RevPaulPediatr.2016;34(4):503---509
REVISTA
PAULISTA
DE
PEDIATRIA
www.rpped.com.br
REVIEW
ARTICLE
Association
of
growth
and
nutritional
parameters
with
pulmonary
function
in
cystic
fibrosis:
a
literature
review
Renan
Marrichi
Mauch
∗,
Arthur
Henrique
Pezzo
Kmit,
Fernando
Augusto
de
Lima
Marson,
Carlos
Emilio
Levy,
Antonio
de
Azevedo
Barros-Filho,
José
Dirceu
Ribeiro
FaculdadedeCiênciasMédicas,UniversidadeEstadualdeCampinas(Unicamp),Campinas,SãoPaulo,Brazil
Received13August2015;accepted2December2015 Availableonline9February2016
KEYWORDS
Cysticfibrosis; Lung/pathophysiology; Growth;
Nutrition
Abstract
Objective: Toreviewtheliteratureaddressingtherelationshipofgrowthandnutritional
param-eterswithpulmonaryfunctioninpediatricpatientswithcysticfibrosis.
Datasource:Acollectionofarticlespublishedinthelast15yearsinEnglish,Portugueseand
Spanish wasmade byresearchinelectronicdatabases ---PubMed,Cochrane,Medline,Lilacs
andScielo---usingthekeywordscysticfibrosis,growth,nutrition,pulmonaryfunctionin
var-iedcombinations.Articlesthataddressedthelongtermassociationofgrowthandnutritional
parameters, with an emphasis on growth, with pulmonary disease in cystic fibrosis, were
included, and we excluded thosethataddressing onlythe relationship between nutritional
parametersandcysticfibrosisandthoseinwhichtheaimwastodescribethedisease.
Datasynthesis: Seven studies were included, with a total of 12,455 patients. Six studies
reported relationship between growth parameters and lung function, including one study
addressingtheassociationofgrowthparameters,solely,withlungfunction,andalltheseven
studiesreportedrelationshipbetweennutritionalparametersandlungfunction.
Conclusions: Thereviewsuggeststhattheseverityofthelungdisease,determinedby
spirome-try,isassociatedwithbodygrowthandnutritionalstatusincysticfibrosis.Thus,theintervention
intheseparameters canlead tothebetterprognosisandlife expectancyforcysticfibrosis
patients.
©2016SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen
accessarticleundertheCCBYlicense(http://creativecommons.org/licenses/by/4.0/).
∗Correspondingauthor.
E-mail:[email protected](R.M.Mauch).
http://dx.doi.org/10.1016/j.rppede.2016.02.001
2359-3482/©2016SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY
504 MauchRMetal.
PALAVRAS-CHAVE
Fibrosecística; Pulmão/fisiopatologia; Crescimento;
Nutric¸ão
Associac¸ãodosparâmetrosdecrescimentoenutricionaiscomfunc¸ãopulmonar nafibrosecística:revisãodaliteratura
Resumo
Objetivo: Revisar a literaturaque aborda arelac¸ão entre osparâmetros de crescimento e
nutricionaiscomafunc¸ãopulmonarempacientespediátricoscomfibrosecística.
Fontesdedados: Dadosforamcoletadosdeartigospublicadosnosúltimos15anosemInglês,
PortuguêseEspanholatravésdepesquisanasbasesdedadoseletrônicas---PubMed,Cochrane,
Medline, Lilacse Scielo---usando aspalavras-chave:fibrose cística, crescimento, nutric¸ão,
func¸ãopulmonarutilizandocombinac¸õesvariadas.Osartigosqueanalisaramaassociac¸ãode
longoprazoentreparâmetrosdecrescimentoenutricionais,comênfaseemcrescimento,com
doenc¸apulmonaremfibrosecística,foramincluídos,sendoexcluídosaquelesqueanalisaram
apenasarelac¸ãoentreosparâmetrosnutricionaisefibrosecísticaeaquelesemqueoobjetivo
eradescreveradoenc¸a.
Síntesedosdados: Seteestudosforamincluídos,comumtotalde12.455pacientes.Seis
estu-dosrelataramrelac¸ãoentreparâmetrosdecrescimentoefunc¸ãopulmonar,incluindoumestudo
queanalisouapenasaassociac¸ãodeparâmetrosdecrescimentocomafunc¸ãopulmonar,etodos
osseteestudosrelataramassociac¸ãoentreparâmetrosnutricionaisefunc¸ãopulmonar.
Conclusões: Arevisãosugerequeagravidadedadoenc¸apulmonar,determinadapor
espirome-tria,estáassociadacomcrescimentocorporaleoestadonutricionalemfibrosecística.Assim,
aintervenc¸ãonessesparâmetrospodecontribuirparaummelhorprognósticoeexpectativade
vidaempacientescomfibrosecística.
©2016SociedadedePediatriadeS˜aoPaulo.PublicadoporElsevierEditoraLtda.Este ´eum
artigoOpenAccesssobumalicenc¸aCCBY(http://creativecommons.org/licenses/by/4.0/).
Introduction
CysticFibrosis(CF)isthemostcommonlethalgenetic dis-easein Caucasian populations.Itis caused by a mutation inagenethatencodestheCysticFibrosisTransmembrane conductanceRegulator(CFTR)protein,whichisexpressed in many epithelial and blood cells, functioning mainly as achloridechannel.1Pulmonarydiseaseisthemost impor-tant manifestation in CF and the main factor acting in morbidity and mortality of the disease. The response in pulmonary diseaseis mediatedby abnormalCFTR,2 modi-fiergenes,3---8airwayinfectionsandinflammation,9probably affectingweightandheightduetoappetitesuppressionand enhancedenergyexpenditure.
Malnutritionandgrowthrestrictionarealsofrequentand arerelatedtotheimpairmentofthepulmonaryfunctionin aviciouscircle:malnourishedpatientstendtopresentworst pulmonaryfunctionandpatientswithseverepulmonary dis-easetendtogrowupless.Althoughtheserelationshipshave beenalreadyreported,10,11thereareafewlongterm anal-ysesin regardtotheachievement ofgrowthandnutrition goalsforthecourseofpulmonaryfunctionfrominfancyto adulthood.
Inthiscontext,theaimofthisstudywastoanalyzelong term studies comparing growth and nutrition parameters (with emphasis in growth) with pulmonary function in CF patients,evaluatingtherelationshipamongthesefactors.
Method
Aliteraturereviewof thelast15years(2000---2015)about the relationship between growth and nutritional parame-tersandlungfunctionwasmade.Thesearchforreferences inEnglish,SpanishandPortuguese wasperformed through
electronicdatabases--- PubMed,Medline,Cochrane,Lilacs andScielo---usingthedescriptors:CF,growth,bodygrowth, pulmonary function and lung function in varied combina-tionsandintheircorrespondenttranslationstoPortuguese andSpanish.Reviewsaddressingthethemewerealso con-sulted,aswellreferencelistsofallarticles,tosearchfor newstudies.
After this stage, we started the screening of papers, by analyzingtitles andabstracts.The firstinclusion crite-rionwastheidentification ofpotentially relevant studies, considering those in which the report compared growth parameters withlung function. In this case, we excluded studiesin whichtheaimsweretocompare weightand/or heightgain,withoutrelationship withpulmonaryfunction, andthoseinwhichtheaimsweretodescribeCFonly.
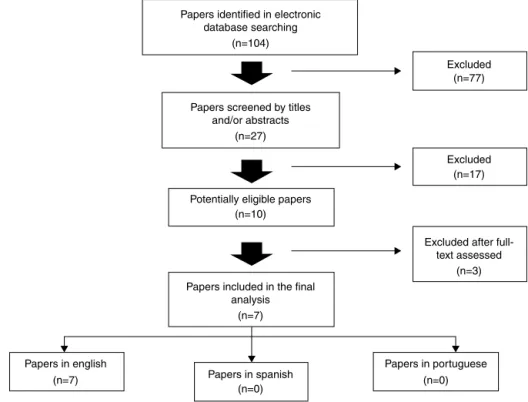
Inthe first search, atotal of 104 articles werefound. Byevaluatingtitlesandabstracts,thefollowing recupera-tioncriteriaforcomplete articleswere:studiesofcohort, longitudinal, cross-sectional, descriptive and prospective, whichresultsevaluatedtherelationshipamongpulmonary function andgrowthparameters inCF patients,excluding thosewhich,despiteofappearinginthesearchresults,did not address the subject under this point of view. In this stage,27paperswerescreened.Thereviewwasconcluded withthereadingofthecompletearticles,and,inthefinal manuscript,sevenarticleswereincluded,12---18allofthemin English(Fig.1;Tables1and2).
Data
synthesis
Associationofgrowthandnutritionalparameterswithpulmonaryfunctionincysticfibrosis 505
Papers identified in electronic database searching
(n=104)
Papers screened by titles and/or abstracts
(n=27)
Papers included in the final analysis
Papers in english
Papers in spanish Papers in portuguese Excluded after
full-text assessed Excluded Excluded
(n=7)
(n=0) (n=0)
(n=3) (n=17) (n=77)
(n=7)
Potentially eligible papers (n=10)
Figure1 Methodofresearch,screening,exclusionandinclusionofpapersinthefinalanalysis.NopapersinSpanishandPortuguese
werefound.
wasacohort study,12 fourwere longitudinal studies13---15,17 andtwowereprospectivestudies.16,18
Theselectedstudiesusedseveralgrowthandnutritional parameters.Amongthenutritionalandgrowthparameters, BodyMassIndex(BMI)wasevaluatedinfivestudies,12,14---16,18 heightalonewasevaluatedintwostudies,13,15 heightgain wasevaluatedintwostudies,13,15WeightForAge(WFA)was evaluatedintwostudies,14,18HeightForAge(HFA)was eval-uatedin twostudies.14,16 The remainingparameters were evaluatedeach onein onestudy:weightalone,14 percent of height-appropriateBody Weight (%haBW),12 percentage ofthe IdealBodyWeight (%IBW),12 Heightfor AgeZ-score (HAZ),12 Weight for Age Z-score (WAZ),12 Height-For-Age adjusted for Target Height (HFA/TH),17 Weight-For-Length andBMIpercentiles(WFL-BMI)18(Tables1and2).
All studies used Forced Expiratory Volume in 1 second (FEV1orFEV1%predicted)asameasureforpulmonary func-tionandonlyoneusedforcedvitalcapacity.14
Sixstudiesassessedtherelationshipofgrowthand nutri-tionalparameterswithpulmonaryfunction12---14,16---18andonly one study assessed the relationship of growth alone with pulmonaryfunction.15
Main
results
Zemel etal.12 studied a large sample (968children) from multiple care centersacross the United Statesduring a 4 yearperiod.Duringthefirst3yearsoffollow-up,thefemale patientsdeclinedinHAZ,whereasmalepatientsincreased HAZ. Bothgroups declined in this same parameter in the lastyear.Thereweredifferencesinthepatternof longitu-dinalchangeinFEV1%,andtherateofdeclinewaslessin malepatients. Theauthors found thatHAZ waspositively
andsignificantlyassociatedwithFEV1%, aswereWAZand %haBW.
Konstanetal.13 examined,in931patients,therelative roleof growthand nutritional statusand theclinical evi-dence of lung disease fromage 3---6 years in determining pulmonaryfunction at 6yearsof age.The resultsshowed thatmean WFAand HFA at both ages3 and6 yearswere belowthe 50thpercentilefor healthy children. The pres-enceof signsand symptomsof lung disease at age 3 was only weakly associated with growth and nutritional cate-goriesinthissameage.However,patientswithlowergrowth andnutritionalindexesatage3hadlowerpulmonary func-tionatage6,andthiswasevidentforWFAandHFA,inwhich thedifferencesinthepercentpredictedlungfunction val-uesreached15and12pointsforthelowestandhighWFA andHFAcategories,respectively.
Petersonetal.14prospectivelyexamineddataof319 chil-drenfromages6---8years.Totalweightchange(kg/month) betweenthechild’sfirstandlastvisitswasexamined asa markerofcumulative growthduringthe 2year period.In repeatedmeasuresregressionanalysis,FEV1valuesdidnot varysignificantlybyheightchangewithinpatientswithhigh orlowweightchange.Neithertheheightnorchangeinthe heightfromfirst observationwere significantlyassociated withFEV1values,butchildrenwhohadasteadyweightgain tendedtoexperiencegreaterincreasesinFEV1thanthose wholoseweight.
506
Mauch
RM
et
al.
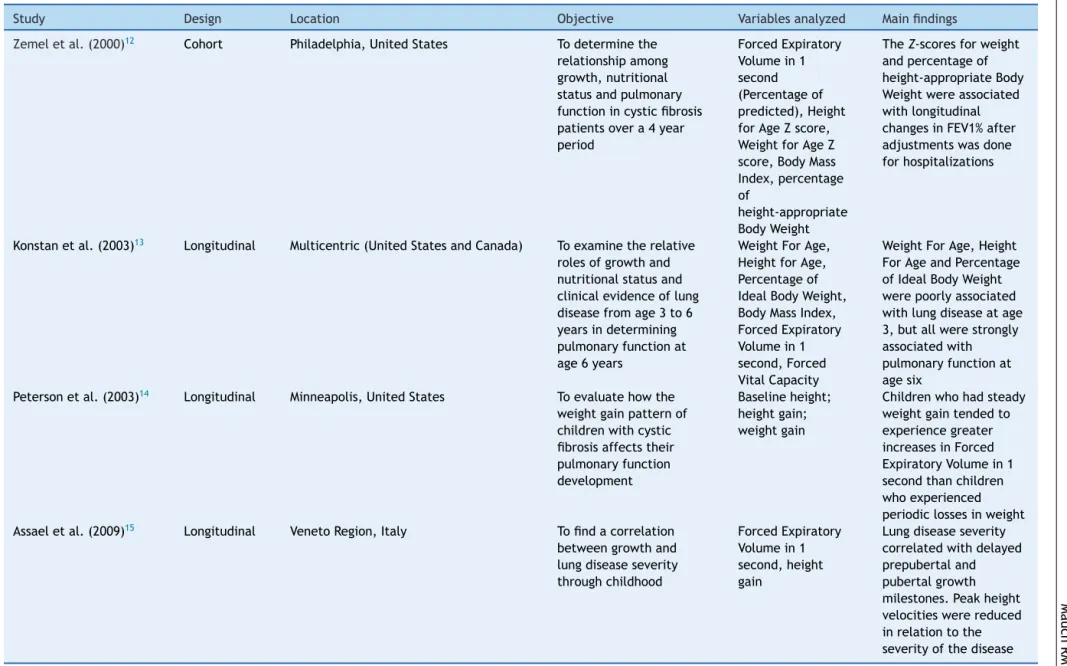
Table1 Descriptionofthestudiesincludedinthesystematicreviewpublishedbefore2010,distributedbyauthorship,design,location,objectiveorhypothesis,mainvariables
studiedandmainfindings.
Study Design Location Objective Variablesanalyzed Mainfindings
Zemeletal.(2000)12 Cohort Philadelphia,UnitedStates Todeterminethe
relationshipamong growth,nutritional statusandpulmonary functionincysticfibrosis patientsovera4year period
ForcedExpiratory Volumein1 second (Percentageof predicted),Height forAgeZscore, WeightforAgeZ score,BodyMass Index,percentage of
height-appropriate BodyWeight
TheZ-scoresforweight andpercentageof height-appropriateBody Weightwereassociated withlongitudinal changesinFEV1%after adjustmentswasdone forhospitalizations
Konstanetal.(2003)13 Longitudinal Multicentric(UnitedStatesandCanada) Toexaminetherelative rolesofgrowthand nutritionalstatusand clinicalevidenceoflung diseasefromage3to6 yearsindetermining pulmonaryfunctionat age6years
WeightForAge, HeightforAge, Percentageof IdealBodyWeight, BodyMassIndex, ForcedExpiratory Volumein1 second,Forced VitalCapacity
WeightForAge,Height ForAgeandPercentage ofIdealBodyWeight werepoorlyassociated withlungdiseaseatage 3,butallwerestrongly associatedwith pulmonaryfunctionat agesix
Petersonetal.(2003)14 Longitudinal Minneapolis,UnitedStates Toevaluatehowthe weightgainpatternof childrenwithcystic fibrosisaffectstheir pulmonaryfunction development
Baselineheight; heightgain; weightgain
Childrenwhohadsteady weightgaintendedto experiencegreater increasesinForced ExpiratoryVolumein1 secondthanchildren whoexperienced periodiclossesinweight Assaeletal.(2009)15 Longitudinal VenetoRegion,Italy Tofindacorrelation
betweengrowthand lungdiseaseseverity throughchildhood
ForcedExpiratory Volumein1 second,height gain
Association
of
growth
and
nutritional
parameters
with
pulmonary
function
in
cystic
fibrosis
507
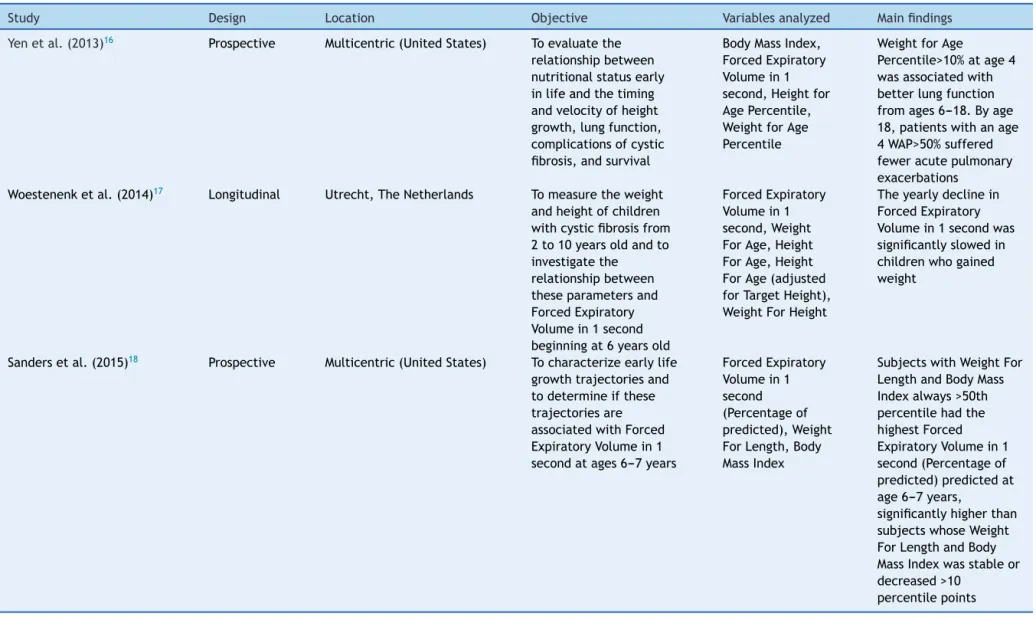
Table2 Descriptionofthestudiesincludedinthesystematicreviewpublishedafter2010,distributedbyauthorship,design,location,objectiveorhypothesis,mainvariables
studiedandmainfindings.
Study Design Location Objective Variablesanalyzed Mainfindings
Yenetal.(2013)16 Prospective Multicentric(UnitedStates) Toevaluatethe
relationshipbetween nutritionalstatusearly inlifeandthetiming andvelocityofheight growth,lungfunction, complicationsofcystic fibrosis,andsurvival
BodyMassIndex, ForcedExpiratory Volumein1 second,Heightfor AgePercentile, WeightforAge Percentile
WeightforAge
Percentile>10%atage4 wasassociatedwith betterlungfunction fromages6---18.Byage 18,patientswithanage 4WAP>50%suffered feweracutepulmonary exacerbations
Woestenenketal.(2014)17 Longitudinal Utrecht,TheNetherlands Tomeasuretheweight andheightofchildren withcysticfibrosisfrom 2to10yearsoldandto investigatethe relationshipbetween theseparametersand ForcedExpiratory Volumein1second beginningat6yearsold
ForcedExpiratory Volumein1 second,Weight ForAge,Height ForAge,Height ForAge(adjusted forTargetHeight), WeightForHeight
Theyearlydeclinein ForcedExpiratory Volumein1secondwas significantlyslowedin childrenwhogained weight
Sandersetal.(2015)18 Prospective Multicentric(UnitedStates) Tocharacterizeearlylife growthtrajectoriesand todetermineifthese trajectoriesare associatedwithForced ExpiratoryVolumein1 secondatages6---7years
ForcedExpiratory Volumein1 second (Percentageof predicted),Weight ForLength,Body MassIndex
SubjectswithWeightFor LengthandBodyMass Indexalways>50th percentilehadthe highestForced ExpiratoryVolumein1 second(Percentageof predicted)predictedat age6---7years,
significantlyhigherthan subjectswhoseWeight ForLengthandBody MassIndexwasstableor decreased>10
508 MauchRMetal.
about8monthslaterthanthatofmildpatients.Theirpeak velocity was lower by 1.3cm/year (vs. mild disease) and 2.0cm/year (vs. healthy subjects). When age, height and heightvelocityatallthefourgrowthmilestoneswere con-sideredasawhole,thedifferencesbetweenpatientswith mildandseverediseasewerehighlysignificant.
Yenetal.,16inaprospectiveobservationalstudy, evalu-ated3,142CFpatientsandfoundthatFEV1%waslowerin thegroupofpatientswithWAP<10%atage4yearsthanall other WAPgroups, neverreachinga FEV1>80% throughout thestudyperiod.Thisstudyalsofoundthatpatientsinthe highest weightandheight percentiles at age4 hadfewer pulmonaryexacerbations,spentfewerdaysinthehospital, andhadbettersurvivalat18yearsofage.
Woestenenk et al.,17 studying 156 children in a mean periodof7.4years,didnotfindcorrelationbetweenFEV1% andeitherweightorheight,inafirstcrosssectional analy-sis.However,regardlessoftheirinitialWFAorWFHcategory, children who increased in weight had minor declines in FEV1% predicted from 6 to 10 years old. The decline in FEV1%slowedby1.8%and1.9%,respectively,foreachunit of increase in WFA and WFH. The study did not find any associationbetweenFEV1andeitherHFAorHFA/TH.
Sanders etal.18 prospectivelystudied6,805 patientsin theCysticFibrosisFoundationPatientRegistry.Childrenwith CF born between 1994 and 2005 followed from age ≤2
through7yearswereassessedaccordingtochangesin annu-alizedWFLpercentilesbetweenages0and2yearsandBMI percentiles between ages2 and 6 years.The results of a multivariablelinearregressionmodelshowedthatsubjects withWFL-BMIalways>50thpercentilehadthehighestFEV1% predicted at age 6---7years, significantly higherthan sub-jectswhoseWFL-BMIwasstableordecreased>10percentile points.
Discussion
StudiesforthemanagementofCFpatientshavebeen con-tributing for the advance in the multidisciplinary care, aiming at the best treatment of this disease. Despite these improvements, pulmonary insufficiency remains as themain causeof deathin CF andtherearestrong asso-ciationsbetween growth and nutritional indices and lung function.19However,moststudiesreportingtheseevidences arecross-sectional,withfewevidencestosupport associa-tionbetween longitudinalchangesin growthandnutrition withchangesinlungfunctionthroughlife.
ThestudyconductedbyAssaeletal.15 wasthefirstone todemonstrate a clear association between early growth eventsandlungfunctioninCFpatients.Thisstudyshowed aprogressivelossofFEV1inpatientswithmild andsevere lungdisease.Inpatientswithseverelungdisease,the pre-pubertal take-off and peakoccurred later and at slightly lower velocity compared to patients with mild disease. Pubertalpeakof severepatientsoccurredabout8months later than that of mild patients. Theirpeak velocity was lowerby1.3cm/year(vs.milddisease)and2.0cm/year(vs. healthysubjects).Whenage,heightandheightvelocityat allthefourgrowthmilestoneswereconsideredasawhole, the differences between patients with mild and severe disease were highly significant. The main finding of this
study isthat lowheight velocityisan early manifestation oflungdiseaseseverityinCF.
Twostudies14,17didnotfindassociationsbetweenchanges inheightandchangesinFEV1,butthesestudieswere con-ductedinshorterperiodsoftime,and,differentlyfromtwo studies previously mentioned,15,16 their analyses included children whoseagesranged from2to10 yearsold.Thus, theinfluenceofgrowthspurtscouldnotbeassessed. How-ever, both studiespoint toan association betweenweight gainandbetterlungfunction.
Three studies12,13,18 reported that the improvement of bothgrowthandclinicalparametersinearlylifewas asso-ciated with a better lung function 2---5 years later. Thus, it issuggestedthat growthandnutritionalstatusin child-hoodmaybestrongpredictorsoftheseverityoflungdisease laterinlife,whichisreinforcedbyYenetal.,16whoshowed thatpatients inthe highestweightandheight percentiles at age 4years hadfewerpulmonary exacerbations, spent fewerdaysinthe hospital,and hadbettersurvivalat age 18years.
Pulmonary function abnormalities, includingdecreased peak flow and lower vital capacity, forced vital capac-ity, and forced expiratory flow, occur in other conditions in which children are malnourished and have stunted growth.20---23 Nutritional interventions with malnourished patients showed that enhanced caloricintake resulted in increased weight andheight gain velocities and improve-ments in other nutritional status measures, besides reductionincasesofpulmonaryinfectionsorslower deteri-orationinpulmonary function.10,24---26Growthandnutrition aretwointimately linkedcharacteristics, so,sincebetter nutritionisassociatedtobetterlung functioninCF, main-taining a healthy nutritional status is important not only for nutritionand growth, but for lung function aswell.27 Stephenson et al.28 studied a cohort of 909 CF patients. Subjectsintheoverweightandobesecategorieswereolder andpresentedbetterlungfunction.Withintheunderweight group,a10%increaseinBMIresultedina4%relativeincrease in FEV1 andindividuals witha BMI inthe adequate range hada5%relativeincreaseinFEV1.Thiswasthefirststudy tocharacterizechangesinnutritionalstatusoverttimeand toquantify the relation betweennutrition andlung func-tion across the spectrum of BMI categories. Regarding to improvementingrowth,theevidencesforclinicaltrialsare also limited. Growth hormone therapy does not seem to improvelungfunctionatasignificantlevel.29
Associationofgrowthandnutritionalparameterswithpulmonaryfunctionincysticfibrosis 509
are about 2000 mutations of the CFTR gene, distributed amongsixclasses.Thus,studiesofassociationamong varia-blesmust,inthefuture,bestructuredformutationclasses thatconfigureamoresevere disease(classesI,II andIII). The higher facility of access tomedicines, attendance at referencecenters,neonatalscreening,earlytreatmentfor
Pseudomonasaeruginosainfection,earlyintakeof pancre-aticenzymes,knowledgeofpolymorphismsanddifferential follow-up in adolescence and adulthood (mainly for the femalegender)arefactorsthatmayequilibrateand mod-ifythenatural historyofCFwithregardtothepulmonary functiondecline,growthandnutritionofthesepatients.
Funding
Thisstudydidnotreceivefunding.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
Wethank www.laboratoriomultiusuario.com.brand LAFIP/ CIPEDforthehelpinthesearch.
References
1.O’Sullivan BP, Freedman SD. Cystic fibrosis. Lancet. 2009;373:1891---904.
2.Knowles MR, Drumm M. The influence of genetics on cys-tic fibrosis phenotypes. Cold Spring Harb Perspect Med. 2012;2:a009548.
3.MarsonFAL,BertuzzoCS,HortencioTD,RibeiroJD,BonadiaLC, RibeiroAF.TheACEgeneD/Ipolymorphismasamodulatorof severityofcysticfibrosis.BMCPulmMed.2012;12:41.
4.MarsonFAL,BertuzzoCS,RibeiroAF,RibeiroJD.Polymorphisms inADRB2genecanmodulatetheresponsetobronchodilators andtheseverityofcysticfibrosis.BMCPulmMed.2012;12:50.
5.MarsonFAL, Rezende LM,Furgeri DT,Ribeiro AF,RibeiroJD, BertuzzoCS.ADRA2Ais a cysticfibrosismodifiergene.IntJ Genet.2013;5:125---31.
6.Marson FA, Marcelino AR, Ribeiro JD, Ribeiro JD, Bertuzzo CS.COX-2genepolymorphisms:geneticdeterminantsofcystic fibrosiscomorbidities.IntJGenet.2013;5:132---8.
7.LimaCS,OrtegaMM,MarsonFA,ZulliR, RibeiroAF,Bertuzzo CS.Cysticfibrosistransmembraneconductanceregulatorgene mutationsandglutathioneS-transferasenullgenotypesincystic fibrosispatientsinBrazil.JBrasPneumol.2012;38:50---6.
8.MarsonFA,BertuzzoC,SecolinR,RibeiroA,RibeiroJ.Genetic interactionofGSHmetabolicpathwaygenesincysticfibrosis. BMCMedGenet.2013;14:60.
9.Chmiel JF, Konstan MW, Elborn JS. Antibiotic and anti-inflammatory therapies for cystic fibrosis. Cold Spring Harb PerspectMed.2013;3,a009779.
10.MillaCE.Nutritionandlungdiseaseincysticfibrosis.ClinChest Med.2007;28:319---30.
11.DelCiampoIR,DelCiampoLA,SawamuraR,deOliveiraLR, Fer-nandesMIM.Nutritionalstatusofadolescentswithcysticfibrosis treatedatareferencecenterinthesoutheastregionofBrazil. ItalJPediatr.2015;41:51.
12.ZemelBS,JawadAF,FitzSimmonsS,StallingsVA.Longitudinal relationshipamonggrowth,nutritionalstatus,andpulmonary
function in childrenwithcysticfibrosis: analysisof the Cys-ticFibrosisFoundationNationalCFPatientRegistry.JPediatr. 2000;137:374---80.
13.Konstan MW, Butler SM, Wohl ME, Stoddard M, Matousek R, Wagener JS, et al. Growth and nutritional indexes in early life predict pulmonary function in cystic fibrosis. J Pediatr. 2003;142:624---30.
14.Peterson ML, Jacobs DR, Milla CE. Longitudinal changes in growth parameters are correlated with changes in pul-monary function in children with cystic fibrosis. Pediatrics. 2003;112:588---92.
15.AssaelBM,CasazzaG, IansaP,Volpi S,MilaniS.Growth and long-termlungfunctionincysticfibrosis:alongitudinalstudy ofpatientsdiagnosedbyneonatalscreening.PediatrPulmonol. 2009;44:209---15.
16.Yen EH, Quinton H, Borowitz D. Better nutritional status in early childhood is associated with improved clinical out-comesandsurvivalin patientswithcysticfibrosis.JPediatr. 2013;162:530---5.
17.WoestenenkJW,StellatoRK,Terheggen-LagroSW,vanderEnt CK,HouwenRH.Therelationshipbetweenbodygrowthand pul-monaryfunctioninchildrenwithcysticfibrosis.ActaPaediatr. 2014;103:162---7.
18.SandersDB,FinkA,Mayer-HamblettN,SchechterMS,Sawicki GS,RosenfeldM,etal.Earlylifegrowthtrajectoriesincystic fibrosisareassociatedwithpulmonaryfunctionatage6years. JPediatr.2015[Epub2desetembrode2015].
19.KeremE,VivianiL,ZolinA,MacNeillS,HatziagorouE, Ellemu-nter H,et al.Factors associatedwithFEV1declineincystic fibrosis: analysis of the ECFS Patient Registry. EurRespir J. 2014;43:125---33.
20.MillerGJ,SaundersMJ,GilsonRJ,AshcroftMT.Lungfunctionof healthyboysandgirlsinJamaicainrelationtoethnic composi-tion,testexerciseperformance,andhabitualphysicalactivity. Thorax.1977;32:486---96.
21.PrimhakR, CoatesFS. Malnutrition andpeak expiratory flow rate.EurRespirJ.1988;1:801---3.
22.NairRH,KesavachandranC,ShashidharS.Spirometric impair-mentsinundernourishedchildren.IndianJPhysiolPharmacol. 1999;43:467---73.
23.MukhopadhvayS,MacleodKA,OngTJ,OgstonSA.Ethnic vari-ation in childhood lung function may relate to preventable nutritionaldeficiency.ActaPaediatr.2001;90:1299---303.
24.Corey M,McLaughlin FJ, Williams M, LevisonH. A compari-son of survival, growth,and pulmonary function inpatients withcystic fibrosisin Bostonand Toronto. J ClinEpidemiol. 1988;41:583---91.
25.McPhailGL,ActonJD,FenchelMC,AminRS,SeidM. Improve-mentsinlungfunctionoutcomesinchildrenwithcysticfibrosis are associated with better nutrition, fewer chronic Pseu-domonasaeruginosainfections,anddornasealfause.JPediatr. 2008;153:752---7.
26.VanDevanterDR,PastaDJ,KonstanMW.Improvementsinlung function andheightamongcohortsof6-year-oldswithcystic fibrosisfrom1994to2012.JPediatr.2014;165:1091---7.
27.CysticFibrosisFoundation.Patientregistry:annualdatareport 2013.Bethesda:CysticFibrosisFoundation;2013.
28.StephensonAL,MannikLA,WalshS,BrotherwoodM,RobertR, Darling PB.Longitudinal trendsin nutritional statusand the relation between lungfunction and BMl in cystic fibrosis: a population-basedcohort.AmJClinNutr.2013;97:872---7.
29.Thaker V, Haagensen AL, Carter B, Fedorowicz Z, Houston BW. Recombinant growthhormone therapyfor cysticfibrosis in children and young adults. Cochrane Database Syst Rev. 2013;6:CD008901.