w w w . r b o . o r g . b r
Original
Article
Diagnosis
of
knee
injuries:
comparison
of
the
physical
examination
and
magnetic
resonance
imaging
with
the
findings
from
arthroscopy
夽
Nilton
Orlando
Júnior,
Marcos
George
de
Souza
Leão
∗,
Nelson
Henrique
Carvalho
de
Oliveira
Fundac¸ãoHospitalAdrianoJorge,Manaus,AM,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received23September2014 Accepted5November2014 Availableonline19October2015
Keywords:
Kneetrauma/diagnosis Kneetrauma/therapy Tibialmenisci
a
b
s
t
r
a
c
t
Objectives:Toascertainthesensitivity,specificity,accuracyandconcordanceofthephysical examination(PE)andmagneticresonanceimaging(MRI)incomparisonwitharthroscopy, indiagnosingkneeinjuries.
Methods:Prospectivestudyon72patients,withevaluationandcomparisonofPE,MRIand arthroscopicfindings,todeterminetheconcordance,accuracy,sensitivityandspecificity. Results:PEshowedsensitivityof75.00%,specificityof62.50%andaccuracyof69.44%for medialmeniscal(MM)lesions,whileitshowedsensitivityof47.82%,specificityof93.87% andaccuracyof79.16%forlateralmeniscal(LM)lesions.Foranteriorcruciateligament(ACL) injuries,PEshowedsensitivityof88.67%,specificityof94.73%andaccuracyof90.27%.For MMlesions,MRIshowedsensitivityof92.50%,specificityof62.50%andaccuracyof69.44%, whileforLMinjuries,itshowedsensitivityof65.00%,specificityof88.46%andaccuracyof 81.94%.ForACLinjuries,MRIshowedsensitivityof86.79%,specificityof73.68%andaccuracy of83.33%.ForACLinjuries,thebestconcordancewaswithPE,whileforMMandLMlesions, itwaswithMRI(p<0.001).
Conclusions:Meniscal and ligamentinjuries can be diagnosed through carefulphysical examination,whilerequestsforMRIarereservedforcomplexordoubtfulcases.PEand MRIusedtogetherhavehighsensitivityforACLandMMlesions,whileforLMlesionsthe specificityishigher.
LevelofevidenceII–Developmentofdiagnosticcriteriaonconsecutivepatients(with universallyappliedreference“gold”standard).
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkperformedattheOrthopedicsandTraumatologyService,Fundac¸ãoHospitalAdrianoJorge,Manaus,AM,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](M.G.deSouzaLeão). http://dx.doi.org/10.1016/j.rboe.2015.10.007
Diagnóstico
das
lesões
do
joelho:
comparac¸ão
entre
o
exame
físico
e
a
ressonância
magnética
com
os
achados
da
artroscopia
Palavras-chave: Traumatismosdo joelho/diagnóstico
Traumatismosdojoelho/terapia Meniscostibiais
r
e
s
u
m
o
Objetivos: Verificarasensibilidade,especificidade,acuráciaeconcordânciaentreoexame físico(EF)earessonânciamagnética(RM)emcomparac¸ãocomaartroscopia,nodiagnóstico daslesõesdojoelho.
Métodos: Estudoprospectivocom72pacientesavaliadosquantoaoEF,àRMeaos acha-dosartroscópicos.Foramcomparadososachadosentresieobservaram-seaconcordância, acurácia,sensibilidadeeespecificidade.
Resultados: OEFdemonstrousensibilidadede75%,especificidadede62,50%eacuráciade 69,44%paraaslesõesmeniscaismediais(MM).Paraomeniscolateral(ML)encontraram-se sensibilidadede47,82%,especificidadede93,87%eacuráciade79,16%.OEFdemonstrou, paralesõesdoligamentocruzadoanterior(LCA),sensibilidadede88,67%,especificidadede 94,73%eacuráciade90,27%.AslesõesdoMM,àsimagensdeRM,apresentaram sensibili-dadede92,50%,especificidadede62,50%eacuráciade69,44%.AslesõesdoMLapresentaram sensibilidadede65%,especificidadede88,46%eacuráciade81,94%.ARMevidencioupara asrupturasdoLCAsensibilidadede86,79%,especificidadede73,68%eacuráciade83,33%. ParaoLCA,amelhorconcordânciafoicomoEF;eparaMMeML,comaRM(p<0,001). Conclusões:Oexamefísicocuidadosodiagnosticaaslesõesmeniscaiseligamentares.ARMé reservadaparacasoscomplexosouduvidosos.Associados,EFeaRMtêmaltasensibilidade paraaslesõesdoLCAedoMM,porémparaoMLéaespecificidadequeémaior.
NíveldeEvidênciaII–Desenvolvimentodecritériosdiagnósticosempacientesconsecutivos (compadrãodereferencia“ouro”aplicado).
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Accuratediagnosingofkneeinjuriesisdirectlylinkedtotaking the clinical history and making a careful physical exami-nation.Meniscal andligament injuriesof thisjoint can be evaluated by means of magneticresonance imaging (MRI) examinations,whichprovideimagesshowingabnormalities ofthemorphologythatarecharacterized.Thesensitivityof thisexaminationcanberaisedaccordingtothemethodsused byradiologists.1 MRIisusuallyanaccuratetypeof
comple-mentaryexaminationforkneeassessment,but it hashigh cost.2
MRI hashigh applicability to the knees, in comparison withotherjoints,anditprovidesexcellentdiagnostic capac-ityforevaluatinglesionsofdifferenttypes,suchasligament, meniscal,tendon,boneandchondralinjuries.3However,no
evidenceto suggest that MRI mightreduce the number of negativearthroscopic procedures has been demonstrated.4
It has been shown that lesion of the anterior meniscal cornu seen on MRI may not any significant clinical pre-sentation,andcorrelationwiththephysicalexaminationis recommended.5Heterogenousresultsregardingtheaccuracy
of physical examinations on meniscal injuries have been observedbecauseofdeficienciesofclinicalpractice.6
Qualifiedorthopedicsurgeonscan safely diagnose ante-riorcruciateligamentandmeniscalinjuriesthroughphysical examination,whilereservingMRIforcomplicatedand con-fusingcases.Thispracticeisnotrecommendedinitially,and itimpairsthesurgeon’straining.7
Theprogressofarthroscopicsurgeryoverrecentdecades, together with clinical and complementary examinations, in association with the low morbidity ofthe surgical pro-cedure, has encouraged its use for diagnosing, treating and making prognoses in relation to intra-articular knee injuries.8
Theobjectiveofthepresentstudy wastodeterminethe accuracy,sensitivity,specificityandconcordanceofthe find-ingsfromphysicalexaminationsandMRIontheknee,taking arthroscopyonthisjointtobethegoldstandard.
Materials
and
methods
BetweenJune2012andDecember2013,aprospectivecohort studywasconductedon72patients(72knees:44rightknees and28leftknees)ofmeanage33.54years,rangingfrom17 to59years(SD34±9),anddistributedaccordingtosexas61 males(84.72%)and11females(15.28%).Thesepatients pre-sentedmeniscalandligamentinjuriesofthekneeandwere evaluatedasoutpatientsandthroughintraoperative arthro-scopicfindings.
acute injuries (less than four weeks since the injury); chondral injuries; femoropatellar pathological conditions; and refusal to sign the free and informed consent state-ment.
Eachpatient’sprevioushistoryofpathologicalconditions wastaken.Emphasis wasgiven tothe causeofthe injury. Thedifferentetiologiesoftheinjurieswere groupedas fol-lows: 58 related to sports (79.2%), 12 were due to trauma unrelated to sports (16.7%) and two were idiopathic (the patient could establish a causal link withthe injury). The patients were asked about their symptoms, such as pain, joint effusion, episodes ofinstability and episodes ofjoint locking. A detailed physical examination was undertaken by a surgeon with more than five years of experience of treating pathological conditions of the knee. In order to evaluate meniscal injuries, the McMurray test was used. For anterior cruciate ligament (ACL) injuries, the Lachman tests were used. Varus and valgus stress tests and poste-rior drawer tests were also performed. The patients’ MRI examinationswere then evaluated, always afterthe phys-ical examination. For the purposesof this study,only the report of the examinations and not the interpretations of the images was taken into consideration. The MRIs were produced infour different imagingcenters and the radiol-ogists didnot haveany contactwith the patientsand did not know about the present study. The MRI reports and physicalexaminationfindingswere noted accordingtothe anatomicalstructureinvolved,suchascruciateligamentsand menisci.
Thesurgery was performedby oneof the authors who had not participated in the initial attendance ofthe case. Theligament stability was again tested, under anesthesia. Arthroscopy was performed through the anterolateral and anteromedialportals.Duringtheoperation,theintra-articular injuriesofthekneefoundthrougharthroscopywerenoted. Anytypeofmeniscallesionencounteredduringthesurgery wasconsideredtobeapositivefinding,independentofthe type(radialorlongitudinal,simpleorcomplex,or degenera-tive)andthesidewasnoted(medialorlateral).Arthroscopy wasconsideredtobethegoldstandardinmakingthe diag-nosis of knee joint injuries. This study did not take into consideration the type of treatment for the joint injuries (meniscalandACL).
Theresultsfromcomparingthefindingsfromthe physi-calexamination,MRIandarthroscopywereobtainedthrough thisdatabase,andthesensitivity,specificity,accuracy,positive predictivevalue,negativepredictivevalueandconcordance wereevaluated.
Someoftheconceptsusedinthisstudyaredefinedbelow:
(1) Sensitivity–thisdemonstratedtheefficiencyofMRIand thephysicalexaminationfordiagnosinglesionsthrough arthroscopy.
TP/TP+TN
(2) Specificity – this demonstrated the efficiency of the parametersfordiagnosingtheabsenceoflesionsthrough arthroscopy.
TN/TN+FP
(3) Accuracy–thisdemonstratedthecapacityofthe physi-calexaminationorMRItocorrectlydefinethepresenceor absenceoflesionsthrougharthroscopy.
TP+TN/No.ofexaminations
(4) Positivepredictivevalue(PPV)–thiswasthelikelihoodthat thelesiondiagnosedonMRIorinthephysicalexamination wouldbepresentthrougharthroscopy.
TP/TP+FP
(5) Negativepredictivevalue(NPV)–thiswasthelikelihood that there would not beany lesion when the physical examinationorMRIwasnormal.
TN/TN+FN
(6) Truepositive(TP):physicalexaminationorMRIshowing lesion,andarthroscopyshowinglesion.
(7) Truenegative(TN):physicalexaminationorMRInormal, witharthroscopynormal.
(8) Falsepositive(FP):physicalexaminationorMRIshowing lesion,witharthroscopynormal.
(9) Falsenegative(FN):physicalexaminationorMRInegative, andarthroscopyshowinglesion.
Thedescriptiveanalysiswasperformedbymeansofthe Minitab statistical software, version 14.1. The kappa con-cordance analysis was performed through the website of the Epidemiology and StatisticsLaboratory (http://www.lee. dante.br/pesquisa/kappa/). Inthis analysis, thesignificance leveltakenfordecision-makingwas5%.
All the patients read and signedthe freeand informed consent statement and the study was submitted to and approved by the institution’s research ethics committee, under the ethics assessment certificate (CAAE) number 16051913.4.0000.0007.
Results
Throughthephysicalexamination,42kneeswerediagnosed with medialmeniscal injuries.From the arthroscopic find-ings,40 kneespresentedinjuries.Thus,thesensitivitywas 75%,specificity62.50%and accuracy69.44%. Forthe lateral meniscus,thetotalnumberofinjuriesencounteredwas14 and therewere positive arthroscopic findings in 23 knees, withsensitivityof47.82%,specificityof93.87%andaccuracyof 79.16%.
Anteriorcruciateligamentinjurieswerefoundin48knees from the clinical examinationand 53 through arthroscopy, withsensitivityof88.67%,specificityof94.73%andaccuracy of90.27%(Table1).
TheMRIshowedmedialmeniscalinjuriesin46kneesand arthroscopyshowedinjuriesin40menisci,thuspresenting sensitivity of92.50%, specificity of62.50% and accuracyof 69.44%.Forthelateralmeniscallesions,thefollowingresults werefound:19kneeswithinjuriesonMRIandpositive arthro-scopicfindingsin20knees,withsensitivityof65%,specificity of88.46%andaccuracyof81.94%.
Table1–Correlationofphysicalexaminationwitharthroscopy.
Resultsfromcorrelatingphysicalexaminationwitharthroscopyinthecasesof72knees
Sensitivity(%) Specificity(%) Accuracy(%)
Medialmeniscus 75.00 62.50 69.44
Lateralmeniscus 47.82 93.87 79.16
ACL 88.67 94.73 90.27
ACL,anteriorcruciateligament.
Table2–CorrelationofMRIwitharthroscopy.
ResultsfromcorrelatingMRIwitharthroscopyinthecasesof72knees
Sensitivity(%) Specificity(%) Accuracy(%)
Medialmeniscus 92.50 74.19 83.33
Lateralmeniscus 65.00 88.46 81.94
ACL 86.79 73.68 83.33
ACL,anteriorcruciateligament.
Table3–CorrelationofphysicalexaminationandMRIwitharthroscopy.
Resultsfromcorrelatingphysicalexamination/MRIwitharthroscopyinthecasesof72knees
Sensitivity Specificity Accuracy
Physical(%) MRI(%) Physical(%) MRI(%) Physical(%) MRI(%)
Medialmeniscus 75.00 92.50 62.50 74.19 69.44 83.33 Lateralmeniscus 47.82 65.00 93.87 88.46 79.16 81.94
ACL 88.67 77.35 94.73 73.68 90.27 76.38
MRI,magneticresonanceimaging;Physical,physicalexamination;ACL,anteriorcruciateligament.
Table4–Cross-correlationofphysicalexaminationandMRIwitharthroscopy.
Sensitivity(%) Specificity(%) Accuracy(%) PPV(%) NPV(%)
ACL 97.0 86.7 75.0 95.3 92.9
MM 96.2 76.5 52.8 86.2 92.8
LM 55.6 97.7 66.7 83.3 91.5
Physical,physicalexamination;MRI,magneticresonanceimaging;ACL,anteriorcruciateligament;MM,medialmeniscus;LM,lateralmeniscus; PPV,positivepredictivevalue;NPV,negativepredictivevalue.
Table5–Evaluationofconcordancebetweenthe
diagnosticmethodsforACLinjuriesbymeansof
arthroscopy,MRIandphysicalexamination.
Diagnosticexaminations Kappa Concordance p-Value
ArtversusMRIversusphysicala 0.55 Moderate <0.001 ArtversusMRIb 0.51 Moderate <0.001 Artversusphysicalc 0.66 Strong <0.001
ACL,anteriorcruciateligament;Art,arthroscopy;MRI,magnetic resonanceimaging;Physical,physicalexamination.
a Concordancewasfoundbetweenthethreemethods.
b ConcordancewasfoundbetweenarthroscopyandMRI.
c ConcordancewasfoundbetweenarthroscopyandMRI.
73.68% and accuracy of83.33% (Table 2). Table 3 shows a summaryofthedatapresentedabove.Table4showsthe phys-icalexaminationandMRIvaluescombined,witharthroscopy takentobethegoldstandardforthediagnosis.
Table6–Evaluationofconcordancebetweenthe
diagnosticmethodsformedialmeniscalinjuriesby
meansofarthroscopy,MRIandphysicalexamination.
Diagnosticexaminations Kappa Concordance p-Value
ArtversusMRIversusphysicala 0.367 Slight/fair <0.001 ArtversusMRIb 0.630 Strong <0.001 Artversusphysicalc 0.322 Slight/fair <0.001
MM,medialmeniscus;Art,arthroscopy;MRI,magneticresonance imaging;Physical,physicalexamination.
a Slight/fairconcordancewasfoundbetweenthethreemethods.
b StrongconcordancewasfoundbetweenarthroscopyandMRI.
c Slight/fairconcordancewasfoundbetweenarthroscopyandMRI.
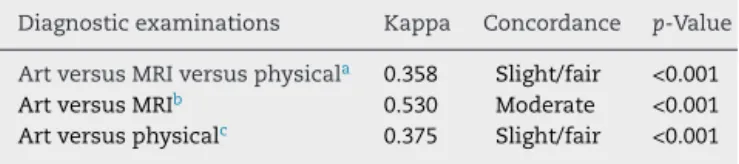
Table7–Evaluationofconcordancebetweenthe diagnosticmethodsforlateralmeniscalinjuriesby
meansofarthroscopy,MRIandphysicalexamination.
Diagnosticexaminations Kappa Concordance p-Value
ArtversusMRIversusphysicala 0.358 Slight/fair <0.001 ArtversusMRIb 0.530 Moderate <0.001 Artversusphysicalc 0.375 Slight/fair <0.001
MM,lateralmeniscus;Art,arthroscopy;MRI,magneticresonance imaging;Physical,physicalexamination.
a Slight/fairconcordancewasfoundbetweenthethreemethods.
b StrongconcordancewasfoundbetweenarthroscopyandMRI.
c Slight/fairconcordancewasfoundbetweenarthroscopyandMRI.
between arthroscopy and the physical examination, for which the kappa value was 0.665; this concordance was significant (p<0.001). For the medial meniscus, the best concordance observed was between arthroscopy and MRI (=0.630;p<0.001)andforthelateralmeniscus,thebest con-cordanceencounteredwasalsobetweenarthroscopyandMRI (=0.530;p<0.001)(Tables5–7).
Discussion
Ligament and meniscal injuries of the knee are generally diagnosedbyorthopedicsurgeonsbymeansofphysical exam-ination,withcomplementaryaidfromMRI.Inthisstudy,the concordancebetweenthesetwotypesofdiagnosticmethod wasinvestigatedincomparisonwiththearthroscopicfindings fromtheknee.
According to Magee et al.,1 comparison between
arthroscopy and MRI presented sensitivity for meniscal injuries of the knee of89% and demonstrated that signal abnormalitiesseenonMRIgaveinformationabout morpho-logicalalterationsofinjuries.Intheirstudy,thesensitivityand specificityvaluesforMRIandarthroscopywererespectively 70.4%and50%formeniscalinjuries.
Brooks et al.4 demonstrated that MRIdid not have the
capacitytodecreasethenumberofnegativearthroscopy pro-cedures,giventhatthephysicalexaminationhadconcordance of79%withthearthroscopicfindingsandMRIshowed con-cordanceof77%witharthroscopy.
StudiesconductedbyShepardetal.5havesuggestedthat
meniscal injuries of the anterior cornu, which are found throughanincreaseintheMRIsignal,commonlydonothave apparentclinicalsigns.Thissuggeststhatthereisa correla-tionofinterpretationsofMRIwiththephysicalexamination. Asdemonstrated byKocabey et al.7 in2004, therewas no
statistical significance(p>0.05) incomparing MRI withthe physicalexamination,indiagnosingmeniscalandligament injuriesofthekneeinrelationtothearthroscopicfindings. Thissuggeststhatwell-trainedorthopedicsurgeonscansafely diagnoseanteriorcruciateligamentinjuriesandthatthe rou-tineofindicatingMRIbeforethephysicalexaminationisnot recommended.
Analysesconducted byPolly et al.9 concluded that MRI
hasadjuvant value in relationto physicalexamination, in preoperativeplanning for knee operations,with sensitivity andspecificityof66.7%and95.1%respectivelyformeniscal
injuries,and100%and96.9%forACLinjuriesevaluatedusing MRI.
MRI should be used as an auxiliary tool in diagnosing meniscalandligamentinjuries,accordingtoChangetal.,10
whodemonstratedsensitivityof92%andspecificityof87%for MRIincomparisonwitharthroscopy,forkneeswithmeniscal injuries.
In acuteinjuriesinwhichphysicalexaminationmaybe inconclusive,MRIhelpsinthediagnosisinthispopulationand mayguidethesurgicalindication,accordingtoMunshietal.11
However,itscorrelationwitharthroscopyinthispopulation hasnotyetbeendocumented.
Combinedmethodsfordiagnosingkneeinjuriesconsisting ofphysicalexaminationandMRIwerefoundtobecapableof diminishingthenumberofnegativearthroscopyprocedures by5%,asdemonstratedbyMunketal.12 Thissuggeststhat
MRIhasdiagnosticvalueandhelpsinrelationtothetypeof anesthesiaandtreatment,andthatitmaysignificantlyreduce theneedforasecondarthroscopicintervention.
Inadouble-blindstudy,Rappeportetal.13commentedthat
knee arthroscopy was performed without priorknowledge oftheMRIdata. TheaccuracyoftheMRIwasgreater than arthroscopyasthegoldstandardfordiagnosis,andwhenMRI wasusedasthestandard,theaccuracyofthearthroscopywas lower,giventhatinacertainsmallnumberofpatients,some injuriesfoundonMRIwerenotshownduringarthroscopy.It wassuggestedthatMRIshouldbeusedinitiallyfor diagnos-ingkneeinjuries,whichwouldalsodiminishthenumberof negativearthroscopyprocedures.
Gelbetal.14demonstratedthatMRIhasbeenused
exces-sivelyincasesofkneedisordersanddoesnothaveafavorable cost–benefitrelationshipinrelationtophysicalexamination, in comparisons with arthroscopy. For physical examina-tion,theseauthorsfoundsensitivityandspecificityof100%, whereasincomparingMRIwitharthroscopy,theyfound val-uesof95%and88%.
In a Brazilian study, Schneider et al.15 found that MRI
wasareliableexaminationfordiagnosingkneeinjuries,with sensitivityof53%andspecificityof95%forACLinjuries,in comparisonwitharthroscopy.
Inthepresentstudy,thesensitivityandspecificityvalues forMRIcomparedwitharthroscopywere86.79%and73.68% respectively,forACLinjuries.
Severinoet al.16 suggestedthatMRIwasanappropriate
methodforcomplementingthephysicalexaminationincases ofligament andmeniscal injuriesofthe kneeand demon-stratedsensitivityandspecificityvaluesforMRIforinjuriesof theACL,medialmeniscusandlateralmeniscusofrespectively 82%and96%,96%and66%,and87%and88%,incomparison witharthroscopy.
IntheanalysesofYousefetal.17onthecorrelationbetween
Inthepresentstudy,physicalexaminationandMRIwere evaluatedand comparedwitharthroscopy.Thiswas differ-entfromthestudiescitedabove,inwhichotherparameters wereevaluated.Theaccuracyofthephysicalexaminationfor medialmeniscalinjurieswasfoundtobe69.44%andthe accu-racyofMRIwas83.33%.Forthelateralmeniscus,thevalues were79.16%forthephysicalexaminationand81.94%forMRI. ForACLinjuries,theaccuracyofthephysicalexaminationwas foundtobe90.27%andtheaccuracyofMRIwas83.33%.
TheaccuracyofMRIfordetectingkneeinjurieswasmore than 90%when it wasevaluated byspecialists, as demon-stratedbyBen-Galinetal.,18 buttheyfoundafalse-positive
rateof47%forACLinjuries,incomparisonwiththe intraoper-ativefindings.Theaccuracyratewas80%forligamentinjuries. Thus,37%ofthesurgicalproceduresindicatedbecauseof sig-nificantalterationsseenonMRIwereperformedunjustifiably. AccordingtoVinckenetal.,19patientswhorequire
arthro-scopictreatmentcanbeappropriatelyidentifiedbymeansof MRIexamination,because ofthesensitivityand specificity ratesof87%and 88%.Theirdatawere similartowhatwas foundinthepresentstudy.
Gobbo et al.20 concluded that the set ofmaneuvers for
meniscal injurieshad good accuracyand significant value, compared with MRI, especially for ruling out other joint injuries.
In2013,Navaliet al.21 stated thatphysicalexamination
andMRIhadacceptablediagnosticpowerinrelationtoknee injuries,althoughphysicalexaminationwasslightlysuperior. Thus,becauseofthecost,MRIshouldbereservedforcasesin whichthereweredoubts,orforcomplexinjuries.
Differingfromtheabovecitations,Yanetal.22statedthat
MRIhadgreateraccuracy,sensitivityandnegativepredictive valuethanclinicalmaneuversincasesofmeniscalinjuries. TheyrecommendedthatMRIshouldberoutinelyrequested fordetectingthistypeofinjury.Thesefindingswere corrobo-ratedinthe presentstudy,withsimilarresults,comprising accuracy,sensitivity and negativepredictive values greater than those from physicalexamination, respectively as fol-lows:medialmeniscus,83.33%versus6944%,92.50%versus 75%and88.46%versus66.66%;andlateralmeniscus,81.94% versus79.16%,65%versus47.82%and86.79%versus79.31% (MRIversusphysicalexamination).
TheefficacyofMRIinrelationtoacutekneetraumahasnot beenstudiedappropriately.Inadoubleblindstudy, Muham-mad etal.23 evaluatedthe clinical efficacy ofMRIin cases
ofacuteknee trauma withinconclusivephysical examina-tions,andusedarthroscopyasthediagnosticgoldstandard. The sensitivity and specificity of MRI were 90% and 67%, respectively,fordetectinganyACLinjuries,50%and86%for medialmeniscal injuries and 88% and 73% forthe lateral meniscus.They thereforesuggestedthat evaluationsusing MRI should be used to guide the need for surgery when theclinicalexaminationwasinconclusive,asinacuteknee injuries.23
Theobjectiveofevaluatingtheaccuracyofphysical exami-nationincomparisonwitharthroscopyandMRIwasthetopic ofastudybyVenuetal.24Theystatedthatphysical
examina-tionalonewasunsatisfactoryfordiagnosingkneeinjuriesand reportedthatMRIandarthroscopywereconcordantin94%of thepatientsevaluated.
In our evaluation, the physical examination presented greateraccuracyinrelationtoarthroscopythandidMRIfor lig-amentinjuries.However,formeniscalinjuries,MRIpresented greateraccuracyinrelationtoarthroscopy.
Evaluationsofkneeinjuriesweremadebymeansof phys-ical examination in this study. However, Solomon et al.25
concluded from analyzing the accuracyofphysical exami-nationformeniscalandligamentinjuriesthatthismightbe betterusedfordiagnosiswhenassociatedwiththepatient’s history and use of a set ofmaneuvers, instead ofspecific maneuversformeniscalandligament injuriesapplied sep-arately.
In2009,Ryanetal.26alsocametotheconclusionthat
phys-icalexaminationperformedcarefullycouldprovidethesame orevenabetterdiagnosisofmeniscalandligamentinjuries, incomparisonwithMRI.
In2012,Ercinetal.27reportedthatphysicalexaminations
thatwereperformedwell,byexperiencedsurgeonsusing mul-tiplemaneuvers,weresufficientformakingthediagnosisof meniscalinjuries.Theirfindingswere similartotheresults fromthepresentstudy.
Thestudy byValles-Figueroaetal.28wasmoreemphatic
incontraindicatingroutinerequestsforMRIexaminationsfor evaluatingkneeinjuries.Theseauthorsstatedthatphysical examinationwassufficientfordiagnosingmeniscaland liga-mentinjuriesofthisjoint.
For medialmeniscal injuries, physicalexamination has greatersensitivitythanMRI,althoughitsaccuracyand speci-ficityarelow,accordingtoSharmaet al.29Theirdatadiffer
somewhatfromours,inwhichMRIwasmoresensitivethan physicalexamination,althoughtheaccuracyandspecificity ofphysicalexaminationwerelowinourstudytoo,inrelation toMRI.
Accordingtotheliterature,30withregardtoarthroscopy,
thereisariskofapproximately8%inrelationtothesurgical procedure.Forthisreason,thepresentauthorsdonotuseit onlyasadiagnosticmethod,butalsoasatherapeuticmethod. Inaddition,arthroscopyusedonlyfordiagnosisisaninvasive tool,anditisslowerandmoreexpensivethanMRI.
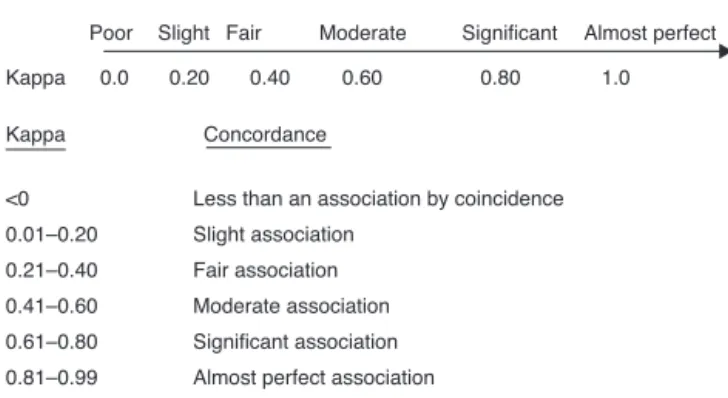
Inordertoevaluatetheconcordanceamongthe parame-tersanalyzed,weusedthekappacoefficient(),asdescribed byVieiraandGarret,31withconcordancevaluesasexpressed
in Fig. 1. Through this, the best concordance was found to be between the physical examination and ACL injuries (=0.665),whichwassignificantconcordance(p<0.001).For medialmeniscalinjuries,thebestconcordancewasobserved betweenarthroscopyandMRI(=0.630;p<0.001);andfor lat-eralmeniscalinjuries,thebestconcordancewasalsofoundto bebetweenarthroscopyandMRI(=0.530;p<0.001).Wedid notfindanysimilarvaluesinthecurrentliterature.
Poor Slight Fair Moderate Significant Almost perfect
Kappa 0.0 0.20 0.40 0.60 0.80 1.0
Concordance Kappa
Less than an association by coincidence <0
Slight association 0.01–0.20
Fair association 0.21–0.40
Moderate association 0.41–0.60
Significant association 0.61–0.80
Almost perfect association 0.81–0.99
Interpretation of kappa
Fig.1–Interpretationofthekappacoefficient;Vieiraand Garret,312005.
instability,onlythe Lachmanmaneuverswereapplied.The method appliedfor treating these injuries, along with the long-term follow-up of these patients, was outside of the scopeofthepresentstudy.
Conclusions
AlthoughMRIandarthroscopyareexcellentcomplementary methodsfordiagnosingintra-articularkneeinjuries,physical examinationcanstillprovideaprecisediagnosiswhendone carefullybyanexperiencedsurgeon,especiallyincasesofACL injury. Thisis evencapableofpromoting lower healthcare costs.MRIshouldonlybeusedtocomplementthefindings indoubtfulcasesorincomplexinjuriesinwhichthe clini-calexaminationisinconclusive,and arthroscopyshouldbe usedfortreatingthese injuries.MRIshould beanoptional examination,ratherthanaroutineexamination.When phys-icalexaminationandMRIwereusedtogether,theirsensitivity forACLandmedialmeniscalinjurieswashighandthe speci-ficityforthelateral meniscuswashigher.For ACLinjuries, therewasconcordancebetweentheexaminations.However, thebestconcordancewasbetweenarthroscopyandphysical examination.Forthemedialmeniscus,thebestconcordance wasobservedbetweenarthroscopyandMRIandforthelateral meniscusitwasalsobetweenarthroscopyandMRI.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. MageeT,ShapiroM,WilliamsD.MRaccuracyand arthroscopicincidenceofmeniscalradialtears.Skeletal Radiol.2002;31(12):686–9.
2. FelerJA,WebsterKE.Clinicalvalueofmagneticresonance imagingoftheknee.ANZSurg.2001;71(9):534–7.
3. SandersTG,MillerMD.Asystematicapproachtomagnetic resonanceimaginginterpretationofsportsmedicineinjuries oftheknee.AmJSportsMed.2005;33(1):131–48.
4.BrooksS,MorganM.Accuracyofclinicaldiagnosisinthe kneearthroscopy.AnnRCollSurgEngl.2002;84(4):265–8. 5.ShepardMF,HunterDM,DaviesMR,ShapiroMS,SeegerLL.
Theclinicalsignificanceofanteriorhornmeniscaltears diagnosedonmagneticresonanceimages.AmJSportsMed. 2002;30(2):189–92.
6.ScholtenRJ,DevilleWL,OpsteltenW,BijlD,vanderPlassCG, BouterLM.Theaccuracyofphysicaldiagnostictestsfor assessingmeniscallesionsoftheknee:ameta-analysis.J FamPract.2001;50(11):938–44.
7.KocabeyY,TetikO,IsbellWM,AtayOA,JohnsonDL.Thevalue ofclinicalexaminationversusmagneticresonanceimaging inthediagnosisofmeniscaltearsandanteriorcruciate ligamentrupture.Arthroscopy.2004;20(7):696–700. 8.BarryBP.Generalprinciplesofarthroscopy.In:TerrySC,
editor.Campbell’soperativeorthopaedics,vol.2,9thed. Philadelphia:MosbyInc.;1999.p.364–73.
9.PollyDW,CallaghanJJ,SikesRA,McCabeJM,McMahonK, SavoryCG.Theaccuracyofselectivemagneticresonance imagingcomparedwiththefindingsofarthroscopyofthe knee.JBoneJointSurgAm.1988;70(2):192–8.
10.ChangCY,WuHT,HuangTF,MaHL,HungSC.Imaging evaluationofmeniscalinjuryofthekneejoint:acomparative MRimagingandarthroscopicstudy.ClinImaging.
2004;28(5):372–6.
11.MunshiM,DavidsonM,MacDonaldPB,FroeseW,Sutherland K.Theefficacyofmagneticresonanceimaginginacuteknee injuries.ClinJSportMed.2000;10(1):34–9.
12.MunkB,MadsenF,LundorfE,StaunstruspH,SchmidtSA, BolvigL,etal.Clinicalmagneticresonanceimagingand arthroscopicfindingsinknees:acomparativeprospective studyofmeniscusanteriorcruciateligamentandcartilage lesions.Arthroscopy.1988;14(2):171–5.
13.RappeportED,WieslanderSB,StephensenS,LaustenGS, ThomsenHS.MRIpreferabletodiagnosticarthroscopyin kneeinjuries.Adouble-blindcomparisonof47patients.Acta OrthopScand.1997;68(3):277–81.
14.GelbHJ,GlasgowSG,SapegaAA,TorgJS.Magneticresonance imagingofkneedisorders.Clinicalvalueand
cost-effectivenessinasportsmedicinepractice.AmJSports Med.1996;24(1):99–103.
15.SchneiderI,SchuedaMA,DemoreAB.Análisecomparativada ressonâncianuclearmagnéticacomaartroscopiano diagnósticodaslesõesintra-articularesdojoelho.RevBras Ortop.1996;31(5):373–6.
16.SeverinoNR,CamargoOPA,AiharaT,CuryRPL,OliveiraVM, VazCES,etal.Comparac¸ãoentrearessonânciamagnéticaea artroscopianodiagnósticodelesõesdojoelho.RevBras Ortop.1997;32(4):275–8.
17.YousefWJ,ThieleES,ScuisatoDL.Correlac¸ãodiagnósticada ressonânciamagnéticacomartroscopianaslesões
intra-articularesdojoelho.RevBrasOrtop.1999;34(6):375–80. 18.Ben-GalinP,SteinbergEL,HagaiA,NachmanA,ShumuelD,
RonA.Accuracyofmagneticresonanceimagingofthekee andunjustifiedsurgery.ClinOrthopRelatRes.2006;447:100–4. 19.VinckenPWJ,terBraakBPM,vanErkelAR,CoerkampEG,de
RooyTPW,MallensWMC,etal.Magneticresonanceimaging oftheknee:areview.ImagingDecisions.2006;10(1):24–30. 20.GobboRR,RangelVO,KaramFC,PiresLAS.Oexamefísicono
diagnósticodaslesõesmeniscais:umacorrelac¸ãoocmos achadoscirúrgicos.RevBrasOrtop.2011;46(6):726–9. 21.NavaliAM,BazavarM,MohseniMA,SafariB,TabriziA.
Arthroscopicevaluationoftheaccuracyofclinical examinationversusMRIindiagnosingmeniscustearsand cruciateligamentruptures.ArchIranMed.2013;16(4):229–32. 22.YanR,WangH,YangZ,JiZH,GuoYM.Predictedprobabilityof
23.MuhammadM,MichaelD,PeterMB,WarrenF,KellyS.The efficacyofmagneticresonanceimaginesinacuteknee injuries.JSportsMed.2000;10(1):34–9.
24.VenuKM,BonniciAV,MarchbankNDP,ChipperfieldA, StenningM,HowlettDC,etal.Clinicalexamination,MRIor arthroscopy:whichisthegoldstandardinthediagnosisof significantinternalderangementintheknee?JBoneJoint SurgBr.2003;85Suppl.2:167.
25.SolomonDH,SimelDL,BatesDW,KatzJN,SchafferJL.Does thispatienthaveatornmeniscusorligamentoftheknee? Valueofthephysicalexamination.JAMA.
2001;286(13):1610–20.
26.RayanF,BhonsleS,ShuklaDD.Clinical,MRIandarthroscopic correlationinmeniscalandanteriorcruciateligament injuries.IntOrthop.2009;33(1):129–32.
27.ErcinE,KayaI,SungurI,DemirbasE,UgrasAA,CetinusEM. History,clinicalfindings,magneticresonanceimaging,and
arthroscopiccorrelationinmeniscallesions.KneeSurg SportsTraumatolArthrosc.2012;20(5):851–6.
28.Valles-FigueroaJF,Malacara-BecerraM,Villegas-ParedesP, Caleti-DelMazoE.ComparisonofMRIandarthroscopic imagesforthediagnosisofkneedisorders.ActaOrtopMex. 2010;24(1):8–13.
29.SharmaUK,ShresthaBK,RijalS,BijukachheB,BarakotiR, BanskotaB,etal.Clinical,MRIandarthroscopiccorrelationin internalderangementofknee.KathmanduUnivMedJ (KUMJ).2011;9(35):174–8.
30.RoseNE,GoldSM.Acomparisonofaccuracybetweenclinical examinationandmagneticresonanceimaginginthe diagnosisofmeniscalandanteriorcruciateligamenttears. Arthroscopy.1996;12(4):398–405.