w w w . r b o . o r g . b r
Original
Article
Is
arthrodesis
still
a
good
indication
for
non-inflammatory
arthrosis
of
the
wrist?
夽
Bruno
de
Araujo
Silva
a,∗,
Marcos
Vinícius
Marciano
Campos
de
Souza
a,
Felipe
Moura
Carrasco
a,
Gustavo
Adolfo
Costa
Melo
a,
Luiz
Eduardo
Luz
Barreiros
a,
Pedro
José
Labronici
baHospitalEstadualdeTraumatologiaeOrtopediaDonaLindu,ParaíbadoSul,RJ,Brazil
bFaculdadedeMedicinadePetrópolis(FMP),Petrópolis,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30July2014
Accepted18September2014
Availableonline9September2015
Keywords: Arthrosis Wrist
Arthrodesisofthewrist
a
b
s
t
r
a
c
t
Objective:Theaimofthisstudywastoobjectivelyandsubjectivelyevaluatewristfunction
aftertotalarthrodesis,amongpatientswithsequelaeofnon-inflammatoryarthritiswho
weretreatedwithrigidinternalfixationusingaDCPplate.
Methods:Thirty-two patients with sequelaeof non-inflammatory degenerativearthritis
weretreatedusingtotalarthrodesisofthewrist.Ofthese,twopatientsweretreatedwith
Kirschnerwiresandfourdiscontinuedthetreatment,thusleaving26patients.The
indi-cationforarthrodesisofthewristwasthepresenceofintracarpalpathologicalconditions:
eightwristspresentedsequelaefromfracturesofthedistalradius;13hadsequelaefrom
fracturesofthescaphoid;andfivehadsequelaefromKienbock’sdisease.Thecaseswere
evaluatedusingthevisualanaloguescale(VAS),themusclestrengthtest,theJebsen–Taylor
functionaltestandtheBuck-Gramckotest.
Results:Itwasobservedthattherewerenosignificantdifferencesatthelevelof5%,inthe
variablesofgripstrength,VAS,Jebsen–TaylorfunctionaltestorBuck-Gramcko/Lohmann
test,betweenthepathologicalconditions.
Conclusion:Totalarthrodesisofthewristusingaplateinthedorsalregionwasshowntobe
asafeandefficienttechniqueforpatientswithdifferenttypesofpathologicalarthrosisof
thewrist,sinceitdidnotcauseanyimportantfunctionalincapacityandbroughtgreatpain
relief.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.Allrightsreserved.
夽
WorkperformedintheHospitalEstadualdeTraumatologiaeOrtopediaDonaLindu,ParaíbadoSul,RJ,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](B.deAraujoSilva).
http://dx.doi.org/10.1016/j.rboe.2015.08.017
Artrodese
ainda
é
uma
boa
indicac¸ão
na
artrose
não
inflamatória
do
punho?
Palavras-chave: Artrose Punho
Artrodesedopunho
r
e
s
u
m
o
Objetivo: Avaliarobjetivaesubjetivamenteafunc¸ãodopunho,apósartrodesetotal,em
pacientescomsequelasdeartritenãoinflamatóriatratadoscomfixac¸ãointernarígidacom
placatipoDCP.
Métodos:Foramtratados32pacientescomsequelasdeartritedegenerativanãoinflamatória
comartrodesetotaldopunho.Desses,doisforamtratadoscomfiosdeKirschnere
qua-trodescontinuaramotratamento.Restaram26.Asindicac¸õesparaaartrodesedopunho
forampacientescompatologiasintracarpais.Oitopunhosapresentavamsequeladefratura
radiodistal,13sequelasdefraturadoescafoideecincosequelasdedoenc¸adeKienbock.
Foramusadosparaaavaliac¸ãoaescalavisualanalógica(EVA),otestedeforc¸amuscular,o
testefuncionaldeJebsen-TayloreotestedeBuck-Gramcko.
Resultados: Observou-senãoexistirentreaspatologiasdiferenc¸asignificativa,nonívelde
5%,nasvariáveisdaforc¸adepreensão,EVA,testefuncionaldeJebsen-Taylorede
Buck-Gramcko/Lohmann.
Conclusão: Aartrodesetotaldepunho,complacanaregiãodorsal,demonstrouseruma
técnicaeficienteeseguraparaospacientescomdiferentestiposdepatologiasdeartrosede
punho,pornãocausarincapacidadefuncionalimportanteetrazerumgrandealíviodador.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier
EditoraLtda.Todososdireitosreservados.
Introduction
Total arthrodesisofthe wrist has becomea standard
pro-cedurefordegenerativewristarthritis.1,2Traditionally,wrist
arthrodesisisthetreatmentforwristarthritisthatdoesnot
respondtoanti-inflammatorymedications,immobilizersand
corticosteroidinjections,eventhoughitsubstantially
dimin-ishesthefunctioningofthisjoint.3
Arthritis in this joint has several causes, including the
following:sequelaeofintra-articularfractures,skewed
con-solidation subsequent to distal fracturing of the radius,
tearing of the interosseous ligaments, avascular necrosis,
inflammatorydiseasesandcongenitaldiseases.2Incasesof
non-inflammatorydiseases,wristarthrodesisprovidespain
reliefandincreasesthegripstrengthofthehand.
Many techniques have been used to perform wrist
arthrodesis, such as use of crossed Kirschner wires,
intramedullary pins, and plates and screws with or
with-out associateduse of bonegrafts.4,5 Rigidinternalfixation
withdifferenttypesofplatesnotonlyreducesthepainand
enablesthe returnto work,but alsomakesosteosynthesis
easyandsafe.Throughusingdorsalplates,consolidationrates
ofbetween93and100%havebeenachieved,withlow
compli-cationrates.1,2,6–9
Theaimofthepresentstudywastoevaluatelimb
func-tionaftertotalwristarthrodesisinpatientswithsequelaeof
non-inflammatoryarthritisthatwastreatedbymeansofrigid
internalfixationwithaDCPplateinthedorsalregionofthe
wrist.
Material
and
methods
BetweenOctober21,2010,andJanuary2014,32patientswith
sequelae of non-inflammatory degenerative arthritis were
treatedbymeansoftotalwristarthrodesis.Theprocedurewas
firstlyapprovedbythe hospital’sethicscommittee.Among
these, twoweretreated withKirschnerwiresandfour
dis-continued the treatment. Thus, 26 patients remained.The
inclusion factorswerethat thepatientswould have
seque-lae of intra-articular wrist fractures, skewed consolidation
subsequenttodistalfracturingoftheradiusandrestrictive
carpal pathologicalconditions(such asKienbock’sdisease).
The exclusion factors were the presence of inflammatory
degenerativediseasesandextracarpalpathologicalconditions
(suchasneuromusculardiseases,lesionsofperiarticularsoft
tissues,tumorresectionsandsequelaeofnerveinjuries).All
thepatientsweretreatedbymeansofrigidinternalfixation
withaDCPplateinthedorsalregionofthewrist.Sex,age,side
anddominancearepresentedinTable1.
Theindicationsforwristarthrodesiswerecasesofpatients
with intracarpal pathological condition. Eight wrists
pre-sented sequelaeofradiodistalfractures,13 hadsequelaeof
fracturesofthescaphoidandfivehadsequelaeofKienbock’s
disease.
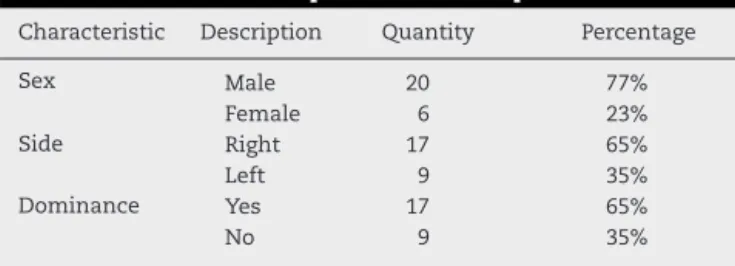
Table1–Generaldescriptionofthesample.
Characteristic Description Quantity Percentage
Sex Male 20 77%
Female 6 23%
Side Right 17 65%
Left 9 35%
Dominance Yes 17 65%
No 9 35%
Source:Filesofthehospitalservice.
Surgicaltechnique
Allthepatientswereoperatedundergeneralanesthesia,
com-plementedwithblockingofthebrachialplexusandpneumatic
ischemiaofthelimbaffected.Thelongitudinaldorsalaccess
routewasopened abovethethirdmetacarpal.The
retinac-ulum ofthe extensors was opened betweenthe third and
fourthtunnels.Thetendonofthelongextensorofthethumb
wasmovedawayradially,andtheextensoroftheindex
fin-ger and the common extensor ofthe fingers were moved
towardtheulna.Neurectomyoftheendbranchofthe
pos-teriorinterosseousnervewasperformedinaroutinemanner.
ThejointcapsulewasopenedastwoU-shapedflapswiththeir
basesattheradiusandulna.Thecartilageoftheradiocarpal
andintercarpaljointswasremovedasfarasthesubchondral
bone,andatLister’stubercle.Wed chosetoperform
curet-tageofthedorsalfaceofthecapitateandthedistalborderof
theradius.Weappliedtemporarydressingsandreleasedthe
pneumatictourniquet.Arectangularbonegraftwasremoved
fromtheipsilateralregion,alongwithspongybone.Weagain
appliedpneumaticischemiatothelimbandremovedthe
tem-porary dressing. Thespongy bonegraft was placedin the
radiocarpal and intercarpaljoints.TheDCP plate forsmall
fragmentswasmodeledwithameanangleof10◦inextension
andosteosynthesiswasperformedusingtheprinciplesofthe
AOtechnique,withsixcorticalgraftsinthethirdmetacarpal
andbetweensixandeightinthe radius,underradioscopic
control.Inthespacebetweenthecapitateandtheplate,we
placedaboneblockfromtheiliaccrest,underpressure.Thus,
nofixationscrewswereusedinthecarpus.Thejointcapsule
wasclosedwhenpossible.Inallthecases,weclosedthe
reti-naculumoftheextensorsandsuturedtheskinusingsimple
stitches.Wedidnotuseanydrainsoranyimmobilizationwith
splints,and onlyusedcompressivedressings.Thepatients
wereinstructedtoactivelymobilizetheirfingersduringthe
immediatepostoperativeperiod.Theywereassessedinthe
first,thirdandsixthweeksandthereaftereverytwomonths
untilthesixthpostoperativemonth.
Subjectiveevaluation
Thepatientswereaskedtomakeasubjectiveevaluationof
theirpostoperativepainusingavisualanaloguescale(VAS).10
TheVASisanefficientinstrumentformeasuringtheintensity
ofthepainandithasbeenusedinresearchandclinicaltrials.
Itconsistsofahorizontallinemeasuring10cm.Oneendis
labeled“nopain” andthe other,“worstpainpossible”. The
patientisaskedtomarkonthislinethepointcorrespondingto
thepainintensitylevelthatheisexperiencingatthatmoment.
Objectiveevaluation
Radiographsinanteroposteriorandlateral viewson allthe
patientswereanalyzedinordertodeterminethewrist
fix-ation position and the time taken for consolidation to be
achieved.
Thefunctionalevaluationincludedamusclestrengthtest
inwhichadynamometerwasusedtomeasurehandgrip;and
thefunctional testofJebsenet al.,11 whichiscomposedof
manipulativetaskssimilartothoseperformedinday-to-day
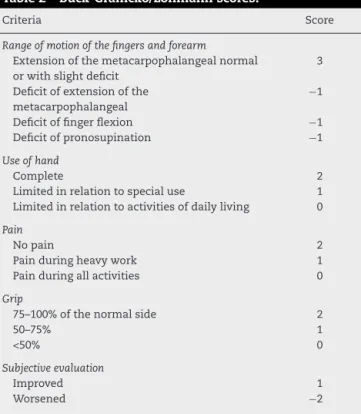
Table2–Buck-Gramcko/Lohmannscores.
Criteria Score
Rangeofmotionofthefingersandforearm
Extensionofthemetacarpophalangealnormal orwithslightdeficit
3
Deficitofextensionofthe metacarpophalangeal
−1
Deficitoffingerflexion −1 Deficitofpronosupination −1
Useofhand
Complete 2
Limitedinrelationtospecialuse 1 Limitedinrelationtoactivitiesofdailyliving 0
Pain
Nopain 2
Painduringheavywork 1 Painduringallactivities 0
Grip
75–100%ofthenormalside 2
50–75% 1
<50% 0
Subjectiveevaluation
Improved 1
Worsened −2
Excellent,9–10;Good,7–8;Satisfactory,5–6;Poor,<5.
activities andisdivided into sevensubtests: (1)writing;(2) simulationofthetaskofturningcardsover;(3)liftingupsmall objects;(4)simulationofusingaspoonforeating;(5)pilingup blocks(i.e.usingpiecesfromthegameofdraughts/checkers); (6)liftinguplargelightobjects;and(7)liftinguplargeheavy objects.Thepercentagescoreisobtainedfrom case-control standardizedvaluesproducedbythisauthor.Inaddition,the Buck-Gramckotest,12 whichisspecific forarthrodesis,was
usedasanobjectiveassessmentforarthrodesis,asshownin
Table2.
Statisticalmethodology
Thedescriptiveanalysispresentedtheobserveddatainthe
formoftables.Thedatawereexpressedasmeans,standard
deviations,medians,minimumsandmaximumsfor
numer-ical data and as frequencies (n) and percentages (%) for
categoricaldata(qualitative).
The comparative analysis on the variables of grip
strength, VAS, Jebsen–Taylor functional test and
Buck-Gramcko/Lohmann test between the three pathological
conditions (sequelae of scaphoid fractures, sequelae of
radiodistal fractures and Kienbock’s disease) was defined
usingtheKruskal–WallisANOVAtest(fornumericalvariables)
andFisher’sexacttest(forcategoricalvariables).
Non-parametrictestswereusedbecausethevariablesdid
not present normal (Gaussian) distribution, giventhat the
hypothesisofnormalityaccordingtotheShapiro–Wilkstest
was rejected. The criterion used to determinesignificance
was thelevel of5%.Thestatistical analysiswasprocessed
using the SAS 6.11 software (SAS Institute, Inc., Cary, NC,
Table3–Descriptionofthevariablesinthewholesample.
Variable n Mean SD Median Minimum Maximum
Gripstrength–wristwitharthrodesis(kg) 26 17.6 11.2 14.7 1.7 42.8 Gripstrength–wristwithoutarthrodesis(kg) 26 31.3 10.0 32.8 10.2 46.9 Deltaforgripstrength(kg) 26 −13.7 12.5 −13.8 −39.8 7.4 Relativedeltaforgripstrength(%) 26 −41.7 36.8 −47.7 −90.7 32.7
VAS–before(points) 26 8.9 1.4 10 4 10
VAS–after(points) 26 3.2 2.9 3 0 10
DeltaforVAS(points) 26 −5.7 3.0 −5.5 −10.0 1.0 RelativedeltaforVAS(%) 26 −64.2 31.3 −63.3 −100.0 11.1 Totaltime–wristwitharthrodesis(s) 26 115.0 76.8 86.9 56.6 351.4 Totaltime–wristwithoutarthrodesis(s) 26 90.6 23.1 89.3 48.5 139.8 Deltafortotaltime(s) 26 24.4 67.5 3.4 −27.2 247.7 Relativedeltafortotaltime(%) 26 24.3 63.0 4.2 −25.4 238.8
Buck-Gramcko/Lohmann(points) 26 5.3 3.2 5.5 0 10
Source:Filesofthehospitalservice. SD,standarddeviation.
Results
Themeantimetakeforconsolidationtobeachievedforthe entiresamplewas10.8 weeks.Forthe casesofsequelaeof scaphoid fractures,the mean time was 10.4 weeks(range: 6–20).Forthecasesofsequelaeofradiodistalfractures,the meantimewas9.4weeks(range:5–24).Forthecasesof seque-lae of Kienbock’s disease, the mean time was 11.6 weeks (range:8–18).Itisimportanttoemphasizethatnocasesof pseudarthrosisoccurred.Thetotallengthoffollow-upforthe samplewas18.5months.
Characterizationofthestudysample
Thisstudyhadtheaimofoutliningtheprofileof26patients subsequenttowristarthrodesis.
The absolute delta is the difference in measurements between the wrist with arthrodesisand the wrist without arthrodesis. In this study, a negative delta expresses the number of kg/point/second less than in the wrist without arthrodesis.
The relative delta is the percentage difference between the two wrists in relation to the wrist without arthrode-sis. In this study, a negative relative delta expresses the percentage kg/point/second less than in the wrist without arthrodesis.
Tables 3–6 present the mean, standard deviation (SD),
median, minimum and maximum of the variables in the
whole sampleand inthedifferent pathological conditions:
sequelaeofscaphoidfractures,sequelaeofradiodistal
frac-turesandKienbock’sdisease,respectively.
Table7presentsthefrequencies(n)and percentages(%)
ofthecategoricalvariables inthewholesampleandinthe
differentpathologicalconditions.
The next objective was to ascertain whether there was
anysignificantdifferenceinthevariables(gripstrength,VAS
score,Jebsen–TaylorfunctionaltestandBuck-Gramckotest),
betweenthepathologicalconditions.
Table 8 presents the mean, standard deviation (SD)
and median of the variables of grip strength, VAS score,
Jebsen–TaylorfunctionaltestandBuck-Gramckotest,
accord-ing to the pathological condition (sequelae of scaphoid
fractures, sequelae of radiodistal fractures and Kienbock’s
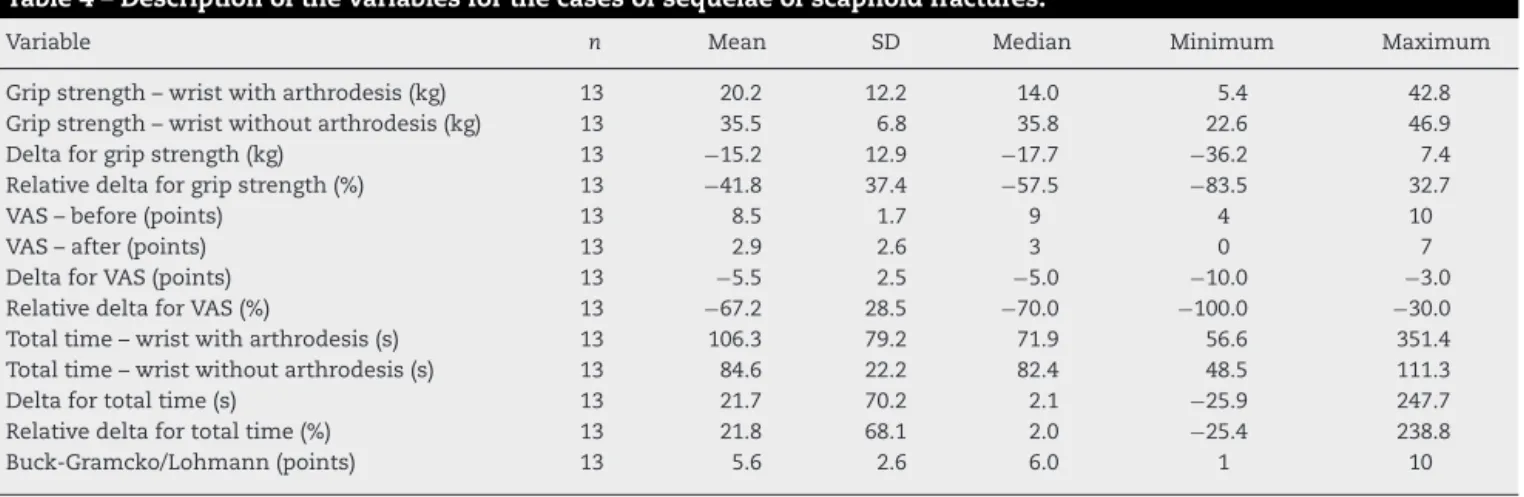
Table4–Descriptionofthevariablesforthecasesofsequelaeofscaphoidfractures.
Variable n Mean SD Median Minimum Maximum
Gripstrength–wristwitharthrodesis(kg) 13 20.2 12.2 14.0 5.4 42.8 Gripstrength–wristwithoutarthrodesis(kg) 13 35.5 6.8 35.8 22.6 46.9 Deltaforgripstrength(kg) 13 −15.2 12.9 −17.7 −36.2 7.4 Relativedeltaforgripstrength(%) 13 −41.8 37.4 −57.5 −83.5 32.7
VAS–before(points) 13 8.5 1.7 9 4 10
VAS–after(points) 13 2.9 2.6 3 0 7
DeltaforVAS(points) 13 −5.5 2.5 −5.0 −10.0 −3.0 RelativedeltaforVAS(%) 13 −67.2 28.5 −70.0 −100.0 −30.0 Totaltime–wristwitharthrodesis(s) 13 106.3 79.2 71.9 56.6 351.4 Totaltime–wristwithoutarthrodesis(s) 13 84.6 22.2 82.4 48.5 111.3 Deltafortotaltime(s) 13 21.7 70.2 2.1 −25.9 247.7 Relativedeltafortotaltime(%) 13 21.8 68.1 2.0 −25.4 238.8
Buck-Gramcko/Lohmann(points) 13 5.6 2.6 6.0 1 10
Table5–Descriptionofthevariablesforthecasesofsequelaeofradiodistalfractures.
Variable n Mean SD Median Minimum Maximum
Gripstrength–wristwitharthrodesis(kg) 8 15.2 10.2 15.7 3.9 30.0 Gripstrength–wristwithoutarthrodesis(kg) 8 30.8 9.9 27.3 19.3 44.0 Deltaforgripstrength(kg) 8 −15.7 14.2 −15.7 −39.8 3.4 Relativedeltaforgripstrength(%) 8 −47.3 38.8 −53.8 −90.7 15.4
VAS–before(points) 8 9.1 1.2 10 7 10
VAS–after(points) 8 3.1 2.6 4 0 8
DeltaforVAS(points) 8 −6.0 3.0 −5.0 −10.0 −2.0 RelativedeltaforVAS(%) 8 −64.6 27.3 −58.6 −100.0 −20.0 Totaltime–wristwitharthrodesis(s) 8 102.5 30.0 97.9 61.0 147.0 Totaltime–wristwithoutarthrodesis(s) 8 93.6 15.6 95.4 72.3 118.7
Deltafortotaltime(s) 8 8.9 31.8 0.7 −17.6 74.7
Relativedeltafortotaltime(%) 8 12.0 41.0 0.9 −18.3 103.2
Buck-Gramcko/Lohmann(points) 8 5.4 3.7 5.0 0 10
Source:Filesofthehospitalservice. SD,standarddeviation.
Table6–DescriptionofthevariablesforthecasesofsequelaeofKienbock’sdisease.
Variable n Mean SD Median Minimum Maximum
Gripstrength–wristwitharthrodesis(kg) 5 14.7 10.3 11.8 1.7 26.5 Gripstrength–wristwithoutarthrodesis(kg) 5 21.3 11.6 21.6 10.2 39.0 Deltaforgripstrength(kg) 5 −6.6 7.0 −10.1 −12.5 2.2 Relativedeltaforgripstrength(%) 5 −32.5 38.1 −32.1 −85.6 10.2
VAS–before(points) 5 9.8 0.4 10 9 10
VAS–after(points) 5 4.2 4.4 4 0 10
DeltaforVAS(points) 5 −5.6 4.7 −6.0 −10.0 1.0
RelativedeltaforVAS(%) 5 −55.8 47.6 −60.0 −100.0 11.1 Totaltime–wristwitharthrodesis(s) 5 157.7 116.8 112.5 65.8 350.7 Totaltime–wristwithoutarthrodesis(s) 5 101.5 33.6 81.8 73.9 139.8 Deltafortotaltime(s) 5 56.3 100.9 4.7 −27.2 214.1 Relativedeltafortotaltime(%) 5 50.5 82.4 6.3 −19.5 156.8
Buck-Gramcko/Lohmann(points) 5 4.6 4.2 3.0 0 10
Source:Filesofthehospitalservice. SD,standarddeviation.
disease)andthecorrespondingdescriptivelevel(pvalue)from theKruskal–WallisANOVAtest(nonparametric).
It was observed that there were no significant differ-ences betweenthe pathological conditionsatthe 5%level,
with regard to the variables of grip strength, VAS score, Jebsen–TaylorfunctionaltestandBuck-Gramckotest.
Table9presentsthe frequencies(n)and percentages(%)
relating to the side with arthrodesis, dominant side and
Table7–Descriptionofthevariablesinthewholesampleandinthedifferentpathologicalconditions.
Variable Total(n=26) Scaphoid(n=13) Radiodistal(n=8) Kienbock(n=5)
n % n % n % n %
Sidewitharthrodesis
Right 17 65.4 9 69.2 6 75 2 40
Left 9 34.6 4 30.8 2 25 3 60
Dominantside
Right 17 65.4 9 69.2 6 75 2 40
Left 9 34.6 4 30.8 2 25 3 60
Result
Excellent 5 19.2 2 15.4 2 25 1 20
Good 4 15.4 2 15.4 1 12.5 1 20
Satisfactory 5 19.2 4 30.8 1 12.5 0 0
Poor 12 46.2 5 38.5 4 50 3 60
T able 8 – Compar a ti v e anal ysis betw een the differ ent pa thological conditions. V aria b le Sequelae of scaphoid fr actur es Sequelae radiodistal fr actur es Kienboc k’ s disease p v alue a Mean ± SD Med Mean ± SD Med Mean ± SD Med Grip str ength – wrist with arthr odesis (kg) 20.2 ± 12.2 14.0 15.2 ± 10.2 15.7 14.7 ± 10.3 11.8 0.49 Grip str ength – wrist without arthr odesis (kg) 35.5 ± 6.8 35.8 30.8 ± 9.9 27.3 21.3 ± 11.6 21.6 0.060 Delta for grip str ength (kg) − 15.2 ± 12.9 − 17.7 − 15.7 ± 14.2 − 15.7 − 6.6 ± 7.0 − 10.1 0.28 Relati v e delta for grip str ength (%) − 41.8 ± 37.4 − 57.5 − 47.3 ± 38.8 − 53.8 − 32.5 ± 38.1 − 32.1 0.71 VA S – befor e (points) 8.5 ± 1.7 9 9.1 ± 1.2 10 9.8 ± 0.4 10 0.14 VA S – after (points) 2.9 ± 2.6 3 3.1 ± 2.6 4 4.2 ± 4.4 4 0.88 Delta for VA S (points) − 5.5 ± 2.5 − 5.0 − 6.0 ± 3.0 − 5.0 − 5.6 ± 4.7 − 6.0 0.91 Relati v e delta for VA S (%) − 67.2 ± 28.5 − 70.0 − 64.6 ± 27.3 − 58.6 − 55.8 ± 47.6 − 60.0 0.91 T otal time – wrist with arthr odesis (s) 106.3 ± 79.2 71.9 102.5 ± 30.0 97.9 157.7 ± 116.8 112.5 0.40 T otal time – wrist without arthr odesis (s) 84.6 ± 22.2 82.4 93.6 ± 15.6 95.4 101.5 ± 33.6 81.8 0.59 Delta for total time (s) 21.7 ± 70.2 2.1 8.9 ± 31.8 0.66 56.3 ± 100.9 4.7 0.91 Relati v e delta for total time (%) 21.8 ± 68.1 2.0 12.0 ± 41.0 0.9 50.5 ± 82.4 6.3 0.85 Buc k-Gr amc ko/Lohmann (points) 5.6 ± 2.6 6 5.4 ± 3.7 5 4.6 ± 4.2 3 0.79 Sour ce : F iles of the hospital service . SD , standar d de viation. a Kruskal–W allis ANO V A.
Buck-Gramckoclassification,accordingtothedifferent
patho-logicalconditions(sequelaeofscaphoidfractures,sequelaeof
radiodistalfracturesand Kienbock’sdisease)and the
corre-spondingdescriptivelevel(pvalue)fromFisher’sexacttest.
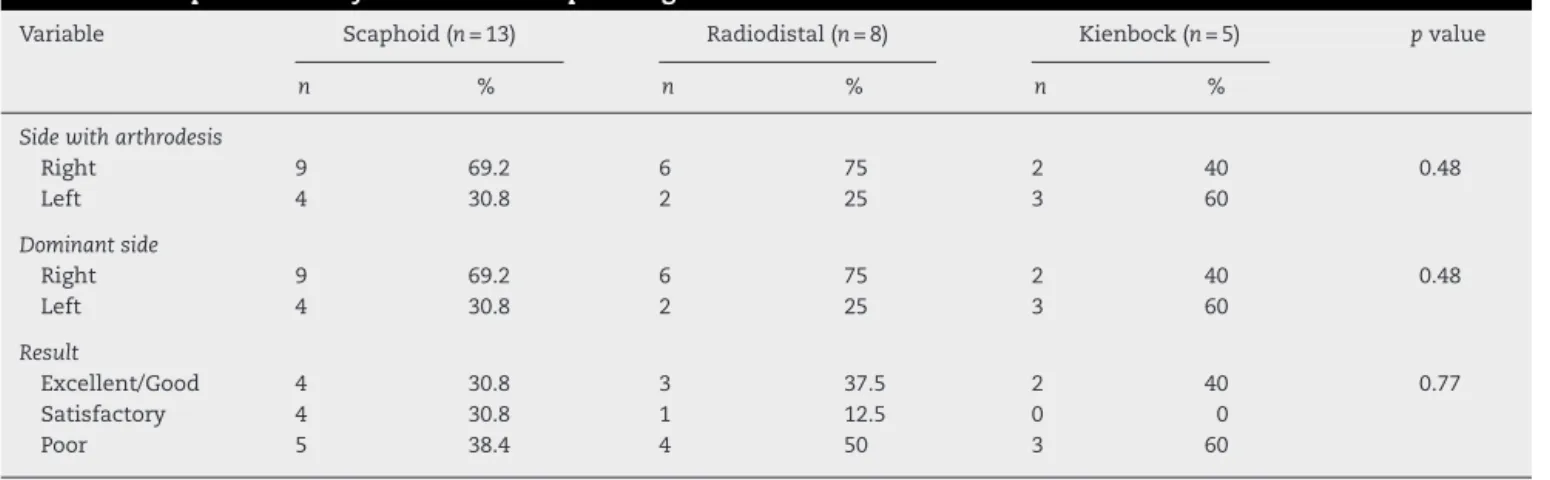
Itwasobservedthattherewerenosignificantdifferences
between the pathological conditions at the 5% level, with
regardtothesidewitharthrodesis,dominantsideand
Buck-Gramckoclassification.
Discussion
When orthopedic surgeons are faced with patients
pre-sentingnon-inflammatorywristarthritiswhoarecandidates
for surgery, wrist arthrodesis should be avoided
when-everpossible.Nevertheless,thisreconstructionprocedureis
well establishedand has been proven tohave great value
for many pathological conditions. Historically, it has
pre-sentedsatisfactorypostoperativeresults,sincetheincapacity
thatarthrodesisproducescanbecompensatedfor,provided
that the patient’s shoulder, elbow, forearm and hand are
normal.13–15 Although severaltechniques fortreating wrist
arthrosis exist, the introduction of dynamic compression
platesbytheAOgroup,16usedinassociationwithbonegrafts,
hasledtohighratesofgoodresultsfromarthrodesis,which
hasmadeitthemostpopularmethod.16,17
According tothe literature,the consolidation rates
sub-sequent to the procedure have been 98–100%, with good
resultsregardingpainreliefandimprovementgripstrength,
andsatisfactionratesofbetween80and100%.Thepatients
report that they would like to haveundergone this
proce-dure before other techniques. Arthrodesis has little or no
repercussion in relation to loss ofmobility and long-term
complications.1,18,19
In the present study, in comparing the sides with and
withoutarthrodesis,thegripstrengthofthehandwaslower
on the side with arthrodesis in all the groups evaluated:
57.5% in the cases of sequelae from scaphoid fractures;
53.8% in the cases of sequelae from radiodistal fractures;
and 32.1% inthe casesofKienbock’s disease,without
pre-senting any significant difference. This demonstrated that
diminutionofmusclestrengthoccurredbothinpathological
conditionsofsequelaeofintra-articularfracturesofthewrist
and insituations ofskewedconsolidation afterdistal
frac-turingoftheradiusandunderrestrictivecarpalpathological
conditions.
Inanalyzing thestateofpain usingthe VAS,thewrists
withandwithoutarthrodesiswerecompared.Completepain
reliefafterwristarthrodesisshouldbeexpectedinthe
major-ityofpatients.20Inthepresentstudy,thepatientsreported
improvementsinpainlevelsinallthegroupsevaluated:70%
improvementoradecreaseoffivepointsontheVASscalein
thecasesofsequelaefromscaphoidfractures;58.6%orfive
pointsinthecasesofsequelaefromradiodistalfractures;and
60%orsixpointsinthecasesofKienbock’sdisease,without
presentinganysignificantdifference.Itwasobservedthatover
thesepatients’follow-upperiod,mostofthemdidnotreport
anypainorneedanyregularanalgesia.
TheJebsen–Taylorfunctionaltest, whichiscomposedof
Table9–Comparativeanalysisbetweenthepathologicalconditions.
Variable Scaphoid(n=13) Radiodistal(n=8) Kienbock(n=5) pvalue
n % n % n %
Sidewitharthrodesis
Right 9 69.2 6 75 2 40 0.48
Left 4 30.8 2 25 3 60
Dominantside
Right 9 69.2 6 75 2 40 0.48
Left 4 30.8 2 25 3 60
Result
Excellent/Good 4 30.8 3 37.5 2 40 0.77
Satisfactory 4 30.8 1 12.5 0 0
Poor 5 38.4 4 50 3 60
Source:Filesofthehospitalservice.
not demonstrate any significant incapacity from arthrode-sis,in comparingthe wrists withand without arthrodesis. In observing the results, the taskswere carried out more slowly on the sidewith arthrodesis,by differences of2.1s amongthe patientswithsequelaefrom scaphoidfractures, 0.9s amongthose withsequelae from radiodistalfractures and6.3samongthosewithKienbock’sdisease,incomparison withthesidewithoutarthrodesis.Theseresultsmaysuggest thatpatientswithsequelaefromKienbock’sdiseasepresenta greatertendencytowardfunctionalincapacity.However,our limitednumberofcasesdoesnotallowustoreachthis con-clusion.
In this study, the Buck-Gramcko test, which is specific forarthrodesis and consistsof anobjective assessment of arthrodesis,demonstratedthatthepatientspresentedresults rangingfromgoodtosatisfactory.Themeanscoresweresix pointsforsequelaeofscaphoidfractures,fiveforsequelaeof radiodistalfracturesandthreeforKienbock’sdisease.
Thestrong pointofthis study was that it analyzedthe resultsfromthreedifferentpathologicalconditionsofwrist arthrosisafterthearthrodesisprocedure.Throughthis,the indications for using this type of procedure can be con-sidered. Theweakpointwas the unsatisfactorynumber of patients,giventhatwristarthrodesisisanuncommon pro-cedure,which prevented usfrom reaching aconclusion of greaterprecision.Anotherpointwasthelackofcomparison ofpainamongthepatientsbeforeandaftertheprocedure.
Themostfrequentcomplications were tendinitisofthe extensors,ineightpatients,andtheneedtoremovetheplate insix.Othercomplicationsincludedonecaseofcontracture oftheextensors, onecaseofsuperficialinfection thatwas resolvedthroughantibiotictherapyandonecaseofloosening ofthesynthesismaterial.
Conclusion
Totalarthrodesisofthewristusingaplateinthedorsalregion wasshowntobeasafeandefficienttechniqueforpatients withdifferentpathologicalconditionsofwristarthrosis,since itdidnotcauseanysignificantfunctionalincapacityandgave risetogreatpainrelief.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.HastingsH2nd,WeissAP,QuenzerD,WiedemanGP, HaningtonKR,StricklandJW.Arthrodesisofthewristfor post-traumaticdisorders.JBoneJointSurgAm.
1996;78(6):897–902.
2.WeissAP,HastingsH2nd.Wristarthrodesisfortraumatic conditions:astudyofplateandlocalbonegraftapplication.J HandSurgAm.1995;20(1):50–6.
3.FieldJ,HerbertTJ,ProsserR.Totalwristfusion.Afunctional assessment.JHandSurgBr.1996;21(4):429–33.
4.AbbotLC,SaundersJB,BostFC.Arthrodesisofthewristwith theuseofgraftsofcancellousbone.JBoneJointSurg. 1942;24:883–98.
5.CampbellCJ,KeokarnT.Totalandsubtotalarthrodesisofthe wrist.JBoneJointSurgAm.1964;46:1520–33.
6.MeadsBM,ScougallPJ,HargreavesIC.Wristarthrodesisusing aSyntheswristfusionplate.JHandSurgBr.2003;28(6):571–4.
7.O’BierneJ,BoyerMI,AxelrodTS.Wristarthrodesisusinga dynamiccompressionplate.JBoneJointSurgBr.
1995;77(5):700–4.
8.SagermanSD,PalmerAK.Wristarthrodesisusingadynamic compressionplate.JHandSurgBr.1996;21(4):437–41.
9.WeissAP.Principlesoflimitedwristarthrodesis.In:Berger RA,WeissAPC,editors.Handsurgery.Philadelphia: Lippincott,Williams&Wilkins;2004.p.1292.
10.HuskissonEC.Visualanaloguescale.In:MelzackR,editor. Painmeasurementandassessment.NewYork:ReavenPress; 1983.p.33–7.
11.JebsenRH,TaylorN,TrieschmannRB,TrotterMJ,HowardLA. Anobjectiveandstandardizedtestofhandfunction.Arch PhysMedRehabil.1969;50(6):311–9.
12.Buck-GramckoD,LohmannH.Compressionarthrodesisof thewrist.In:TubianaR,editor.Thehand.Philadelphia: Saunders;1981.p.723.
13.HaydenRJ,JebsonPJ.Wristarthrodesis.HandClin. 2005;21(4):631–40.
15.BarbieriCH,MazzerN,EluiVMC,FonsecaMCR.Resultados funcionaisdaartrodesedopunho.ActaOrtopBras. 2002;10(1):17–24.
16.MüllerME,AllgöwerM,SchneiderR,WilleneggerH.Manual ofinternalfixation:techniquesrecommendedby
theAOgroup.2nded.Berlin:Springer-Verlag; 1979.
17.LarssonSE.Compressionarthrodesisofthewrist.A consecutiveseriesof23cases.ClinOrthopRelatRes. 1974;(99):146–53.
18.NagyL,BüchlerU.AO-wristarthrodesis:withandwithout arthrodesisofthethirdcarpometacarpaljoint.JHandSurg Am.2002;27(6):940–7.
19.LeNenD,RichouJ,SimonE,LeBourgM,NabilN,DeBodman C,etal.Thearthriticwrist.I.Thedegenerativewrist:surgical treatmentapproaches.OrthopTraumatolSurgRes.2011;974 Suppl:S31–6.