetingoftheAmericanAcademyofNeurology;2000.
6.Amorim JA,Remígio DS,Damázio FilhoO, et al.Intracranial subduralhematomapost-spinalanesthesia:reportoftwocases andreviewof33casesintheliterature.RevBrasAnestesiol. 2010;60(620---629):344---9.
112 LETTERSTOTHEEDITOR
of intrathecal drug delivery device. Reg Anesth Pain Med. 2000;25:76---8.
8.ScottDB,HibbardBM.Seriousnon-fatalcomplications associ-atedwithextraduralblockinobstetricpractice.BrJAnaesth. 1990;64:537---41.
9.Watts RA, Mooney J, Lane SE,et al. Rheumatoid vasculitis: becomingextinct?Rheumatology.2004;43:920---3.
10.SrivastavaU,AgrawalA,GuptaA,etal.Intracranialsubdural hematomaafterspinalanesthesia for cesareansection:case reportand reviewof literature.JObstetAnaesth CritCare. 2014;4:45---7.
11.MossD,JalaluddinM.Pediatricsubduralhematoma. In: Bat-jerHH,LoftusCM,editors.Textbook ofneurologicalsurgery. Philadelphia:LippincottWilliams&Wilkins;2003.p.1095---102.
12.Azzarelli B. Neuropathology of the central nervous system: trauma, cerebrovascular disease, infections, demyelinating, neurodegenerative, nutritional and metabolic disorders. In: BatjerHH,LoftusCM,editors.Textbookofneurologicalsurgery. Philadelphia:LippincottWilliams&Wilkins;2003.p.207---33.
13.KayacanN,AriciG,KarsliB,etal.Acutesubduralhaematoma afteraccidentalduralpunctureduringepiduralanaesthesia.Int JObstetAnesth.2004;13:47---9.
14.EzriT,AbouleishE,LeeC,etal.Intracranialsubduralhematoma followingduralpunctureinaparturientwithHELLPsyndrome. CanJAnaesth.2002;49:820---3.
OzkanOnala,∗,EmineAslanlara,SezaApiliogullaria,
OmerFarukErkocakb,JaleBengiCelika
aSelcukUniversityMedicalFaculty,Departmentof
AnesthesiaandIntensiveCare,Konya,Turkey
bSelcukUniversityMedicalFaculty,Departmentof
OrthopedicsandTraumatology,Konya,Turkey
∗Correspondingauthor.
E-mail:[email protected](O.Onal). Availableonline18March2016
http://dx.doi.org/10.1016/j.bjane.2015.04.003
0104-0014/
©2016SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Preventing
atelectasia
at
robotic
surgery
Prevenir
atelectasia
em
cirurgia
robótica
DearEditor,
We read the article ‘‘Robotic prostatectomy: the anes-thetist’sviewforroboticurologicalsurgeries,aprospective study’’ written by Oksarand Ocal witha great interest.1
They share the anesthetic management of the robotic prostatectomy.We wouldlike tothankto theauthors for their contribution witha successfully designed and docu-mentedstudy.Webelievethatthesefindingswillenlighten abouttheanestheticmanagementoftherobotic prostatec-tomy.
Robotic-assisted laparoscopic prostatectomy (RALP) is a technically difficult surgery requiring experience. The duration of the surgery is usually prolonged because of detailedpreparation beforesurgery. The anesthetic man-agementrequiresmoreattentionthanopensurgerydueto pneumo-peritoneum. Prolonged operation time, the tren-delenburgposition,andincreasedintra-abdominalpressure dueto pneumo-peritoneum usuallylead tosevere atelec-tasis, increased level of PaCO2 and acidosis.2---4 However
intermittentrecruitmentmaneuvershouldbemadeto pre-vent and improve atelectasis due to pneumo-peritoneum and trendelenburg. Recruitment maneuver especially before extubation may improve postoperative lung functions.5
Consequently, effects due to excessive trendelenburg position in addition to classical complications of laparo-scopicprocedure at robotic-assistedlaparoscopic prostate surgery should be considered. Increasing airway pressure
is inescapable. Increasing minute ventilation may not be enough to be maintained in the PaCO2’s normal
range.Pressure-controlmodeforminglowerpeakpressure shouldbepreferredandappropriatePEEPsould besetted to prevent atelectasis.5,6 Also intermittant recruitment
maneuvershouldbemadeasneeded.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.OksarM,AkbulutZ,OcalH,etal.Roboticprostatectomy:the anesthetist’sviewforroboticurologicalsurgeries,aprospective study.BrazJAnesthesiol.2014;64(5):307---13.
2.Oksar M,Akbulut Z, Ocal H, et al. Anesthetic considerations forroboticcystectomy:aprospectivestudy.BrazJAnesthesiol. 2014;64(2):109---15.
3.Hypolito O, Azevedo JL, Gama F, et al. Effects of elevated artificial pneumoperitoneum pressure on invasive blood pres-sureandlevelsofbloodgases.BrazJAnesthesiol.2014;64(2): 98---104.
4.Ozdemır M, Bakan N, Sahın OT, et al. The comparison of sevoflurane-remifentanyland propofol-remifentanyl in robotic prostatectomies.JClinAnalMed.2013;4(4):313---7.
5.TalabHF,ZabaniIA,AbdelrahmanHS,etal.Intraoperative venti-latorystrategiesforpreventionofpulmonaryatelectasisinobese patientsundergoinglaparoscopicbariatricsurgery.AnesthAnalg. 2009;109(5):1511---6.