Indications for head computed tomography in children with mild
Indications for head computed tomography in children with mild
Indications for head computed tomography in children with mild
Indications for head computed tomography in children with mild
Indications for head computed tomography in children with mild
traumatic brain injury
traumatic brain injury
traumatic brain injury
traumatic brain injury
traumatic brain injury
Indicações de tomografia de crânio em crianças com trauma cranioencefálico
Indicações de tomografia de crânio em crianças com trauma cranioencefálico
Indicações de tomografia de crânio em crianças com trauma cranioencefálico
Indicações de tomografia de crânio em crianças com trauma cranioencefálico
Indicações de tomografia de crânio em crianças com trauma cranioencefálico
leve
leve
leve
leve
leve
ENRICO GHIZONI1; ANDREADE MELO ALEXANDRE FRAGA2; EMILIO CARLOS ELIAS BARACAT3; ANDREI FERNANDES JOAQUIM1;
GUSTAVO PEREIRA FRAGA4, TCBC-SP; SANDRO RIZOLI5 ; BARTO NASCIMENTO6
A B S T R A C T A B S T R A C T A B S T R A C T A B S T R A C T A B S T R A C T
The “Evidence Based Telemedicine - Trauma and Emergency Surgery” (TBE-CITE) performed a critical appraisal of the literature and selected the three most relevant and recent publications on the indications for head computed tomography (CT) scan in pediatric patients with mild traumatic brain injury (TBI). The first study identified patients with mild TBI, high and low risk factors for intracranial injuries detected on CT scan and the need for neurosurgical intervention. The second evaluated the guidelines of the National Institute of Clinical Excellence for pediatric patients with TBI. The outcome of this study was either performing a head CT scan or hospital admission. The last study identified and analyzed the patients in whom the CT scan is not necessary and consequently should not be routinely indicated. Based on the critical appraisal of the literature and expert discussion, the opinion of the TBE-CITE was to favor the adoption of the PECARN guidelines, proposing CT scans for children with GCS of 14, altered level of consciousness and palpable skull fracture, or when warranted by the physician experience, multiple findings or worsening symptoms.
Key words: Key words: Key words: Key words:
Key words: Craniocerebral trauma. Tomography. Skull. Neurosurgery. Child.
EBT-TACS Meeting on Dec 10th, 2013, with the participation of the following services: St. Michael’ Hospital e Sunnybrook Health Science Center,
University of Toronto, Toronto, Canada; Department of Pediatrics, Division of Trauma Surgery, and Division of Neurosurgery, School of Medical Sciences, University of Campinas, Campinas, SP, Brazil.
1. Assistant Physician, Division of Neurosurgery, Department of Neurology, School of Medical Sciences, University of Campinas, Campinas, SP, Brazil; 2. Assistant Physician, Department of Pediatrics, School of Medical Sciences, University of Campinas, Campinas, SP, Brazil; 3. Associated Professor, Department of Pediatrics, School of Medical Sciences, University of Campinas, Campinas, SP, Brazil; 4. TCBC-SP, FACS. Coordinating Professor, Division of Trauma Surgery, Department of Surgery, School of Medical Sciences, University of Campinas, Campinas, SP, Brazil; 5. FRCSC, FACS. Full Professor, Department of Surgery and Critical Care Medicine, University of Toronto; Director, Trauma, St Michael’s Hospital, Toronto, Canada; 6. Assistant Professor, Surgery, Department of Surgery, University of Toronto, Toronto, Canada.
INTRODUCTION
INTRODUCTION
INTRODUCTION
INTRODUCTION
INTRODUCTION
T
raumatic brain injury (TBI) is one of the most common indications for hospitalization among children, and is often associated with important morbidity and mortality1. In the United States, approximately 150-180 children per 100,000 people are hospitalized annually. Seventy-four to 80% of these children are classified as having mild TBI according to the Glasgow Coma Scale (GCS) scores, of 13-152. The majority of children sustaining mild TBI are discharged home after a brief period of observation in emergency departments. However, a small proportion (0.5%) of these pediatric patients might progress to neurological deterioration, requiring neurosurgical interventions3,4. Timely detection and evacuation of intracranial hematomas are fundamen-tal for favorable neurological outcomes in this population. Computed tomography (CT) is the diagnosticmethod of choice for early detection of traumatic intracranial hematomas4.
The liberal use of head CT for mild TBI may unnecessarily expose children to ionizing radiation, which in turn may increase the risk of developing leukemia and brain tumors by up to three-fold. In addition, the widespread use of head CT in mild TBI further increases health care costs5,6. Although guidelines for the use of head CT for adult patients with mild TBI are available, the indications for head CT in pediatric trauma patients remain controversial due to the limited evidence available to guide its use7,8. Due to the high prevalence of TBI in children and consequent widespread use of head CT, development of guidelines for its rational use is urgent.
on recommendations for head CT in mild TBI in pediatric populations. These studies represent medical practice in North America and Europe9,10,11.
Based on the evidence reviewed, recommendations for head CT in children with mild TBI were generated.
STUDY 1
STUDY 1
STUDY 1
STUDY 1
STUDY 1
“CATCH: a clinical decision rule for the use of computed tomography in children with minor head injury.” 9
Rationale Rationale Rationale Rationale Rationale
The lack of widely accepted evidence-based recommendations for the use of head CT in children with mild TBI.
Question Question Question Question Question
Proposal of a clinical decision rule for the use of head CT for pediatric patients with mild TBI.
Main findings Main findings Main findings Main findings Main findings
A clinical decision tool was proposed based on seven risk factors, which are classified in low and high risks. (Table 1).
The presence of at least one high risk factor had 100% sensitivity and 70,2% specificity for predicting the need for neurosurgical intervention, which would require that 30.2% of patients undergo head CT.
The presence of at least one high and one low risk factors had 98,1% sensitivity and 50,1% specificity for identifying intracranial lesions, which would require that 51.9% of patients undergo head CT.
Strenghts Strenghts Strenghts Strenghts Strenghts
1. Prospective multicentre study involving 10 academic pediatric centres, with large sample size.
2. The clinical decision rule was developed based on high sensitivity, which is reassuring for the clinician that, if used, patients who really requires head CT would not be missed.
3. The study first outcome is a composite outcome that includes not only CT findings but also the need for neurosurgical interventions, which addresses in part the issue that not all children had a head CT performed.
4. Head CTs reviewed by an independent radiologist, and by a second radiologist or a neurosurgeon in uncertain cases. If uncertainty persisted, the CT was considered normal.
5. Well-established inclusion criteria and trained outcome assessors.
Limitations Limitations Limitations Limitations Limitations
1. Not all children in the study underwent head CT. Therefore, it is unknown whether some children were asymptomatic, but with intracranial lesions.
2. It was unclear why some children were excluded from the study.
3. The clinical decision rule needs to be validated, and its economic impact evaluated.
4. Although with high sensitivity, the clinical decision tool has low specificity, indicating the need for head CT in only 51.9% of children with mild TBI. Among these children, only 0.5% will require neurosurgical intervention and 4-7% will have intracranial lesions.
5. The subgroup of children under 2 years of age is small (23 cases), which limits generazability and precision of estimates.
STUDY 2
STUDY 2
STUDY 2
STUDY 2
STUDY 2
“ The implications of National Institute of Clinical Excellence (NICE) guidelines on the management of children presenting with head injury “ 10
Rationale Rationale Rationale Rationale Rationale
Investigate the impact of NICE guidelines on the management of children with head injury, as compared with the protocol proposed by “The Royal College of Surgeons of England (RCS)”.
Table 1 Table 1Table 1 Table 1
Table 1 – Risk factors for the presence of intracranial lesion.
High Risk High RiskHigh Risk High Risk High Risk
- GCS < 15 two hours following injury
- Suspected open and/or depressed cranial fractures - History of worsening headache
- Irritability on clinical examination Low Risk
Low RiskLow Risk Low Risk Low Risk
- Any signs of basal skull fracture - Large subgaleal hematoma
Question Question Question Question Question
Do NICE guidelines increase the rate of head CT and reduce admissions in children with head injury?
Main findings Main findings Main findings Main findings Main findings
NICE guidelines led to higher rates of head CT utilization and lower admission rates than the RCS protocol in children with head injury. The study composite outcome included rates of head radiographs and CTs and hospital admission. High risk patients (table 2) underwent head CT with the intent to potentially avoid unnecessary hospital admissions.
Strenghts Strenghts Strenghts Strenghts Strenghts
1. The study addresses an important public health issue. Implementing the NICE guidelines has the potential to decrease admission rates, and thus to reduce health care costs in head injury management.
2. Large multicenter study, which allows more precision in estimates and generazability of findings.
3. The study first outcome is a composite outcome that includes not only CT findings but also the need for neurosurgical interventions, which addresses in part the issue that not all children had a head CT performed.
Limitations Limitations Limitations Limitations Limitations
1. The study utilized data from a prospective multicenter study; thus, it retrospectively applied the guidelines based on simulation.
2. The outcomes were the need for head radiographs or CTs, and need for hospital admission. It did not address the need for neurosurgical interventions, nor the presence of intracranial findings on CT
3. It included all children 16 years of age or younger, with no distinction on the severity of head injury. No other exclusion criteria apart from refusal to participate.
4. Eleven high-risk factors included, which makes the clinical decision rule difficult to implement.
STUDY 3
STUDY 3
STUDY 3
STUDY 3
STUDY 3
“ Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study “ 11
Rationale Rationale Rationale Rationale Rationale
The need for prospectively developing clinical decision rules for the use of head CT in different centres in children with mild TBI; and particularly developing specific criteria for children under 2 years of age.
Question Question Question Question Question
Determine criteria that identify a subgroup of children with very low risk of clinically important (ci) head injury where head CT can be avoided.
Main findings Main findings Main findings Main findings Main findings
Out of 42,000 pediatric patients prospectively evaluated, 15,000 (35.3%) required head CT, 376 children (0.9%) sustained ciTBI, and only 60 patients (0.1%) needed neurosurgical interventions. Recommendations for two subgroup of children were developed: under 2 years of age and 2 years or older.
Children without any risk factors listed on the table can be classified as being low-risk, and do not require head CT (< 2 years – 53.5%; 2 years or older – 58.3%). In children under 2 years, the clinical rule both had a negative predictive value and a sensitivity of 100%; whilst in children 2 years or older, its negative predictive value and sensitivity were 99.95% and 96.8%, respectively.
Strenghts Strenghts Strenghts Strenghts Strenghts
1. Patients with GCS < 14, where the risk of a positive head CT is 20%, were excluded, which prevented artificially improving the clinical decision rule performance. Similarly, asymptomatic patients and patients with non-significant mechanisms of trauma were excluded.
2. Large prospective multicenter study, which allowed the development of specific criteria for the subgroup of children less than 2 years of age.
Table 2 Table 2 Table 2 Table 2
-Table 2 - NICE guidelines for performing head CT in high-risk patients.
- GCS< 13
- GCS13 - 14 2 h following injury
- Suspected open and/or depressed skull fracture - Any sign of basal skull fracture
- Post-traumatic seizure - Focal motor deficit - Two or more vomits
- Amnesia lasting over 30 minutes - 65 years or older
- Coagulopathy
3. The clinical decision rule is simple and easy to use clinically.
4. The main outcome of interest was defined as clinically important TBI, which was important to prevent missing patients with normal head CT, but clinically significant TBI (concussions).
Limitations Limitations Limitations Limitations Limitations
1. The study was conducted in pediatric academic hospitals, where the rates of head CT are below than the national average in non-academic centres. Therefore, the real impact of this clinical decision rule remains uncertain in non-academic hospitals.
2. Due to ethical reasons, head CT was not performed in all children, which might have affected the performance (predictive values and sensibility) of the clinical decision tool.
3. Long-term neuro-cognitive outcomes were not evaluated in the study.
CONCLUSIONS
CONCLUSIONS
CONCLUSIONS
CONCLUSIONS
CONCLUSIONS
Fortunately, children with mild TBI encompass the vast majority of emergency room visits for head injury, displaying low rates of intracranial lesions and rarely necessitating neurosurgical intervention. Therefore, the risk of ionizing radiation exposure should be pondered against the low prevalence of clinically important TBI in the pediatric population. Guidelines on the use of head CT for mild TBI are fundamental for a more rational management of children with head injury. These guidelines should be simple and easy to apply in different clinical settings.
Our EBT-TACS group critically appraised the three most relevant multicentre studies addressing clinical decision rules for the use of head CT in children with mild TBI. Recommendations, which would also apply to local Brazilian emergencies. were generated for the use of head CT in children presenting with mild TBI.
The following conclusions were drawn:
1. Currently, clinical decision rules for the use of head CT are available to instruct families and guide medical practice, with the advantage of potentially avoiding unnecessary ionizing radiation exposure in pediatric populations.
2. Simple clinical decision rules can be easily applied in different settings, particularly non-academic and non-specialized centres, with the potential to reduce the rates of unnecessary head CT utilization.
3. Compliance with available clinical decision rules for the use of head CT in pediatric populations can potentially reduce health care costs and prevent ionizing radiation exposure in children.
Recommendations Recommendations Recommendations Recommendations Recommendations
These authors believe that the protocol proposed by the PERCAN study (study 3) is the most robust and objective, validated. and simple to apply clinically for the use of head CT in children presenting with mild TBI. As a result, our EBT-TACS group recommends using these decision rules when deciding on the need for head CT in children presenting with mild TBI. Compliance with these rules allows physicians to stratify patients in different risk categories; it has the potential to benefit children, preventing radiation exposure; and can potentially minimize health care costs.
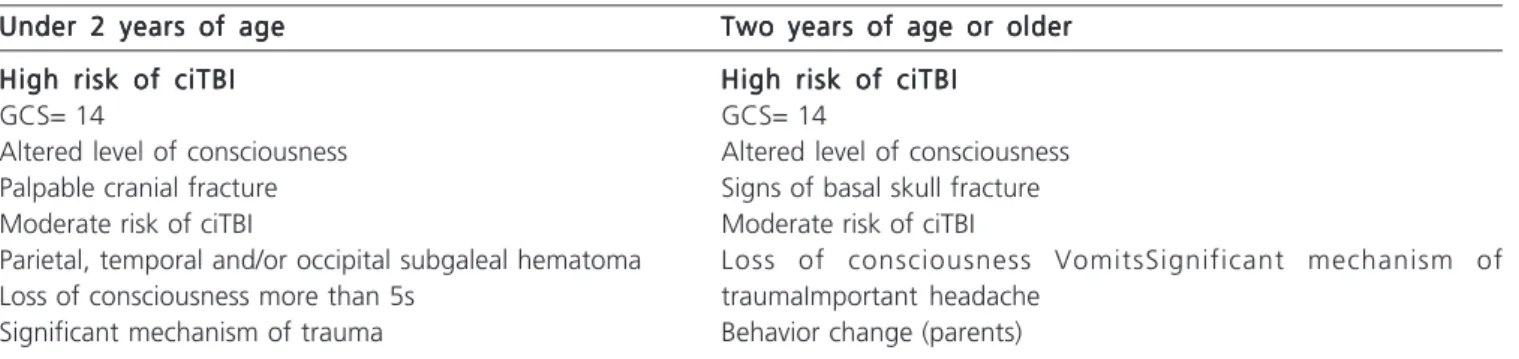
Table 3 Table 3Table 3 Table 3 Table 3
Under 2 years of age Under 2 years of ageUnder 2 years of age Under 2 years of age
Under 2 years of age Two years of age or olderTwo years of age or olderTwo years of age or olderTwo years of age or olderTwo years of age or older High risk of ciTBI
High risk of ciTBIHigh risk of ciTBI High risk of ciTBI
High risk of ciTBI High risk of ciTBIHigh risk of ciTBIHigh risk of ciTBIHigh risk of ciTBIHigh risk of ciTBI
GCS= 14 GCS= 14
Altered level of consciousness Altered level of consciousness
Palpable cranial fracture Signs of basal skull fracture
Moderate risk of ciTBI Moderate risk of ciTBI
Parietal, temporal and/or occipital subgaleal hematoma Loss of consciousness VomitsSignificant mechanism of
Loss of consciousness more than 5s traumaImportant headache
Significant mechanism of trauma Behavior change (parents)
R E S U M O R E S U M O R E S U M O R E S U M O R E S U M O
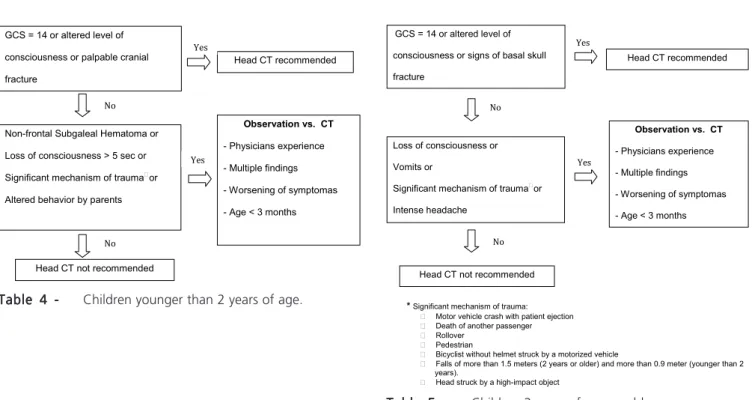
Table 4 Table 4 Table 4 Table 4
-Table 4 - Children younger than 2 years of age.
Tab Tab Tab Tab
Tabllllle 5 -e 5 -e 5 -e 5 -e 5 - Children 2 years of age or older.
REFERENCES
REFERENCES
REFERENCES
REFERENCES
REFERENCES
1. Snyder CL, Jain VN, Saltzman DA, Strate RG, Perry JF, Leonard AS. Blunt trauma in adults and children: a comparative analysis. J Trauma. 1998;30:1239-45.
2. Durkin MS, Olsen S, Barlow B, Virela A, Connolly Jr ES. The epidemiology of urban pediatric neurological trauma: evaluation of, and implications for, injury prevention program. Neurosurgery. 1998;42:300-10.
3. Tran T, McGuire T, Malcolm C, et al. Incidence of delayed intracranial hemorrhage in children with an uncomplicated minor head injury [abstract]. Pediatr Res. 2002;50:83.
4. Galbraith S. Misdiagnosis and delayed diagnosis in traumatic intracranial haematoma. BMJ. 1976;1:1438-9.
5. Brenner DJ, Hall EJ. Computed tomography - An increasing source of radiation exposure. N Engl J Med. 2007;357: 2277-84. 6. Pearce MS, Salotti JA, Little MP et al. Radiation exposure from CT
scans in childhood and subsequent risk of leukaemia and brain tumors: a retrospective cohort study. Lancet. 2012;380:499-505. 7. Stiell IG, Wells GA, Vandemheen K, et al. The Canadian CT head rule for patients with minor head injury. Lancet. 2001;357:1391-6.
8. Haydel MJ, Preston CA, Mills TJ, et al. Indications for computed tomography in patients with minor head injury. N Engl J Med. 2000;343:100-5.
9. Osmond MH, Klassen TP, Wells GA, et al. CATCH: a clinical decision rule for the use of computed tomography in children with minor head injury. CMAJ. 2010;182:341---8.
10. Dunning J, Daly JP, Malhotra R, et al. The implications of NICE guidelines on the management of children presenting with head injury. Arch Dis Child. 2004;89:763-7.
11. Kuppermann N, Holmes JF, Dayan PS, et al. Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet. 2009;374:1160---70.
S t a t e m e n t S t a t e m e n t S t a t e m e n t S t a t e m e n t S t a t e m e n t
The opinions and assertions contained herein represent the private views of the participants of the Evidence-based Telemedicine - Trau-ma and Acute Care Surgery (EBT-TACS) Journal Club, and are not to be construed as reflecting the views of the institutions that they represent.
Received on 01/12/2012
Accepted for publication 06/12/2012 Conflict of interest: None.
Source of funding: None.
How to cite this article: How to cite this article: How to cite this article: How to cite this article: How to cite this article:
Ghizoni E, Fraga AMA, Baracat ECE, Joaquim AF, Fraga GP, Rizoli S, Nascimento B. Indications for head computed tomography in children with mild traumatic brain injury. Rev Col Bras Cir. [periódico na Internet] 2013;40(6). Disponível em URL: http://www.scielo.br/rcbc
Address for correspondence: Address for correspondence: Address for correspondence: Address for correspondence: Address for correspondence: Dr. Enrico Ghizoni, MD, PhD E-mail: ghizonie @ gmail.com
analisou e identificou os pacientes onde a TC de crânio seria desnecessária e, portanto, não deve ser feita rotineiramente. Baseado nessa revisão crítica da literatura e a discussão com especialistas, o TBE-CiTE concluiu que é importante evitar a exposição desneces-sária de crianças com TCE leve à radiação ionizante da TC de crânio. O grupo favoreceu a utilização do guideline do PECARN onde ECG de 14, alteração do nível de consciência ou fratura do crânio palpável são indicações de TC de crânio, ou quando a experiência do médico, achados múltiplos ou piora dos sintomas ocorrerem.
Descritores Descritores Descritores Descritores