Introduction
Injuries prevalence in elite male artistic gymnasts
CDD. 20.ed. 796.024 796.41
http://dx.doi.org/10.1590/1807-55092016000100079
Natália Batista Albuquerque GOULART* Morgana LUNARDI** Jennifer Faraon WALTRICK*** Annelise LINK*** Leandro GARCIAS*** Mônica de Oliveira MELO*** João Carlos OLIVA**** Marco Aurélio VAZ****
*Colegiado de Educa-ção Física, Universi-dade Federal do Vale do São Francisco, Petrolina, PE, Brasil. **Centro de Desportos, Universidade Federal de Santa Catarina, Flo-rianópolis, RS, Brasil. ***Centro de Ciências Biológicas e da Saú-de, Universidade de Caxias do Sul, Caxias do Sul, RS, Brasil. ****Escola de Educa-ção Física, Universi-dade Federal do Rio Grande do Sul, Porto Alegre, RS, Brasil.
Men’s artistic gymnastic (AG) is featured by the executions of high complexity skills to be performed in six diff erent apparatus: fl oor exercise, pommel horse, rings, vault, parallel bars, and horizontal bar1. In recent years, AG has shown great evolution due to materials and apparatus development, as well as to training methods improvement2-3. Such changes have increased the number of participants, due to a more attractive sport. However, improve in performance has been a result from more diffi cult elements created by the athletes (sometimes with the athlete’s name being given to a specifi c movement). In addition, a more strict scoring system has resulted from these
material, technical and performance improvements. All these factors might lead to a higher injury risk4-5.
According to Nunomura4, each apparatus presents unique characteristics. Injuries are related to the movements performed on these apparatus, as well as to insuffi cient training, guidance and protection given to the gymnasts. However, the literature lacks a systematic study looking at the mechanisms and incidence of sports injury. Epidemiological studies in sports injuries are important strategies to identify risk factors and to set preventive measures against these injuries6-8. Th e literature presents a wide range of studies on the prevalence of injuries among female
Abstract
The purpose of this study was to investigate the injuries prevalence in men elite artistic gymnasts. Twenty Brazilian senior gymnasts, aged 23.1 ± 6.5 years, 13.9 ± 5.0 years of practice and 36.5 ± 4.7 hours per week training, participated in this study. The athletes answered a morbidity questionnaire, formulated according to studies from the literature, for information on the injuries’ characteristics and circumstances. Information about the injury circumstances (gymnastic apparatus, overload training and physical exercises), the anatomic site injured, the affect biological tissue and the return to training after injury treatment were evaluated. Data were analyzed by descriptive statistics, absolute and relative frequencies. The training overload, and fl oor, pommel horse and vault were the events that presented higher injuries frequency. In relation to anatomic site, ankle, hands/fi ngers and shoulder were the most cited regions. The ligament, bone and articular capsule were the most affected biological tissues. In relation to gymnasts’ return to their sports activities, 56% of them reported a better condition at return, 33% reported to have returned at the same fi tness level and 10% indicated that they were in a worse condition when they returned to the sports activities. The men’s artistic gymnastics injuries are related to the mechanical demands of this sport. The analysis of risk factors helps in understanding the injuries mechanisms in gymnastics, and provides relevant information that can assist in effective prevention strategies.
gymnasts. However, these studies rarely address injury occurrence in males. Th us, the current study aims to investigate the prevalence of injuries in men’s artistic
Method
Athletes had an average training time of about 14 years, with more than 35 hours of training per week (TABLE 1).
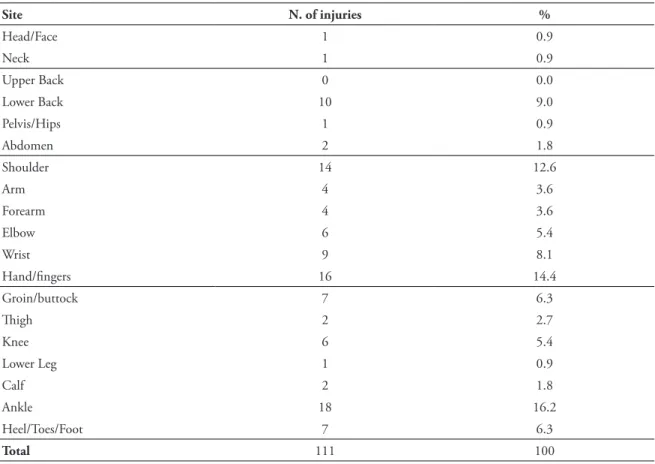
Injuries were located at the forearm (36%), ankle joint (16.2%), hand and fi ngers (14.4%), shoulder (12.6%), lower back (9.0%), wrist (8.1%) and groin/buttock and heel/toes/foot (6.3%), elbow and knee (5.4%) (TABLE 2).
According to the event, injuries were distributed on Floor (23.4%), Pommel Horse (11.7%), A total of 20 Brazilian senior men gymnasts participated in the current study. Th e gymnast group consisted of high performance (elite) gymnasts at national competition level. Th e present investigation was approved by the Ethics Committee on Human Research from the Federal University of Rio Grande do Sul (CAAE: 1 0059712.9.0000.5347). All gymnasts and trainers (in the case of young gymnasts) signed the informed consent form to participate in the study. Th e athletes answered a morbidity questionnaire used to identify the injuries prevalence. Th e questionnaire was formulated according to epidemiological descriptive studies on gymnastics athletes found in the literature5-8. Interviews were conducted at the time the injury occurred or thereafter, during artistic gymnastic competitions or training sessions. Th e questionnaire included personal information such as age, time of training (in years) and weekly training hours. Athletes recorded injury information about its anatomical location, circumstance of injury (gymnastic apparatus) and about their return to training activities after injury treatment. In order to better classify the collected data, injuries were separated according to
gymnastics, the gymnastic apparatus at which the injury occurred, the anatomical sites and the most aff ected biological tissues of these injuries.
the aff ected biological tissue, using the following classifi cation: bone injury, cartilage injury, ligament injury, tendon injury, muscle injury and capsular injury. In addition, two events found in the training routine were added to evaluate injury prevalence at the men’s apparatus: overload training (related to repetitive eff ort of the musculoskeletal system due to gymnastic training) and warm up/physical preparation exercises. Th e participants answered the questions and the investigator, who was also in charge of making notes in the questionnaire, conducted the procedure.
On the current study, injury was considered as any gymnastics-related incident resulting from training and/or competition and able to cause the athlete’s temporary suspension from the training routine or modifi cation of all or part of his training as well as the need for medical treatment for at least a month8. Recorded data were systematically organized on Excel spreadsheets for analysis. Data on the injuries prevalence, their anatomical site, as well as the gymnastic apparatus where they occurred, were analyzed using descriptive statistics by absolute and relative frequencies distribution.
Results
Rings (8.1%), Parallel Bars and Horizontal Bars (7.2%), and Vault (11.7%). Overload Training was responsible for 27% of the injuries, whereas Warm up/Physical Exercises accounted for 3.6% (TABLE 3).
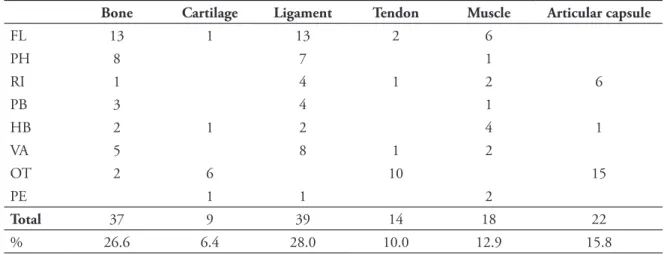
Regarding the biological tissues that were mostly aff ected, ligament injuries had the highest relative incidence (28%), followed by bone (26.6%), articular capsule (15.8%), muscle (12.9%), tendon (10%) and cartilage (6.4%) (TABLE 4).
TABLE 1 - Gymnasts’ age, training experience and training time variables.
Age Training time Weekly hours
TABLE 2 - Absolute (n) and relative (%) injuries distribution regarding their anatomical site.
Site N. of injuries %
Head/Face 1 0.9
Neck 1 0.9
Upper Back 0 0.0
Lower Back 10 9.0
Pelvis/Hips 1 0.9
Abdomen 2 1.8
Shoulder 14 12.6
Arm 4 3.6
Forearm 4 3.6
Elbow 6 5.4
Wrist 9 8.1
Hand/fi ngers 16 14.4
Groin/buttock 7 6.3
Th igh 2 2.7
Knee 6 5.4
Lower Leg 1 0.9
Calf 2 1.8
Ankle 18 16.2
Heel/Toes/Foot 7 6.3
Total 111 100
FL: Floor; PH: Pommel Horse; RI: Rings; PB: Parallel Bars; HB: Horizontal Bars; VA: Vault;
OT: Overload Training; PE: Warm up/ Physical Exercises.
TABLE 3 - Absolute (n) and relative (%) injuries distribution according to the event.
Site FL PH RI PB HB VA OT PE
Head/Face 1
Neck 1
Upper Back
Lower Back 1 1 8
Pelvis/Hips 1
Abdomen 2
Shoulder 4 2 8
Arm 1 1 1 1
Forearm 2 2
Elbow 2 1 3
Wrist 4 1 4
Hand/fi nger 2 6 4 3 1
Groin/buttock 3 2 1 1
Th igh 1 1
Knee 3 1 1 1
Lower Leg 1
Calf 1 1
Ankle 7 1 2 1 1 6
Heel/Toes/Foot 5 2
Total Injuries 26 13 9 8 8 13 30 4
AG is associated with intensive movement repetition to achieve a precise execution of the different exercises. Moreover, in recent years, complexity increased in their implementation and motor demand, fact that determined an increase in daily training hours2,6. In this study, injuries caused by overload training presented the highest percentage of reports. Daly et al.9 reported that fatigue was a
major factor contribution to injury in elite gymnasts. Th ey are more often found at the shoulders and in the lower back. Micheli and Allison10 reported
that lower back injuries are usually related to acute microtrauma (single traumatic event) or successive microtrauma events (overuse). Such events result from repetitive fl exions and extensions due to spine rotation in gymnastics movements. AG, just as other sports, works with an intense calendar of important competitions. Sometimes the athlete does not have time to physically recover for the next competition, as it is required.
In addition to overload training, fl oor, pommel horse and vault also lead to high injury occurrence, respectively. Floor is the most complex AG apparatus and it is composed of acrobatic elements combined with gymnastic strength and balance exercises11.
Floor exercise demands are linked to strength (muscle power in the lower and upper limbs), fl exibility, and muscular anaerobic endurance. It may be noticed that injuries caused by this device are found in diff erent joints due to its complexity and the injuries are mostly concentrated in the lower limbs4,6. On the
other hand, the pommel horse predominantly uses
Discussion
TABLE 4 - Events related to artistic gymnastic training and the affected biological tissue.
Bone Cartilage Ligament Tendon Muscle Articular capsule
FL 13 1 13 2 6
PH 8 7 1
RI 1 4 1 2 6
PB 3 4 1
HB 2 1 2 4 1
VA 5 8 1 2
OT 2 6 10 15
PE 1 1 2
Total 37 9 39 14 18 22
% 26.6 6.4 28.0 10.0 12.9 15.8
the strength of the upper limbs, since the athlete’s weight is fully supported on the hand11.
Gymnasts must execute all elements without interruptions, which demands high anaerobic and muscular endurance, rhythm and balance on the upper limbs6,11. Th ese exercises may be associated with
the high percentage of injuries in wrists, hands and fi ngers. As for the vault exercise, each vault begins with the preparatory running (25 meters), continues with a take-off from both feet to the springboard, a support phase on the table with two hands (fi rst phase), and the second fl ight phase involves the pushing off from the table up to landing in a standing position12. Th us,
vault leads to high rates of injuries located in the ankle, especially caused by the landing movements6,13.
In relation to anatomic site, ankle, hands/fi ngers and shoulder were the most cited regions. By analyzing the movements performed on each men’s artistic gymnastics unit, it was possible to conclude that the ankle is the most demanded joint in landing, mainly on the fl oor and vault apparatus6,14.
Nunomura4 reports that most ankle injuries
occur due to unsuccessful landing. Th e gymnast must be able to control the ground reaction force, using biomechanical and neuromuscular strategies (biarticular muscle activation) during the landing procedure13-15. According to the literature, teaching
the correct and controlled movement, and using exercises for the lower limbs are important strategies to prevent and minimize injuries15-17.
In addition, hands and fi ngers also present high injury incidence since much of the exercises in men’s
FL: Floor; PH: Pommel Horse; RI: Rings; PB: Parallel Bars; HB: Horizontal Bars; VA: Vault;
devices involve suspension and body support on these structures. According to literature4,8, the hand and
fi nger injuries go from acute events, such as blisters and abrasions, to the most complex ones, such as dislocations and fractures, as it was herein mentioned.
Finally, the shoulder joint is also often injured, mainly due to movements performed in the rings. According to Carrara and Mochigueki18, most movements in the rings require shoulder abduction and consequent capsular compression in order to keep joint stability. Th us, many injuries suff ered in this unit are due to infl ammation in the shoulder joint capsule. Th e current study also aimed to evaluate the tissues presenting the highest injury prevalence in men’s AG. Th e ligament tissue presented the biggest number of cases, usually due to sprains. According to the report of the athletes themselves, these injuries are mostly caused by the fl oor apparatus, and they often occur after successive jumps or incorrect landings6,8. Ligaments, despite being adaptable and fl exible, allow natural movement of the bones they are connected to. Th ey do not present major force resistance under sprain loads19. Th us, it results in the partial rupture of this tissue and in the longer overall time required to treat it.
In addition to the ligament tissue, bone tissue injuries were also quite cited by the athletes. According to the results, they occur due to fractures in the feet, toes as well as in the hands and fi ngers. Bone tissue is a specialized structural tissue and its solid composition adapts to the support functions and to its protection20.
According to the literature, bone injuries have aff ected athletes due to the strong impact of the exercises required by the artistic gymnastics6,20. Th erefore, it
is worth teaching right landing technique, since the movement must be done on both feet or on both hands in order to dissipate power impact on the structures13,16.
Finally, the injuries in the articular capsule are also among the three most cited tissues and it is due to the overload training and, in some cases, to specifi c ring exercises, as it was previously mentioned. Among this group of injuries, it is worth highlighting those located in the anterosuperior top and on the posterosuperior shoulder labrum (SLAP). Th ese injuries usually occur in the insertion zone, over the biceps tendon, due to the biomechanical overload exerted by the shoulders rotation and abduction movements21-22. Carrara and Mochigueki18 report that many athletes present shoulder instability, thus training sessions should involve strengthening of shoulder muscles that are related to dynamic stabilization of this joint, especially the rotator cuff .
Biological tissue response is infl uenced by tissue age, tissue fatigue, mechanical tissue properties, and other factors19. Th erefore, athletes and coaches must know some clinical aspects that occur in skeletal tissues following trauma, as well as the fact that the aff ected tissue requires diff erent treatment modalities (immobilization, surgical treatments, infi ltrations) to keep the segment from any other injuries. In this study, the athletes reported that some injuries severely aff ected more than one tissue. The injuries in AG show complex etiology; however, Nunomura4 points out that the role played by health professionals such as physical educators, physiotherapists and medical doctors may reduce injury risks and allow faster recovery and the gymnasts’ safe return to sports practice. Besides the basic precautions involving injuries, the biomechanical studies have provided theoretical data in such extent that the skills needed to prevent injury and prolong the athlete’s career in sport are more properly applied.
Regarding the conditions required to the gymnasts’ return to sports practice after treatment, 56% of them have reported better return, 33% reported to have returned at the same fi tness level as pre-injury and 10% have reported to be worse fi tted when they returned to sports practice. During the rehabilitation period, after the injury was healed, the athletes must change their training habits and improve their skeletal tissues conditioning in order to enable their effi cient recovery23. According to
the current study, most athletes reported better conditioning after the recovery period. Such result is linked to the strengthening exercises used in rehabilitation and to reduced training load, as well as to training and improved strengthening techniques.
In the current study, the athletes had diffi culty remembering previous injuries. On the other hand, they reported that it was easier to remember the latest events or those that have marked their careers. In addition, the diffi culty athletes have to be properly diagnosed for certain injuries by clinical professionals was also shown in the current study. Th erefore, it is also important to have the participation of these health professionals (such as physiotherapist or coach) to answer information regarding athletes’ injuries.
The current study presents the following conclusions:
Resumo
Prevalência de lesões na ginástica artística masculina de alto rendimento
A proposta deste estudo foi investigar a prevalência de lesões na ginástica artística masculina de alto rendimento. Vinte ginastas brasileiros da categoria adulta, com 23,1 ± 6,5 anos, 13,9 ± 5,0 anos de prá-tica no esporte e 36,5 ± 4,7 horas de treino semanais, participaram do estudo. Os atletas responderam o questionário de lesões referidas, formulado a partir de estudos da literatura, para obter informações sobre as características e circunstâncias das lesões. Foram considerados dados sobre o aparelho ou evento do treinamento em que ocorreu a lesão, o local anatômico lesionado, o tecido biológico afetado e o retorno às atividades após a lesão. Os dados foram avaliados por meio de estatística descritiva, a partir das fre-quências absolutas e relativas. A sobrecarga de treinamento e os aparelhos solo, cavalo com alças e salto sobre a mesa foram os eventos com maior frequência de lesões. Em relação ao local anatômico, tornozelo, mãos/dedos e ombro foram as regiões mais citadas. Os tecidos ligamentares e ósseo, bem como a cápsula articular foram os tecidos biológicos mais afetados. Em relação ao retorno às atividades, 56% relataram melhora, 33% reportaram retorno ao mesmo nível prévio à lesão e 10% relataram piora do desempenho após retorno às atividades. As lesões na ginástica artística masculina estão associadas às demandas me-cânicas do esporte. A análise dos fatores de risco contribui no entendimento dos mecanismos das lesões na ginástica, bem como pode auxiliar em estratégias efetivas de prevenção.
PALAVRAS-CHAVE: Lesão; Ginástica; Treinamento; Questionário.
References
1. Oliveira MS, Bortoleto MAC. Apontamentos sobre a evolução histórica, material e morfológica dos aparelhos da ginástica artística masculina. Rev Educ Fís. 2011;22:283-95.
2. Nunomura M, Pires RF, Carrara P. Análise do treinamento da ginástica artística brasileira. Rev Bras Cienc Esporte. 2009;31:25-40.
3. Schiavon LM, Paes RR, Toledo E, et al. Panorama da ginástica artística feminina brasileira de alto rendimento esportivo: progressão, realidade e necessidades. Rev Bras Educ Fís Esporte. 2013;227:423-36.
4. Nunomura M. Lesões na ginástica artística: principais incidências e medidas preventivas. Motriz. 2002;8:21-29. 5. Hoshi RA, Pastre CM, Vanderlei LCM, et al. Rev Bras Med Esporte. Lesões desportivas na ginástica artística: estudo a
partir de morbidade referida. Rev Bras Med Esporte. 2008;14:440-45.
6. Caine DJ, Russel K, Lim L. Handbook of sports medicine and science: gymnastics. Oxford: United Kingdom; 2013. - The anatomical sites with highest injury
prevalence in men’s artistic gymnastics are: ankle, hands, fi ngers and shoulders;
- Biological tissues presenting higher injury prevalence in men’s artistic gymnastics are: ligament tissue, bone and articular capsule of the shoulder joint.
Th us, studies focused on analyzing risk factors associated with injuries are critical for a better understanding on the occurrence mechanisms as well as to boost the development of more specifi c prevention programs for AG. Data in the current study showed that injuries in AG mostly occur because of physical stress due to training and/
7. Grigore V, Cosma G, Paunescu M. Retrospective study regarding artistic gymnastic injuries. Procedia Soc Behav Sci. 2014;17:45-49.
8. Dennis C, Kathy K, Warren H, et al. A three-year epidemiological study of injuries aff ecting young female gymnasts.
Phys Th er Sport. 2003;4:10-23.
9. Daly RM, Bass SL, Finch CF. Balancing the risk of injury to gymnasts: how eff ective are the counter measures? Br J Sports Med. 2001;35:8-20.
10. Micheli LJ, Allison G. Lumbar spine injury in the young athlete. Rev Bras Med Esporte. 1999;5:59-65. 11. Nunomura M. Ginástica artística. São Paulo: Odysseus; 2008.
12. Federation Internationale de Gymnastique. Code of points of men’s artistic gymnastic 2013-2016. Lausanne: FIG; 2013. 13. Gittoes MJ, Irwin G. Biomechanical approaches to understanding the potentially injurious demands of gymnastic-style
impact landings. Sports Med Arthrosc Rehabil Th er Technol. 2012;4:1-9.
14. Mcnitt-Gray JL, Mechanical demand and multijoint control during landing depend on orientation of the body seg-ments relative to the reaction force. J Biomech. 2001;34:1471-82.
15. Kirialanis P, Malliou P, Beneka A, et al. Occurrence of acute lower limb injuries in artistic gymnasts in relation to event and exercise phase. Br J Sports Med. 2003;37:137-9.
16. Marinšek M. Basic landing characteristics and their implication. Sci Gymnastics J. 2011;2:59-67.
17. Cuk II, Marinsek M. Landing quality in artistic gymnastics is related to landing symmetry. Biol Sport. 2013;30:29-33. 18. Carrara P, Mochigueki, L. Análise biomecânica do crucifi xo nas argolas. R. Bras Ci Mov. 2008;16:83-91.
19. Nordin M, Frankel VH. Biomecânica básica do sistema musculoesquelético. 3a ed. Rio de Janeiro: Guanabara Koogan; 2003. 20. Nakamoto JC, Saito M, Cunha AP, et al. Fratura do escafoide por estresse em ginasta: relato de caso. Rev Bras Ortop.
2009;44:533-5.
21. Godinho GG, Freitas JMA, Leite LMB, et al. Lesões slap no ombro. Rev Bras Ortop. 1998;33:345-52. 22. Silva RT. Lesões do membro superior no esporte. Rev Bras Ortop. 2010;45:122-31.
23. Prentice WE. Modalidades terapêuticas em medicina esportiva. São Paulo: Manole; 2002.
ENDEREÇO Natália Batista Albuquerque Goulart Colegiado de Educação Física Universidade Federal do Vale do São Francisco Av. José de Sá Maniçoba, s/n - Campus Universitário
56304-917 - Petrolina - PE - BRASIL e-mail: [email protected]