SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Effect
of
muscle
contractions
on
cartilage:
morphological
and
functional
magnetic
resonance
imaging
evaluation
of
the
knee
after
spinal
cord
injury
夽
Marco
Kawamura
Demange,
Camilo
Partezani
Helito
∗,
Paulo
Victor
Partezani
Helito,
Felipe
Ferreira
de
Souza,
Riccardo
Gomes
Gobbi,
Alexandre
Fogac¸a
Cristante
UniversidadedeSãoPaulo,FaculdadedeMedicina,DepartamentodeOrtopediaeTraumatologia,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received16September2015 Accepted22January2016 Availableonline2February2016
Keywords:
Spinalcordinjuries Knee
Cartilage,articulation Magneticresonanceimaging Musclecontraction
a
b
s
t
r
a
c
t
Objective:Toevaluate theeffectofcompleteabsenceofmusclecontractionsonnormal humancartilageinthepresenceofjointmotion.
Methods:Patientswithcompleteacutespinalcordinjurieswereenrolled.Allpatients under-wentmagneticresonanceimaging(MRI)onbothkneesassoonastheirmedicalcondition wasstableandatsixmonthsaftertheprimarylesion.Allpatientsreceivedrehabilitation treatmentthatincludedlower-limbpassivemotionexercisestwiceaday.TheMRIswere analyzedbytworadiologistswithexpertiseinmusculoskeletaldisorders.Aregionofinterest wasestablishedatthepatellarfacetsandtrochlea,andT2relaxationtimeswerecalculated. TheareaunderthecartilageT2relaxationtimecurvewascalculatedandstandardized. Results:Fourteenpatientswithcompletespinalcordinjurieswereenrolled,butonlyeight patientsagreedtoparticipateinthestudyandsignedtheinformedconsentstatement.Two patientscouldnotundergokneeMRIduetotheirclinicalconditions.InitialkneeMRIswere performedonsixpatients.Aftersixmonths,onlytwopatientsunderwentthesecond bilat-eralkneeMRI.BothpatientswereneurologicallyclassifiedasFrankelA.AnincreaseinT2 valuesonthesix-monthMRIwasobservedforbothknees,especiallyinthepatellofemoral joint.
Conclusion: Theabsenceofmusclecontractionsseemstobedeleterioustonormalhuman kneecartilageeveninthepresenceofanormalrangeofmotion.Furtherstudieswitha largernumberofpatients,despitetheirhighlogisticalcomplexity,mustbeperformedto confirmthishypothesis.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheDepartmentofOrthopedicsandTraumatology,HospitaldasClinicas,FacultyofMedicine,UniversidadedeSão Paulo,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:Camilohelito@yahoo.com.br(C.P.Helito). http://dx.doi.org/10.1016/j.rboe.2016.01.009
Palavraschave: Traumamedular Joelho
Cartilagem,articulac¸ão Imagemderessonância magnética
Contrac¸ãomuscular
Objetivo: Avaliaro efeito da completa ausência de contrac¸ão muscular nacartilagem humananormalnapresenc¸ademovimentoarticular.
Métodos: Pacientes comlesão completa da medula espinalforam incluídos. Todos os pacientesforamsubmetidosàressonânciamagnética(RM)emambososjoelhosassim queascondic¸õesclínicasforamestabilizadasedepoisdeseismesesdalesãoinicial.Todos ospacientesreceberamtratamentodereabilitac¸ãoqueincluíamovimentospassivospara exercitarosmembrosinferioresduasvezespordia.RMforamanalisadaspordois radiologis-tascomexperiênciaemdoenc¸asmusculoesqueléticas.Asregiõesdeinteresseconsideradas foramasdapatelaenatróclea,eostemposderelaxamentoT2foramcalculados.Aáreada cartilagemabaixodosvaloresderelaxamentoemT2foicalculadaepadronizada. Resultados: Catorzepacientescomlesãomedularcompletaforamincluídos,porémapenas oitopacientesconcordaramemparticipardoestudoeassinaramotermodeconsentimento informado.DoispacientesnãopuderamfazerRMdosjoelhosdevidoàscondic¸õesclínicas. RMinicialfoifeitaemseispacientes.Apósseismeses,apenasdoispacientesfizerama segundaRMdeambososjoelhos.Ambosestavamemcondic¸ãoneurológicaclassificada comoFrankelA.UmaumentodosvaloresemT2nosextomêsfoiobservadoemambosos joelhos,especialmentenaarticulac¸ãopatelofemoral.
Conclusão: Aausênciadecontrac¸ãomuscularpareceserdeletériaàcartilagemdojoelho humanonormal,mesmonapresenc¸ademovimentosarticularesnormais.Maisestudos comumnúmeromaiordepacientesdevemserfeitosparaconfirmarestahipótese.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Severalinvitroandanimalstudieshaveshownthatacertain amountofmechanicalloadingandjointmovementisrequired tomaintainnormalcartilagemorphology,biochemical com-position,andbiomechanicalproperties.1,2
Spinal cord injury (SCI) causes decreases in muscle mass, cardiovascular fitness, bone density, and unload-ing due tothe absence ofmuscle contractions.3,4 Previous studies have shown differences in patellar and tibial car-tilage thickness, mainly progressive thinning (atrophy), in SCI patients compared with age-matched healthy volun-teers due to the absence of normal joint loading and movement.5
These differences may be due to inadequate cartilage nutritionandtheabsenceofgoodeffectsofloadingand move-ment of the joint, which are of majorimportance for the maintenanceofthemorphologicalandfunctionalintegrityof articularcartilage.6,7
Oneimportantreasonforthiscartilagethinningis immo-bilization.Someauthorshaveconcludedthatexercisessuch as continuous passive motion can prevent this type of alteration.8However,webelievethatthepublishedevidence isinsufficienttoconcludethatthistypeofmovementinthe absenceofmusclecontractionscanpreventarticularcartilage damage.
Therefore,theobjectiveofthisstudywastoevaluatethe effectofthecompleteabsenceofmusclecontractionson nor-malhumancartilageinthepresenceofjointmotion.
Method
Thisstudyreceivedinstitutionalreviewboard(IRB)approval from ourinstitution. Weenrolledpatientswitha complete spinalcordlesionwithtetraplegiaorcompleteparaplegia.We didnotenrollpatientswithspinalcordlesionsatthe lum-barleveltoassurethecompleteabsenceoflowerlimbmuscle contractions.
Allpatientsunderwentkneemagneticresonanceimaging (MRI)afterthediagnosisoftheiracutelesionassoonastheir medicalconditionwasstabletoavoidharmduetothisexam. All MRI scans were performed with a1.5-T MR imager (SignaExciteHD;GEHealthcare,Waukesha,WI,USA)usinga dedicatedkneecoil(HDT/R8-channelHigh-ResolutionKnee Array).ThescanswereperformedusinganMRIknee imag-ingprotocolwithsagittalandcoronalT1-weightedsequences, aswellassagittal,coronal,andaxialT2-weightedsequences withfatsaturationfastspin-echosequences.
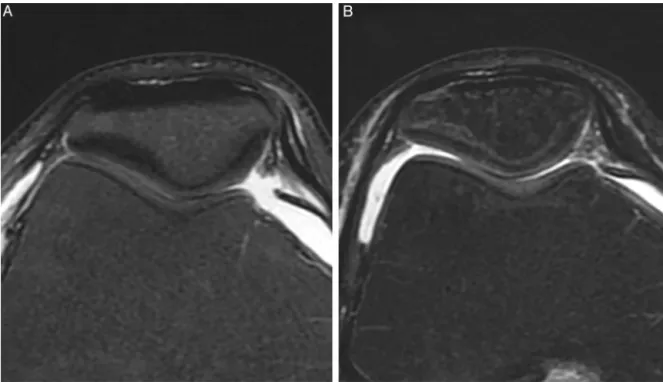
Fig.1–AxialT2WIatthepatellofemoraljoint.Initialimaging(A)andimagingattheone-yearfollow-up(B)demonstratinga similarcartilagesignals.
totalacquisitiontime,3min50s.Using asagittallocator, a singleaxialdatasetwasobtainedforthepatellofemoraljoint. AsecondMRIwasperformedsixmonthsafterthespinal cordinjury.None ofthepatientsexhibitedimprovementin theneurologicalconditionofthelowerlimbatthetimeofthe secondevaluation.
All patients received rehabilitation treatment, including lowerlimbpassivemotionexercisestwiceaday. The reha-bilitationteamincludedphysiotherapistsandaphysiatrist.
TheMRIswereanalyzedbytworadiologistswithexpertise inmusculoskeletaldisorders.
Aregionofinterest(ROI)wasplacedatthepatellarfacets andtrochlea,andtheT2relaxationtimewascalculated.The areaunderthecurveofthecartilageT2relaxationtimewas calculatedandstandardized
Results
Weenrolled14 patientswith completespinal cordinjuries whometourinclusioncriteria,butonlyeightpatientsagreed toparticipateinthestudyandsignedtheinformedconsent form.
TwopatientscouldnotundergokneeMRIduetoclinical conditions,andsixpatientsunderwenttheinitialkneeMRI.
Aftersixmonths, onlytwo patientshad undergone the secondbilateralkneeMRI.Bothpatientswereneurologically classifiedasFrankelA,definedasalackofmotoractivityor sensibilitybelowtheleveloftheinjury.
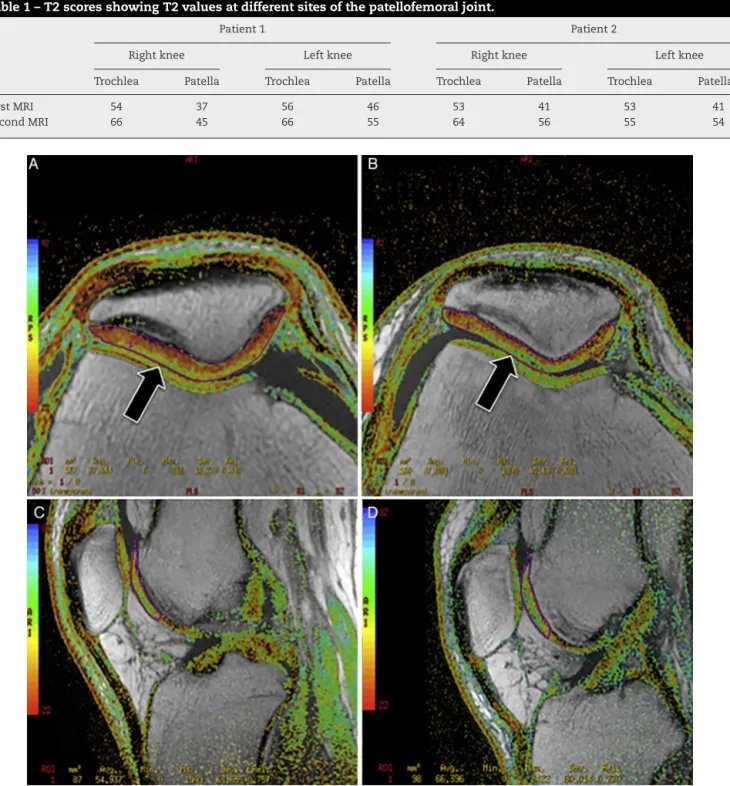
Table1presentstheT2mappingvaluesforthetwopatients in both knees. Note that there is an increase in the T2 valueatthesix-monthMRIforbothknees,especiallyinthe patellofemoraljoint(Figs.1and2).
Discussion
Toourknowledge,thisisthefirststudyprovidingevidence of early cartilage degradation by prospectively performing MRI with T2 mapping in non-ambulatory complete spinal cordinjurypatients.PreviousMRIstudieshadsuggestedthis hypothesis but could not prospectively perform serial MRI exams.5
The addition of a T2 mapping sequence to a rou-tine MRI protocol at 3.0T improved the sensitivity of the detection of cartilage lesions within the knee joint from 74.6% to 88.9%,with only a small reduction in specificity. The greatest improvement in sensitivity with the use of the T2 maps was in the identification of early cartilage degeneration.9
Trochlea Patella Trochlea Patella Trochlea Patella Trochlea Patella
FirstMRI 54 37 56 46 53 41 53 41
SecondMRI 66 45 66 55 64 56 55 54
Fig.2–Axial(AandB)andsagittal(CandD)T2mappingimagesatthepatellofemoraljoint.Initialimaging(AandC)and imagingattheone-yearfollow-up(BandD)demonstratingqualitativechangesandincreasedT2valuesatthesuperficial layerofthepatellarcartilage(blackarrows).Accordingtothescaleused,greenpointsrepresentworsecartilagequality.
Ruckstuhletal.12demonstratedtheeffectofincreasedor reducedloadingonshoulderarticularcartilage.Thefollowing threegroupswerecompared:individualswithparaplegiawith highshoulderdemand(n=11),individualswithquadriplegia withreducedloadingoftheshoulderjoint(n=8),andacontrol group(n=9).Therewasnodifferenceincartilagethickness or minimum joint space according to MRI with 3D recon-struction.Inananimalstudy,Moryamaetal.13observedthat thecartilagethicknessinspinalcord-injuredkneesdecreased
Vanwanseeleet al.5,14 performed a transversal study by analyzingkneecartilageinpatientswithcompletetraumatic spinalcordinjurieswithMRIat6(n=9),12 (n=11),and 24 months(n=6)aftertheinjury.Theresultswerecomparedwith thoseinyoung,healthyvolunteers(n=9).Theindividual dif-ference mapsof43% ofthepatients showedlocalareas of substantialthinning6and12monthsafterinjury.Thedata obtainedbyVanwanseeleetal.5,14corroborateourfindingsby showinganegativeeffectofspinalcordinjuryonknee artic-ularcartilage.Inourreport,weprospectivelycomparedeach individualafterasix-monthperiodbyperformingtwoserial MRIs.
To evaluate the effect of overloading of articular carti-lage,Muhlbaueretal.15comparedcartilagethicknessbetween ninetriathletesandninephysicallyinactivevolunteers.There wasahighinterindividualvariabilityofthemeanand max-imumcartilagethicknessvaluesforallsurfaces,bothinthe triathletesandintheinactivevolunteers.Inthepatella,the femoraltrochlea,andthelateralfemoralcondyle,themean andmaximumcartilagethicknessvalueswereslightlyhigher inthetriathletes,buttheyweresomewhatlowerinthemedial femoralcondyleandinthemedialandlateraltibialplateau. However,thedifferencesdidnotattainstatisticalsignificance. Torzilli et al.2 observed that mechanical loading of sufficientmagnitudecaninhibitECMdegradation by chon-drocyteswhenstimulatedbyinterleukin(IL)-1.Themolecular mechanismsinvolvedinthisprocessarenotclearbut prob-ably involve altered mechanochemical signal transduction betweentheECMandchondrocytes.
Continuouspassivemotioniscommonlyused postopera-tivelyfollowingcartilagesurgery.Unfortunately,theclinical evidence16–19tosupporttheuseofcontinuouspassivemotion islackingdespiteanoverwhelmingabundanceofbasic sci-encesupportandthecommonclinicalpracticeofcontinuous passivemotionimplementationpostoperativelyinknee carti-lagerestorationprocedures.20Themostcommonlyprescribed parameterswithinaContinuouspassivemotionregimenare initiatedonthefirstpostoperativeday,withaninitial range-of-motionof0–30◦ and a frequencyof1 cycle per minute, appliedforsixtoeighthoursdailyoversixweeks.21Studies havedemonstratedthatcontinuouspassivemotionfacilitates therepairoffull-thicknessdefectsinarticularcartilage.22,23
Thepatientsevaluatedinthisstudyhadanormalpassive rangeofmotionduringthesix-monthperiodaftertheSCI, buttheypresentedarticularcartilagedamage.Thisresultmay haveoccurredbecauseanormalrangeofmotionwithout mus-clecontractionisnotsufficienttomaintainthenutritionand structuralpropertiesofthecartilage.
Ourstudyhassomelimitations.First,therewereonlytwo patientsincluded inthe finalsix-month MRI study.Asthe MRIwasperformedforresearchpurposesnotrelatedtotheir spinalcordinjury,wehaddifficultyenrollingpatients.Most patientsindicatedthatthelogisticsofundergoingkneeMRI arenoteasyconsideringtheirphysicallimitations.Second, weperformedtime-zeroandsix-monthMRIsonly,whichdoes notprovideinformationonthe timeatwhich thecartilage alterationsbegantooccur.Weconsiderthatperformingknee MRIsforresearchpurposesintheinitialthreemonthsaftera traumaticspinalcordlesionwouldhaveverylowacceptance amongpatientsandtheirrelatives.
Conclusion
Theabsenceofmusclecontractionsseemstobedeleteriousto normalhumankneecartilageeveninthepresenceofa nor-malrangeofmotion.Furtherstudies withalargernumber ofpatients,despitetheirhighlogisticalcomplexity,mustbe performedtoconfirmthishypothesis.
Conflict
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.VanwanseeleB,LucchinettiE,StüssiE.Theeffectsof immobilizationonthecharacteristicsofarticularcartilage: currentconceptsandfuturedirections.OsteoarthrCartil. 2002;10(5):408–19.
2.TorzilliPA,BhargavaM,ParkS,ChenCT.Mechanicalload inhibitsIL-1inducedmatrixdegradationinarticularcartilage. OsteoarthrCartil.2010;18(1):97–105.
3.KocinaP.Bodycompositionofspinalcordinjuredadults. SportsMed.1997;23(1):48–60.
4.WhiteneckGG,CharlifueSW,FrankelHL,FraserMH,Gardner BP,GerhartKA,etal.Mortality,morbidity,andpsychosocial outcomesofpersonsspinalcordinjuredmorethan20years ago.Paraplegia.1992;30(9):617–30.
5.VanwanseeleB,EcksteinF,KnechtH,StüssiE,SpaepenA. Kneecartilageofspinalcord-injuredpatientsdisplays progressivethinningintheabsenceofnormaljointloading andmovement.ArthritisRheum.2002;46(8):2073–8. 6.McKeeP,HannahS,PrigancVW.Orthoticconsiderationsfor
denseconnectivetissueandarticularcartilage–theneedfor optimalmovementandstress.JHandTher.2012;25(2):233–42. 7.O’HaraBP,UrbanJP,MaroudasA.Influenceofcyclicloading
onthenutritionofarticularcartilage.AnnRheumDis. 1990;49(7):536–9.
8.KnapikDM,HarrisJD,PangrazziG,GriesserMJ,SistonRA, AgarwalS,etal.Thebasicscienceofcontinuouspassive motioninpromotingkneehealth:asystematicreviewof studiesinarabbitmodel.Arthroscopy.2013;29(10):1722–31. 9.KijowskiR,BlankenbakerDG,MunozDelRioA,BaerGS,Graf
BK.Evaluationofthearticularcartilageofthekneejoint: valueofaddingaT2mappingsequencetoaroutineMR imagingprotocol.Radiology.2013;267(2):503–13. 10.KaraM,TiftikT,ÖkenÖ,AkkayaN,TuncH,Özc¸akarL.
ltrasonographicmeasurementoffemoralcartilagethickness inpatientswithspinalcordinjury.JRehabilMed.
2013;45(2):145–8.
11.FindikogluG,GunduzB,UzunH,ErhanB,RotaS,ArdicF. Investigationofcartilagedegradationinpatientswithspinal cordinjurybyCTX-II.SpinalCord.2012;50(2):136–40. 12.RuckstuhlH,KrzyckiJ,PetrouN,VanwanseeleB,StussiE.A
quantitativestudyofhumeralcartilageinindividualswith spinalcordinjury.SpinalCord.2008;46(2):129–34.
13.MoriyamaH,YoshimuraO,KawamataS,TakayanagiK, KuroseT,KubotaA,etal.Alterationinarticularcartilageof ratkneejointsafterspinalcordinjury.OsteoarthrCartil. 2008;16(3):392–8.
14.VanwanseeleB,PirnogC,SzékelyG,StüssiE.Quantitative analysisoflocalchangesinpatellarcartilageinspinalcord injuredsubjects.ClinOrthopRelatRes.2007;456:98–102. 15.MühlbauerR,LukaszTS,FaberTS,StammbergerT,EcksteinF.
transplantation.Aretrospectivestudyofhumanpatella cartilagedefecttreatment.KneeSurgSportsTraumatol Arthrosc.1999;7(4):232–8.
17.MarderRA,HopkinsGJr,TimmermanLA.Arthroscopic microfractureofchondraldefectsoftheknee:acomparison oftwopostoperativetreatments.Arthroscopy.
2005;21(2):152–8.
18.RodrigoJJ,SteadmanJR,SillimanJF,FulstoneHA.
Improvementoffull-thicknesschondraldefecthealinginthe humankneeafterdebridementandmicrofractureusing continuouspassivemotion.AmJKneeSurg.1994;7:109–16. 19.SchultzW,GöbelD.Articularcartilageregenerationofthe
kneejointafterproximaltibialvalgusosteotomy:a
surgery:asystematicreview.Orthopedics.2010;33(12): 878.
21.KarnesJM,HarrisJD,GriesserMJ,FlaniganDC.Continuous passivemotionfollowingcartilagesurgery:doesacommon protocolexist?PhysSportsmed.2013;41(4):53–63.
22.WilliamsJM,MoranM,ThonarEJ,SalterRB.Continuous passivemotionstimulatesrepairofrabbitkneearticular cartilageaftermatrixproteoglycanloss.ClinOrthopRelat Res.1994;(304):252–62.