w w w . e l s e v i e r . c o m / l o c a t e / b j i d
The
Brazilian
Journal
of
INFECTIOUS
DISEASES
Original
article
Molecular
identification
of
viral
agents
associated
with
acute
conjunctivitis:
a
prospective
controlled
study
Emine
Akc¸ay
a,
Ahmet
C¸
arhan
b,
Gözde
Hondur
c,
Zeliha
Koc¸ak
Tufan
d,
Necati
Duru
e,
Selc¸uk
Kılıc¸
f,
Ezgi
Naz
Ensari
a,∗,
Nagihan
U ˘gurlu
a,
Nurullah
C¸
a ˘gıl
aaYıldırımBeyazıt,UniversityFacultyofMedicine,DepartmentofOphthalmology,Ankara,Turkey
bYıldırımBeyazıt,UniversityFacultyofMedicine,DepartmentofMedicalBiology,Ankara,Turkey
cUlucanlarEyeTrainingandResearchHospital,Ankara,Turkey
dYıldırımBeyazıtUniversity,FacultyofMedicine,DepartmentofInfectiousDiseasesandClinicalMicrobiology,Ankara,Turkey
eKayseriEducationandResearchHospital,OphthalmologyClinic,Kayseri,Turkey
fTurkeyPublicHealthInstitute,Ankara,Turkey
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received8October2016 Accepted29March2017 Availableonline20May2017
Keywords:
Adenovirus Conjunctivitis Viral
PCR
a
b
s
t
r
a
c
t
Background:Viralconjunctivitisarethemostfrequentinfectionsinophthalmologyclinics. Thediagnosisisusuallyrelyingonclinicalfindingsandmedicalhistory.However, topi-calantibioticsareoftenusedunnecessarilyadditiontosymptomatictreatmentbecauseof unsureagents.WeaimedtodetecttheAdenovirus,CoxsackievirusandEnterovirusfrom conjunctivaandpharyngealsamplesofpatients.
Methods:Theconjunctivaandpharyngealsamplesofthepatientswithconjunctivitiswere taken byVirocult transport media andkeptat −80◦Cup to studyday.Adenovirusspp,
Enterovirus70andEnterovirus71,CoxsackieA24andCoxsackieA16weredetectedby real-timePCR.Samplesfromhealthyhealthcareworkersofophthalmologyclinicwereusedfor controlgroup.
Results:Atotalof176samples(conjunctivalandpharyngealsamplesof62patientand26 healthysubjects)wereincluded.Themeanageof34(55.7%)maleand27(44.3%)female patientswas34±17.Twentyfive(40.3%)ofthepatientswerereceivingantibioticdropsat firstvisit.ThemainetiologicagentinconjunctivalsampleswasfoundtobeAdenovirus (46/62,74.2%)followedbyEnterovirus70(4/62,6.4%)andEnterovirus71(4/62,6.4%). Cox-sackievirus16and24werealsofoundin2patients(1/62each,1.6%).Pharyngealsamples werealsopositiveforAdenovirus(20/62,32.3%),Enterovirus70and71(7/62,11.3%and5/62, 8.1%respectively),Coxsackievirus16and24(2/62,3.2%and1/61,1.6%).
∗ Correspondingauthor.
E-mailaddress:[email protected](E.N.Ensari). http://dx.doi.org/10.1016/j.bjid.2017.03.016
Conclusions: Itisverydifficultinviralconjunctivitistomakeclinicaldifferentiationcaused bydifferentagentsbecauseofcommonclinicalsignsandsymptoms.Inroutineclinical work,theviralconjunctivitisusuallyrelatedwithAdenovirus.Butalmostonefourthofthe patients’conjunctivitiswerenotrelatedtoAdenovirus,whichshowstheimportanceofthe laboratorydiagnostics.Truediagnosisplaysanimportantroleonpreventionof contamina-tionandunnecessaryuseofantibioticsinviralconjunctivitis.
©2017SociedadeBrasileiradeInfectologia.PublishedbyElsevierEditoraLtda.Thisis anopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
Adenoviruses, a major cause of viral conjunctivitis,1–3 are
double-strandednon-envelopedDNAvirusesbelongingtothe familyAdenoviridae,genusMastadenovirus.Fifty-oneserotypes of human adenoviruses have been recognized and classi-fiedintosevenspecies(A-G)basedongenomesequencing, phylogenetic, and biological characteristics.4 Adenoviruses
areimplicatedinawiderangeofhumandiseasesincluding pharyngoconjunctival fever,an acute and highlyinfectious disease characterizedby fever, pharyngitis, acute follicular conjunctivitis,and regionallymphoidhyperplasia with ten-der,enlargedpreauricularadenopathy.1,3 Theserotypes3,4,
and7arefrequentlyassociatedwiththe pharyngoconjunc-tival fever. Epidemic keratoconjunctivitis (EKC) is a highly contagious,severeformofconjunctivitis,whichmayleadto outbreaksworldwide.Adenovirusserotypes8,11,19,and37 arecommonetiologicagentsofepidemickeratoconjunctivitis with severe symptoms, such as severe discharge, lacrima-tion,membraneformation,andmultiplesubepithelialcorneal infiltrates.Acutenonspecificfollicularconjunctivitisismostly caused byhumanadenovirus serotype 3, 4, 7,and 14,but it does not involve the cornea and the resulting conjunc-tivitis istypically mild. Nonspecific follicular conjunctivitis usuallyresolveswithinaweekto10dayswithouttreatment. Chronickeratoconjunctivitisistherarestformofocular ade-noviralinfection and iscaused byadenovirus type2, 3,4, and53.3,4 Acutehemorrhagicconjunctivitis(AHC)isan
epi-demicformofhighlycontagiousconjunctivitismostlycaused byEnterovirus70andCoxsackievirusA24variant.3,5 Herpes
simplexvirus,rubella,rubeola,varicellazoster,Epstein–Barr and Newcastle viruses are the other agents for viral conjunctivitis.6
Thediagnosisofviralconjunctivitisisusuallyperformed onthebasisofpatienthistoryandclinicalfindings,although serologic and molecular laboratory diagnoses are also cur-rentlyavailable.Unnecessaryantibiotictherapyisfrequently administered as a result of unknown etiology. The aim of this study was to identify the most common etiologic agentsofacuteconjunctivitisanddeterminetherelationship betweentheetiologicagentsandtheclinicalfindings, com-plications,andsystemicfindingsamongacuteconjunctivitis cases.
Methods
Clinicaldefinition
Aprospective,controlledclinicalstudywasconductedto eval-uate62consecutivelyenrolledpatientsthatwereadmittedto theAnkaraAtatürkTrainingandResearchHospitalbetween July2013andSeptember2014withsuspectedviral conjunc-tivitis (who had at least one of the following complaints and findings: hyperemia, lacrimation, foreign body sensa-tion,discharge,burning,follicularconjunctivitis,conjunctival hemorrhages,membraneformation,eyelidswelling,or con-junctivalhemorrhages)orkeratoconjunctivitis(thosewhohad punctatecornealdefectsorsubepithelialinfiltratesinaddition toviralconjunctivitisfindings).Twenty-sixhealthyvolunteers workingintheophthalmologydepartmentatalltimeswere includedascontrols.
ThisstudyfollowedthetenetsoftheDeclarationofHelsinki and was approved by the local ethics committee. Written informedconsentwasobtainedfromthestudyparticipants beforesamplecollection.
Samplecollection
Pharyngeal and conjunctival samples were collected from patientsandcontrolsbytwoexperiencedophthalmologists. Thesampleswereplacedinviraltransportmedium(Virocult, BD)withswabsandstoredat−80◦Cuntilanalysis.
Sampleprocessingandvirusidentification
MolecularidentificationwasusedforEnterovirus70/71. Cox-sackievirusA16/A24vandadenovirusweredeterminedusing areal-timePCRkit(DaAnGeneCo.,Ltd,Guangzhou,China) using virus-specificprimersandfluoresceinlabeledprobes. Viral DNA and RNA extraction were performed in a200l
sample volume using PureLink Viral DNA and RNA kit (Invitrogene, Thermo Fisher Scientific, Waltham, MA, USA) according to the manufacturer’s instructions. Afterelution ofviralDNAand RNAsamplesina50lelutionbuffer,the
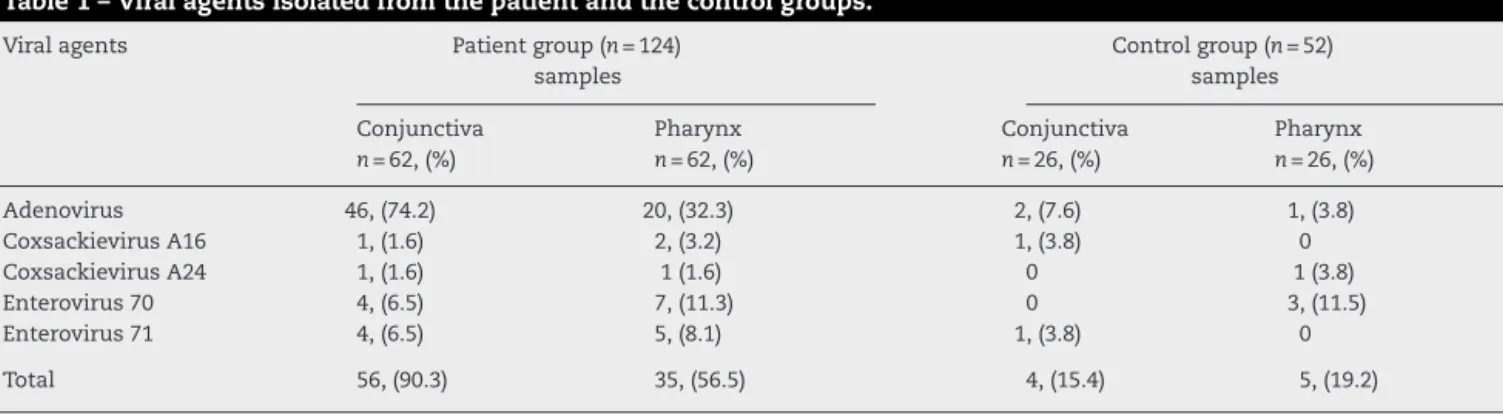
Table1–Viralagentsisolatedfromthepatientandthecontrolgroups.
Viralagents Patientgroup(n=124)
samples
Controlgroup(n=52) samples
Conjunctiva n=62,(%)
Pharynx n=62,(%)
Conjunctiva n=26,(%)
Pharynx n=26,(%)
Adenovirus 46,(74.2) 20,(32.3) 2,(7.6) 1,(3.8)
CoxsackievirusA16 1,(1.6) 2,(3.2) 1,(3.8) 0
CoxsackievirusA24 1,(1.6) 1(1.6) 0 1(3.8)
Enterovirus70 4,(6.5) 7,(11.3) 0 3,(11.5)
Enterovirus71 4,(6.5) 5,(8.1) 1,(3.8) 0
Total 56,(90.3) 35,(56.5) 4,(15.4) 5,(19.2)
CoxsackievirusA16/A24v, and Adenovirus were carried out according to the manufacturer’s instructions. Adenovirus reactionwasperformedinatotal45lreactionvolumeusing
2lsamplesupernatant,3lofTaqmixture,and40lofADV
PCRreactionsolution.Thereal-timePCRreactionconditions forADVwas onecycle of93◦Cfor2min,10 cyclesof93◦C for45sand55◦Cfor1min,and30cyclesof93◦Cfor30sand 55◦Cfor45s.Thereal-timePCRreactionsforEnterovirus70/71 andCoxsackievirusA16/A24vwere setat17lofPCR
reac-tion solutionA, 3lofPCRreaction solutionB,and 5lof
samplesupernatant.Thereal-timePCRreactionconditions forEnterovirus70/71andCoxsackievirusA16/A24vwereone cycle of50◦C for15min, onecycle of95◦Cfor 15minand 40 cycles of 94◦C for 15s and 55◦C for 45s. All real-time PCRreactionswererunwithnegativeandpositivecontrols. Datacollectioninallthereactionswassetasstep2(55◦C)of stage3.TheCycleThresholdValue(Ct)above30and38was acceptedasnegativeforAdenovirusand Enterovirus70/71, andCoxsackievirusA16/A24v,respectively.Allreal-timePCR reactionswereperformedusingAppliedBiosystems,7500Fast Real-TimePCRSystem(Applied Biosystems,ThermoFisher Scientific,Waltham,MA,USA).
AllStatisticalanalysiswasperformedusingSPSS12.0 soft-ware(SPSSInc.,Chicago,IL,USA).
Results
Atotalof124samples(62conjunctivaand62pharynx)from62 patientswerecollected.Themeanagewas34yearsformale (54.8%)and28forfemale(45.2%)patients;theoverallmeanage was34±17.Fifty-twosamples(26conjunctivaand26pharynx) from26healthycontrolswerealsocollected.Themeanage was8yearsformale(30.8%)and18forfemale(69.2%)controls; theoverallmean agewas39±10years.Twenty-five (40.3%) patientsreceivedantibioticdropsatthefirstvisit.
Amongthe62patientswithacuteconjunctivitis,50(80.6%) had conjunctiva samples withPCR positive for one ofthe viralagents.Bothconjunctivalandpharyngealsamplesin25 patients(40.3%)werePCRpositiveforoneoftheviralagents. Conjunctivaladenovirusisolatescorrelatedsignificantlywith pharyngealadenovirusisolates(r=0.407,p=0.01)(Table1).
Conjunctival samples of six patients were positive for mixedinfections.Adenoviruswasisolatedfromthree(50%) of the six Enterovirus 70 isolated from conjunctiva sam-ples; two (33.3%) of the six Enterovirus 71 isolated from
Table2–Viralagentsisolatedfromtheconjunctiva samplesofthepatientsreceivingantibioticdropsatfirst visit.
Viralagents Conjunctivasamplesn=25,(%)
Adenovirus 18,(72)
CoxsackievirusA16 1,(4)
CoxsackievirusA24 –
Enterovirus70 2,(8)
Enterovirus71 2,(8)
Total 23,(92)
conjunctivasamples,andone(16.7%)ofthesixCoxsackievirus A16isolatedfromconjunctivasamples.
Theclinicalpresentationwasbilateralin32.2%(20/62)of thepatients.Themostcommonsymptomswerehyperemia, lacrimation, foreign body sensation, discharge, and burn-ing, in decreasing order. Follicular conjunctivitis (n=54/64, 84.3%),eyelidswelling(n=36/62,58.1%),conjunctival hemor-rhages(n=9/62,14.5%),membraneformation(n=6/62,9.7%), punctate corneal defects (n=4/62, 6.4%), and subepithelial infiltrates (n=2/62, 3.2%) were the most reported findings in thepatient group. Theprevailing extraocularsymptoms were lymphadenopathy(14/62, 22.6%) and systemic symp-tomslikeheadacheandfever(12/62,19.4%).Pharyngitiswas alsoobservedin16.1%(10/62)ofthepatients.Seventy-six per-centofthepatientswhohadalreadyreceivedantibioticdrops attheirfirstvisithadPCRpositiveconjunctivalspecimens.In thisgroup,aswellasinthetotalstudygroup,thedetectedviral agentswereAdenovirus(18/25,72%),Enterovirus70(2/25,8%), Enterovirus71(2/25,8%),andCoxsackievirus16(1/25,4%),in decreasingorder.Coxsackievirus24wasnotdetectedinthis group(Table2).
activeinfectionweretheoneswithpunctatecornealepithelial defectsatinitialpresentation.
Discussion
Acuteconjunctivitisisarathercommondisease,whichmay affectmanypeopleandimposeeconomicandsocialburdens. Studies haveshownthat virusescause upto35–80%ofall casesofacuteconjunctivitis2,7,8andbetween65%and90%of
casesofviralconjunctivitisarecausedbyadenoviruses.1,3,5In
linewiththesestudies,inourinvestigationAdenoviruswas themostcommonly isolatedcausative agentofacute con-junctivitisfrombothconjunctivaandpharynxsamples(74.2% fromconjunctivasamples,32.3%frompharynxsamples).
The second most frequently observed causative agents were Enterovirus70 and Enterovirus71,respectively. Previ-ously,Lietal.isolatedCoxsackievirusA24asthesecondmost common viral agentfollowing adenovirusesforacute con-junctivitis,butnoEnterovirus70 wasisolated.Additionally, adenoviruseswerethe mostfrequentlyidentifiedagentsin co-infectionsofacuteconjunctivitis,whichisconcordantwith ourdata.5
Viralconjunctivitis,secondarytoadenoviruses,ishighly contagious,andthevirusspreadsthroughdirectcontactvia contaminatedfingers,medicalinstruments,swimmingpool water,orpersonalitems.Handwashingandisolationofthe infectedpatientsareessentialtoavoidtransmission.9None
ofthe caseshavea history ofexposuretoswimming pool water.In35%ofthecases,thecontaminationwasintrafamilial transmissionthroughhandsandpersonalitems.Noclinicians involvedinsamplecollectionorintreatingthepatientswere contaminatedbecauseproperprecautionsweretaken.
Redness,itching,burning,waterydischarge,foreignbody sensation, follicular conjunctivitis, membrane formation, lymphadenopathy,andhemorrhagesarecommonsymptoms inviralconjunctivitis.3,5Ourfindingsareinaccordancewith
theliterature,asthesamecommonsymptomswereobserved, makingclinical diagnosesmucheasier.Inthis study,some symptoms were significantly associated with adenoviruses (p<0.05).Forexample,conjunctivaladenoviruswasisolated fromallpatientswithconjunctivalmembranes,92.8%ofthe patientswithlymphadenopathy,and75%ofthepatientswith punctatestaining.However,therewerenosignificant correla-tionsamongothersymptomsandviralagents.
Thediagnosisoftheviralconjunctivitisisusuallymadeon thebasisofpatienthistoryandclinicalfindings.Viralcultures byconventional techniquesarethe goldstandard,butmay beinsensitiveforcertainsamplesandtakeupto21daysto developthecytopathiceffect.4PCRisausefultechniquethat
amplifiessmallamountsofviralDNAwithgreatsensitivity andspecificity.Alaboratoryconfirmationofthevirus-related etiologymightaidthephysicianinmakinganaccurate diag-nosisandtakinghygienicprecautions,andthereforereduce thespreadofthedisease.4,10Inthisstudy,wecollectedboth
conjunctivaand pharynxsamplesfrom patientswithacute conjunctivitisandusedthePCRmethodforidentificationof viral agents. We primarily observed among those patients withvaryingdemographiccharacteristicsanddiagnosedwith acuteconjunctivitisthatthemostcommonlydetectedagents
were viruses. Ofthe 62acuteconjunctivitis cases,80.6%of theconjunctivasampleswerePCRpositiveforoneoftheviral agents.Inaddition,in40.3%ofthepatients,bothpharyngeal andconjunctivalsamplesyieldedthesameviralagent.
Because of overlapping features in clinical presenta-tion,definitive diagnosisofinfectious conjunctivitiscanbe challenging.5Theresultofthisstudyrevealedthatalthough
thereweredifferencesinclinicalpresentation,therewerealso someoverlaps.Previously,Marangonetal.reporteda signif-icantcorrelationbetweenlaboratoryandclinicalfindingsin viraldiseases.11
Ourisolationofinfectiousviralagentsfromthesamplesof asymptomaticcontrolswhoworkedinophthalmologyclinics indicatescontaminationfromthepatients.
InthestudyofLietal.,singleinfectionswereobservedin 49.89%ofcasesandmixedinfectionsweredetectedin2.36%.5
Inourstudy,conjunctivalsamplesofsixpatients(9.5%)were positiveformixedinfections.Adenoviruswasisolatedfrom conjunctiva samples together with Enterovirus 70 in three patients, with Enterovirus 71 in two patients, and in one patienttogetherwithCoxsackievirusA16.Amongthepatients whowereinfectedwithmixedviralagents,thereasonforthe malepredominanceandtheagerangeof25–35maybedue totheincreasedexposuretimeandfrequencyofcontactwith thesourceofinfection.3,5
Althoughnoeffectivetreatmentexists,artificialtearsand coldcompressesmayrelievesomeofthesymptoms.6
Antibi-oticdropsarenotindicatedforviralconjunctivitisastheiruse may complicatetheclinicalpresentationbycausingallergy andtoxicity.3,12,13Mostofthemedicinesareprescribed
inap-propriately.Rationaldruguserequiresfivecriteriaincluding: accuratediagnosis,accurateprescription,accurate dispensa-tion,suitablepackaging,andpatientorientation.14Increased
antibiotic resistance is also of concern with frequent and inappropriate use of antibiotics. Antibiotic resistance also occurs inthemanagementofeyeinfections withantibiotic drops.15 Udehet al.demonstratedthat thecorrect
identifi-cationofpatientswithviralconjunctivitismightreducethe costsrelatedtoinadequateuseofantibioticsinpatientswith EKC.10Inappropriateantibioticdropsandnonsteroidal
anti-inflammatorydropsmay leadtohistologicalandstructural toxicityinconjunctiva.16,17 Inaddition,adenoviral
conjunc-tivitisisassociatedwithsignificantcomplications,including subepithelialinfiltrates,lacrimaldrainageabnormalities,and symblepharonformation.18
A rapid, inexpensive and accurate method for diagnos-ing adenoviralocularinfectionsisneedednotonlytolimit the transmissionofthevirus withincommunities,butalso toavoidthe expensive,unnecessary,and ineffectiveuseof antibiotictherapies.10
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. UchioE,TakeuchiS,ItohN,etal.Clinicalandepidemiological featuresofacutefollicularconjunctivitiswithspecial referencetothatcausedbyherpessimplexvirustype1.BrJ Ophthalmol.2000;84:968–72.
2. WoodlandRM,DarougarS,ThakerU,etal.Causesof conjunctivitisandkeratoconjunctivitisinKarachi,Pakistan. TransRSocTropMedHyg.1992;86:317–20.
3. O’BrienTP,JengBH,McDonaldM,RaizmanMB.Acute conjunctivitis:truthandmisconceptions.CurrMedResOpin. 2009;25:1953–61.
4. LynchJP,KajonEA.Adenovirus:epidemiology,globalspread ofnovelserotypes,andadvancesintreatmentand prevention.SeminRespirCritCareMed.2016;37:586–602. 5. LiJ,YangY,LinC,etal.Etiologyofacuteconjunctivitisdueto
coxsackievirusA24variant,humanadenovirus,herpes simplexvirus,andchlamydiainBeijing,China.JpnJInfect Dis.2014;67:349–55.
6. AmericanAcademyofOphthalmology.Cornea/external diseasepanel.Preferredpracticepatternguidelines: conjunctivitis-limitedrevision.SanFrancisco,CA:American AcademyofOphthalmology;2011.
7. StensonS,NewmanR,FedukowiczH.Laboratorystudiesin acuteconjunctivitis.ArchOphthalmol.1982;100:1275–7.
8.FitchCP,RapozaPA,OwensS,etal.Epidemiologyand diagnosisofacuteconjunctivitisataninner-cityhospital. Ophthalmology.1989;96:1215–20.
9.WarrenD,NelsonKE,FarrarJA,etal.Alargeoutbreakof epidemickeratoconjunctivitis:problemsincontrolling nosocomialspread.JInfectDis.1989;160:938–43. 10.PintoRDP,LiraRPC,ArietaCEL,CastroRS,BononSHA.
Prevalenceofadenoviralconjunctivitis.Clinics. 2015;70:748–50.
11.MarangonFB,MillerD,AlfonsoE.Laboratoryresultsinocular viraldiseases:implicationsinclinical-laboratorycorrelation. ArqBrasOftalmol.2007;70:189–94.
12.CronauH,KankanalaRR,MaugerT.Diagnosisand
managementofredeyeinprimarycare.AmFamPhysician. 2010;81:137–44.
13.KaufmanHE.Adenovirusadvances:newdiagnosticand therapeuticoptions.CurrOpinOphthalmol.2011;22:290–3. 14.NepaleseNationalFormulary.1sted.Nepal:Kathmandu
NepalMinistryofHealth;1997.
15.AsbellPA,ColbyKA,DengS,etal.OcularTRUST:nationwide antimicrobialsusceptibilitypatternsinocularisolates.AmJ Ophthalmol.2008;145:951–8.
16.SoodAK,GuptaA,DabralT.Indiscriminateuseoftopical antibiotics:amenace.IndianJOphthalmol.1999;47:121–4. 17.GaynesBI,FiscellaR.Topicalnonsteroidalanti-inflammatory
drugsforophthalmicuse:asafetyreview.DrugSaf. 2002;25:233–50.
18.KurnaAS,AltunA,OflazA,KaratayAA.Evaluationofthe impactofpersistentsubepithelialcornealinfiltrationsonthe visualperformanceandcornealopticalqualityafterepidemic keratoconjunctivitis.ActaOphthalmol.2015;93: