SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Hip
disarticulation
–
case
series
analysis
and
literature
review
夽
Diogo
Lino
Moura
∗,
António
Garruc¸o
CentroHospitalareUniversitáriodeCoimbra,DepartamentodeOrtopedia,Coimbra,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14February2016 Accepted1September2016 Availableonline3March2017
Keywords: Hipjoint Disarticulation Amputation Lowerextremity Infection Tumor
a
b
s
t
r
a
c
t
Objective:Topresentaretrospectivestudyof16patientssubmittedtohipdisarticulation. Methods:Duringtheperiodof16years,16patientswhounderwenthipdisarticulationwere identified.Allofthemwerestudiedbasedonclinicalrecordsregardingthegender,ageat surgery,disarticulationcause,postoperativecomplications,mortalityratesandfunctional statusafterhipdisarticulation.
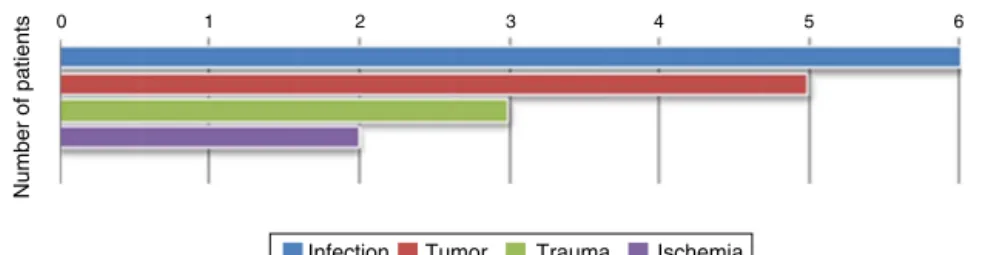
Results:Hipdisarticulationwasperformedelectivelyinmostcasesandurgentlyinonly threecases.Theindicationshadthefollowingorigins:infection(n=6),tumor(n=6),trauma (n=3),andischemia(n=2).Themeanpost-surgerysurvivalwas200.5days.Thesurvival rateswere6875%aftersixmonths,5625%afteroneyear,and50%afterthreeyears.The mortalityrateswerehigherindisarticulationswithtraumatic(66.7%)andtumoral(60%) causes.Regardingtheeightpatientswhosurvived,halfofthemambulatewithcrutchesand withoutprosthesis,25%walkwithlimbprosthesis,and25%arebedridden.Complications andmortalitywerehigherinthecasesofurgentsurgery,andinthosewithtraumaticand tumoralcauses.
Conclusion:Hipdisarticulationisamajorablativesurgerywithobviousimplicationsforlimb functionality,aswellashighratesofcomplicationsandmortality.However,whenperformed atthecorrecttimeandwithproperindication,thisprocedurecanbelife-savingandcan ensurethereturntothehomeenvironmentwithacertaindegreeofqualityoflife.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheCentroHospitalareUniversitáriodeCoimbra,DepartamentodeOrtopedia,Coimbra,Portugal.
∗ Correspondingauthor.
E-mails:[email protected],[email protected](D.L.Moura). http://dx.doi.org/10.1016/j.rboe.2016.09.008
Desarticulac¸ão
da
anca
–
Análise
de
uma
série
e
revisão
da
literatura
Palavras-chave: Articulac¸ãodaanca Desarticulac¸ão Amputac¸ão Extremidadeinferior Infec¸ão
Tumor
r
e
s
u
m
o
Objetivo:Apresentarumestudoretrospectivoem16pacientessubmetidosadesarticulac¸ão daanca.
Métodos: Foramidentificados16pacientessubmetidosadesarticulac¸ãodaancaaolongo de16anos.Todosforamestudadospormeiodosregistosclínicosquantoasexo,idadena cirurgia,causadadesarticulac¸ão,complicac¸õesnopós-operatório,índicesdemortalidade egraudefuncionalidadeapósadesarticulac¸ãodaanca.
Resultados: Adesarticulac¸ãodaancafoifeitaeletivamentenamaioriadassituac¸õese ape-nasdeformaurgenteemtrêscasos.Asindicac¸õestiveramasseguintesorigens:infecc¸ão (n=6),tumor(n=5),traumatismo(n=3)eisquemia(n=2).Otempomédioglobalde sobre-vivênciapós-cirurgiafoide200,5dias.Osíndicesdesobrevivênciaforamde68,75%após seismeses,56,25%apósumanoede50%apóstrêsanos.Osíndicesdemortalidadeforam maiselevadosnasdesarticulac¸õesdecausatraumática(66,7%)edecausatumoral(60%).Em relac¸ãoaosoitopacientesquepermanecemvivos,metadefazmarchacomapoiodemuletas canadensesesemprótese,25%fazemmarchacommembroprotéticoe25%encontram-se acamados.Astaxasdecomplicac¸õesemortalidadeforammaiselevadasnasdesarticulac¸ões urgentesenasefetuadasemconsequênciadetraumatismosetumores.
Conclusão: Adesarticulac¸ãodaancaéumacirurgiaaltamentemutilante,comimplicac¸ões óbviasnafuncionalidadedomembroetaxaselevadasdecomplicac¸õesemortalidade.No entanto,quandoefetuadoemummomentoadequadoecomindicac¸ãocorreta,esse pro-cedimentopodesalvaravidadopacienteegarantiroseuregressoaodomicíliocomalguma qualidadedevida.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Hip disarticulation is the amputation of the lower limb throughthehipjoint;itcontinuestobeoneofthemost radi-calproceduresinorthopedicsurgery.1,2Thissurgeryaccounts
onlyforapproximately0.5%oflowerlimbamputations.1The
mostfrequentindicationsarehighlyinvasivetumorsofthe musculoskeletalsystemthatareunresectablewithlimb con-servation,limbischemia,trauma,andseveremusculoskeletal infectionsofthepelvicregionand/orgroin.1
Material
and
methods
The authors present a series of 16 patients who under-wenthipdisarticulationoveraperiodof16years(1999–2015) at this institution, which includes centers dedicated to tumorsandsepticpathologyofthemusculoskeletalsystem. All patientswere characterizedand studied retrospectively through clinical records regarding gender, age at surgery, causeofdisarticulation,postoperativecomplications, mortal-ityrates,anddegreeoffunctionalityafterhipdisarticulation. Thevariables were analyzedusing SPSS, version23, and a 0.05significancelevelwasadopted.Quantitativevalueswere presentedasmean,minimum value,maximum value,and standarddeviation,whilequalitativevalueswere described asnumber (n) and percentage(%). For the comparisons of qualitativevariablesbetweengroups,thechi-squaredtestwas used,whiletheMann–Whitneytestwasusedforquantitative
variables.ThisstudywasapprovedbytheEthicsCommittee oftheCentroHospitalareUniversitáriodeCoimbra,andall patientsortheirrespectivefamiliessignedaninformed con-sentform.
Results
Sample comprised of 16 patients, nine males and seven females,withameanageof61.25years(29–87).Disarticulation surgerywasperformedaccordingtothetechniquesdescribed in the literature.3,4 Afterisolating and ligatingthe femoral
0
Number of patients
1 2 3 4 5 6
Infection Tumor Trauma Ischemia
Fig.1–Reasonsforhipdisarticulation.
Table1–Descriptionoftheseriesofhipdisarticulations.
Cause Frequency (number)
Frequency (percentage)
Urgent dislocations (percentage)
Meanpost-surgerysurvival inpatientswhodied(days)
Mortality (percentage)
Complications
Infection 6 37.50 0 171.5 33.33 33.33
Tumor 5 31.25 0 416 60 60
Trauma 3 18.75 66.67 3 66.67 33.33
Ischemia 2 12.50 50 7 50 50
chondrosarcoma (n=3), pleomorphic sarcoma of the thigh (n=2),andbasalcelltumors(n=1).
The three polytraumatized patients in this series had extensiveslough inthe pelvisand thigh, withmulti-organ injuriesandneedformultidisciplinarytreatment.Allofthem showedhemodynamicinstabilityandonlyonesurvivedpast thefirstpostoperativeweek.Thecausesofischemiaverifiedin thesamplewereacutearterialischemiaduetofemoral arte-rialthromboembolismandiatrogeniclesionofthecommon femoralartery. Inthreepatients,onewithtraumaticlesion andtwowithischemiclesions,asupracondylaramputation ofthe femurwas initially performed, which, due to unfa-vorableevolutionandsuperinfection,ledtotheneedforhip disarticulation.Complicationswereobservedpostoperatively insevenpatients(43.75%),mainlysuperficialinfections(n=5), suturedehiscence(n=2),necrosisoftheamputationstump scar(n=2),and metastasisoftheamputationstump(n=1). Complicationsweremorecommonlyobservedin disarticu-lationsduetotumors(60%),whichcorrespondstothegroup withthelongestpost-surgicalsurvivaltime(416days).Atrend forhigherratesofcomplicationsinemergencysurgerieswhen compared with elective (66.67% vs. 38.50%) was observed, but withoutstatistical significance(p=0.55). Ahigher com-plicationrateinindividualswhounderwentsurgerypriorto disarticulationwasnotobserved.
Meanoverall post-surgicalsurvivaltimewas200.5days; whenthismanuscriptwasdrafted,onlyhalfofthepatients inthe samplewere alive.Survival rates were 68.75% after six months, 56.25% after one year, and 50% after three years. Mortality rates were higher in disarticulations due to trauma (66.7%)and tumor (60%). For the eightpatients who had died when this review was drafted, there was a tendency for lower survival time inthose who underwent emergency surgery (4.33±3.79 days) when compared with electivesurgery(318.20±318.01days),butwithoutstatistical significance(p=0.14).Inpatientswhoarealive,themost com-monreasonfordisarticulationwasinfection(50%),followed bytumor(25%);therewasonlyonecaseofischemiaandone caseoftrauma.
Meanlifeexpectancyofthosewhosurvivedformorethan three months after surgery was 205.5 days for bedridden patientsand588daysforthosewhowereabletowalk.Half ofthepatientswalkwithcrutcheswithoutprosthesisdueto intolerance to it,25% walkwithprosthetic limbs, and 25% arebedridden.Inthesixpatientswhoareabletowalk,the mostfrequentreasonfordisarticulationwasinfection(50%), followedbytumor(33.33%).Allthesepatientshavefrequent eventsofphantompainrequiringmedicaltreatment.
Discussion
Hipdisarticulationisacomplexandinfrequentsurgery,only performedasthelastoptioninextremecases.1,5Theliterature
onthissurgeryisscarce,mainlyintheformofcasereportsand smallseries.5Areviewofthemostrelevantarticlesrelatedto
hipdislocationsispresentedbelow.
Endeanetal.6analyzedaseriesof53hipdislocations
mortality rate was significantly higher in urgent surgeries (33%)whencomparedwithelectivesurgeries(4%).Presence of ischemia associated with limb infection and heart dis-easewasthegreatestpredictorofmortality.DénesandTill7
analyzedaseriesof63dislocations,whoseindicationswere arterialischemia(n=34),tumor(n=24),andinfection(n=4). Surgical wound complications were observed in 64.86% of the patients whosedisarticulation had vascular cause and in20.83%ofthose withtumorcause.Themortalityrate in thefirst postoperativemonth rangedfrom 43.24%inthose withavascular cause to0%inthose causedbytumor. All patientswhounderwentdisarticulationduetoatumorwere able to walk with a prosthetic limb; in contrast, of those whoseetiologywasvascular,onlytwousedprosthesesand 19becamewheelchair-dependent.Unruhetal.8presenteda
seriesof38hipdislocationsover11yearsofexperience.Four patientsweredisarticulatedbilaterallyand20ofthe disartic-ulationsoccurredinapreviouslyamputatedlimb,13ofthem duringthesamehospitalizationperiod.Indicationsfor disar-ticulationswereischemiasecondarytoatherosclerosis(n=17), femoralosteomyelitis(n=10),andtrauma(n=11).Theauthors reportedpost-operativeinfections(63%)asthemostfrequent complication.Inthepostoperativeperiod,septicshock(21%), hemorrhagicshock(11%),disseminatedcoagulopathy(11%), acuterenalfailure (24%),and cardiac(26%)and pulmonary (24%)dysfunctionswereobserved.Meanmortalityratewas 44%:60%incasesofischemiaassociatedwithinfection,20% incasesofischemiawithoutinfection,22%incasesoffemoral osteomyelitis,100%incasesoftraumaassociatedwith infec-tion,and 33% incases oftraumawithout infection. Those authors stated that the presenceof preoperative infection tripledtheriskofdeathafterhipdisarticulation.Regarding functionality,theyobservedthatnoneofthe19survivorswere abletousetheprostheticlimb,onlyfourwereabletowalk withawalker,12werewheelchair-dependent,andthreewere bedridden.Fenelonetal.9presentedaseriesof11
disarticula-tionssecondarytoinfectioncomplicationsofhiparthroplasty. Indicationsfordisarticulationwereseverefistulizingsoft tis-sueand femurinfections, onecaseofpronouncedfemoral boneloss,and onecaseofrupturedfalseaneurysmofthe externaliliac artery.Disarticulationwasurgentinsixcases andelective intheremainder;no deathswere observedin theperioperativeperiod.Themostcommonlyfound microor-ganismswereStaphylococcusaureus,Pseudomonas,andProteus; 81.82%ofthedisarticulatedpatientshadalreadyundergone fourormorehiparthroplastyrevisionsurgeries.Theauthors suggest that some dislocations could have been avoided if a resection arthroplasty had been performed instead of repeatedprosthesisrevisions.Assessingthefunctionalresults oftheeightsurvivorsatthetimeofthereview,sixpatients wereabletowalk,fourwithwalkersandtwowithprosthetic limbs,andtwowerebedridden.Therewerealsothreecasesof surgicalwoundcomplicationsandtwocasesofphantompain. LászlóandKullmann10studied29hipdislocationsofischemic
originandalsofoundahighrateofsurgicalwound complica-tions.Healingbyfirstintentiononlyoccurredintwocases; scarringby second intention with superficial necrosiswas observedin13cases,andtherewere12casesofdeep necro-sis.Themortalityrateintheperioperativeperiodwas37%. Onlytwopatientsregularlyusedtheprostheticlimb.Itwas
observedthatthemortalityratewashigherwhenpatientshad undergonepreviousdistalamputations.Mostofthepatients had undergoneamean of2.3priordistalamputations and 2.9conservativelimbsurgeries.Theseauthorsconcludedthat surgicalaggression increasesthe riskofmortalityand that amputationmustfirstbeperformedattheappropriatelevel, soasnottosubjectthepatienttoseveralsurgeries.Another studyof15dislocationsduetoinfection,sevendueto necro-tizinginfectionsandeightduetopersistentinfectionsofthe proximalthigh, indicatedthatthemostcommonpathogen wasStaphylococcusaureus,presentineightpatients.5
Surger-ieswereelectiveineightpatientsandemergenciesinseven. Allpatientssurvivedsurgery;onlyonedeathwasrecorded,on the29thdayafterdisarticulation.5Theauthorsconcludedthat
hipdisarticulationastreatmentofsevereinfectionsofthehip andgroincanresultinhighlevelsofsurvival,evenincases ofemergencysurgery,andtheyattributetheseresultsto mul-tidisciplinaryinvolvement,andtotheexperienceinsurgical andpost-surgicaltreatmentperformedintheintensivecare unitattheirinstitution.5Jainetal.11studied80dislocations,
exclusively duetotumor, and foundthatthe predominant histologictypeswereosteosarcoma(n=27),chondrosarcoma (n=8),leiomyosarcoma(n=8),andliposarcoma(n=6).In52.5% ofthecases,disarticulationwasperformedasthefirstsurgery, whileintheremainder,surgerywasperformedduetolocal recurrenceafteranattemptoflimb-sparingsurgery.The five-yearsurvivalrateofprimarydisarticulationwas32%,whilefor localrecurrenceitwas25%.Thereweretencasesoflocal recur-renceafterdisarticulationwithinadequateresectionmargins. Of the 11 patients who answered the questionnaire about functionality,onlyonewasabletouseaprostheticlimb regu-larly;eightpatientsreportedphantompain.
Inthepresentsample,weobservedthatmost disarticula-tionsduetoinfectionoccurredinthecontextofpatientswith largetumorprostheses,whichisinagreementwithhigher riskofthesereconstructionstodevelopinfection,notonlydue tothelengthandsurgeryduration,butalsotothe immuno-compromisedstatusofpatients.12Predictably,complications
after hip disarticulationare frequent, not only due to the extent of surgery, but also because patients often present extremesituations,withmultiplecomorbiditiesand hemody-namicinstability.Theliteraturepresentscontroversialresults onmortalityafterhipdisarticulation;theratesvaryaccording totheindication,clinicalstatusofthepatient,andthedegree ofurgencyofthesurgery.6–10Inthepresentstudy,itisevident
thatthebestsurvivalrateswereobservedinelectivesurgery, particularlyininfectiousandtumorcauses.Conversely,severe polytraumapatients,inemergencysituationsandoften asso-ciatedwithhemodynamicinstability,presenttheworstresults intermsofsurvivalandmortalityrate.Thefewstudiesthat analyze functional results afterhip disarticulation demon-stratedthatpatientspresentpoorqualityoflifeandsignificant difficultiesintherecoveryofthegaitandintheuseof sub-stitution prosthesisforthelower limb.7–9,11,13,14 Theenergy
expenditure forgaitinpatientsundergoinghip disarticula-tionincreasesby82%,thusthepatientisoftenconfinedtoa wheelchairorbedridden.5,8,15Furthermore,Nowroozietal.15
presentstudy,ashalfofthesurvivorswalkwithcrutches with-outtheuseoftheprostheticlimb,whileonly25%canusethe prosthesis.DénesandTill.7reportedthatfunctionalsuccess
dependsonthecauseofdisarticulationandadvocatethat,in general,thoseduetotumorandtraumaarebettersuitedto gaitthanthoseduetovascularconditions.Inthepresent sam-ple,themostcommonreasonsfordisarticulationinpatients whoarecurrentlyabletowalkwereinfectionandtumors;the onlylivingpatientwithanischemicconditionisbedridden. Individualmotivation,age,overallhealthstatus,and comor-biditiesofthepatientareconsideredtobecrucialfactorsfor recoveryofgait.11
Thelimitationsofthepresentstudywerethesmallnumber ofindividualsinthesampleandthefactthatitwasa retro-spectiveobservationalstudy.Largersamplescouldprobably changesomeofthestatisticaltrendsintostatistically signifi-cantdifferences.
Conclusions
Hip disarticulation is a highly mutilating and last-resort surgery,withobviousimplicationsforlimbfunctionalityand highratesofcomplicationsandmortality.However,when per-formedinthepropertimewindowandwithcorrectindication, it isa life-saving surgerythat allowsthe patient toreturn home.Forthesuccessofthissurgicalprocedure,early identi-ficationofhipdisarticulationindicationsisparamount;soas nottopostponeanunavoidablesituationand consequently aggravatetheprognosis.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. DillinghamTR,PezzinLE,MacKenzieEJ.Limbamputation andlimbdeficiency:epidemiologyandrecenttrendsinthe UnitedStates.SouthMedJ.2002;95(8):875–83.
2.KaufmanMH,WakelinSJ.Amputationthroughthehipjoint duringthepre-anaestheticera.ClinAnat.2004;17(1): 36–44.
3.BoydHB.Anatomicdisarticulationofthehip.SurgGynecol Obstet.1947;84(3):346–9.
4.SugarbakerPH,ChretienPB.Asurgicaltechniqueforhip disarticulation.Surgery.1981;90(3):546–53.
5.ZalavrasCG,RigopoulosN,AhlmannE,PatzakisMJ.Hip disarticulationforseverelowerextremityinfections.Clin OrthopRelatRes.2009;467(7):1721–6.
6.EndeanED,SchwarczTH,BarkerDE,MunfakhNA, Wilson-NeelyR,HydeGL.Hipdisarticulation:factors affectingoutcome.JVascSurg.1991;14(3):398–404. 7.DénesZ,TillA.Rehabilitationofpatientsafterhip
disarticulation.ArchOrthopTraumaSurg.1997;116(8): 498–9.
8.UnruhT,FisherDFJr,UnruhTA,GottschalkF,FryRE,Clagett GP,etal.Hipdisarticulation.An11-yearexperience.Arch Surg.1990;125(6):791–3.
9.FenelonGC,VonFoersterG,EngelbrechtE.Disarticulationof thehipasaresultoffailedarthroplasty.Aseriesof11cases.J BoneJointSurgBr.1980;62(4):441–6.
10.LászlóG,KullmannL.Hipdisarticulationinperipheral vasculardisease.ArchOrthopTraumaSurg.1987;106(2): 126–8.
11.JainR,GrimerRJ,CarterSR,TillmanRM,AbuduAA.Outcome afterdisarticulationofthehipforsarcomas.EurJSurgOncol. 2005;31(9):1025–8.
12.GraciC,MaccauroG,MuratoriF,SpinelliMS,RosaMA, FabbricianiC.Infectionfollowingbonetumorresectionand reconstructionwithtumoralprostheses:aliteraturereview. IntJImmunopatholPharmacol.2010;23(4):1005–13.
13.DaigelerA,LehnhardtM,KhadraA,HauserJ,SteinstraesserL, LangerS,etal.Proximalmajorlimbamputations–a
retrospectiveanalysisof45oncologicalcases.WorldJSurg Oncol.2009;7:15.
14.EbrahimzadehMH,KachooeiAR,SoroushMR,Hasankhani EG,RaziS,BirjandinejadA.Long-termclinicaloutcomesof war-relatedhipdisarticulationandtranspelvicamputation.J BoneJointSurgAm.2013;95(16):e114,1-6.