w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Quality
of
life
in
stomized
oncological
patients:
an
approach
of
integrality
from
Brazilian
Unified
Health
System
Cristilene
Akiko
Kimura
a,b,∗,
Ivone
Kamada
c,
Dirce
Bellezi
Guilhem
caUniversidadedeBrasília(UnB),Brasília,DF,Brazil
bFaculdadedeCiênciaseEducac¸ãoSenaAires(Facesa),ValparaísodeGoiás,GO,Brazil
cPost-GraduatePrograminNursing,FaculdadedeCiênciasdaSaúde,UniversidadedeBrasília(UnB),Brasília,DF,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30April2015 Accepted6December2015 Availableonline1February2016
Keywords:
Qualityoflife Ostomy
Colorectalneoplasms IntegralityinHealth UnifiedHealthSystem
a
b
s
t
r
a
c
t
Introduction:IntegralityisconsideredanessentialconstitutionaldoctrinalprincipleofSUS, beingconsideredasamajorchallengeinhealthinBrazil.Thisinvolvespracticingfocusing onthequalityoflifeofoncologicalstomizedpeople.
Objective:ToanalyzequalityoflifeofoncologicalstomizedpeoplefromtheHealth Depart-ment,theFederalDistrict,Brazil,fromtheperspectiveofintegralityoftheUnifiedHealth SysteminBrazil.
Methods:Cross-sectional,exploratoryanddescriptivestudywithaquantitativeand qualita-tiveapproachinthelightofacontentanalysis.Thiswasaconveniencesample,including120 patientsregisteredintheStomizedPeopleProgramoftheHealthDepartment,theFederal District,Brazil.Inthisstudy,sociodemographic,clinical,andWHOQOL-brefquestionnaires andanindividualinterviewwereused.DatawereanalyzedbyMicrosoft®OfficeExcel2010 programandSPSS20.0software.Statisticalsignificancewasacceptedat5%.
Results:Physical,SocialAffairs,andEnvironmentdomainsarecorrelatedwiththemean score,withstatisticallysignificantresults(p<0.0001),thecontentanalysisresultedinthree categories:complicationswiththestoma,self-care,andComprehensivehealthcare.
Conclusion:Ourresultshighlighttheneedtorealizetheintegralityasaprincipleatvarious levelsofdiscussionandofthepracticeofhealthcareforstomizedoncologicalpeople.
©2016SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
Qualidade
de
vida
de
estomizados
oncológicos:
uma
abordagem
da
integralidade
do
SUS
do
Brasil
Palavras-chave:
Qualidadedevida Ostomia
r
e
s
u
m
o
Introduc¸ão:Aintegralidadeéconsideradaumprincípiodoutrinárioconstitucionale essen-cialdoSUS,eéapreciadacomoumgrandedesafionoâmbitodasaúdenoBrasil.Istoimplica práticasvoltadasparaaqualidadedevidadaspessoasoncológicasestomizadas.
∗ Correspondingauthor.
E-mail:[email protected](C.A.Kimura).
http://dx.doi.org/10.1016/j.jcol.2015.12.003
Neoplasiascolorretais Integralidadedesaúde SistemaÚnicodeSaúde
Objetivo: AnalisaraqualidadedevidadepessoasoncológicasestomizadasdaSecretária deSaúdedoDistritoFederal,Brasil,sobaperspectivadaintegralidadedoSistemaÚnicode SaúdedoBrasil.
Métodos:Estudotransversal,exploratório-descritivocomabordagemquantitativae qualita-tivaàluzdaanálisedeconteúdo.Aamostrafoiconstituídaporconveniência,cominclusão de120pacientescadastradosnoProgramadeEstomizadosdaSecretariadeSaúdedoDistrito Federal,Brasil.Oestudoutilizouosquestionáriossóciodemográfico,clínico,eo WHOQOL-brefeumaentrevistaindividual.OsdadosforamanalisadospelosprogramasMicrosoft® OfficeExcel2010eSPSS20.0.Asignificânciaestatísticaaceitafoide5%.
Resultados:OsDomíniosFísico,Relac¸õesSociaiseMeioAmbienteestãocorrelacionadoscom oescoremédio,comsignificânciaestatística(p<0,0001),eaanálisedeconteúdoresultouem trêscategorias:Complicac¸õescomaestomia,AutocuidadoeAssistênciaintegralàsaúde.
Conclusão: Ficaevidenciadaanecessidadedeseperceberaintegralidadecomoprincípio emváriosníveisdediscussõesedepráticadocuidadoemsaúdeparapessoasoncológicas estomizadas.
©2016SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Introduction
Theconceptofintegralityallowsfortheidentificationofthe subjectinitsentirety,evenifnotreachableinitsfullness, con-sideringthewholeuniverseofpossibledimensionsamenable tointervention,throughtheaccessallowedbythemselves.1
Thus,integralitysuggeststheadditionandenhancement ofcareinthehealthprofessions,notbeingdefinedonlyas abasic guideline ofthe UnifiedHealthSystem (SUS). That is,integralitycan beunderstood asaconjugateofrelevant notionstoanexpandedassistance,withcoordinationofthe actionsoftheprofessionalsinvolvedinacomprehensive per-spectiveofthehumanbeingendowedwithfeelings,desires, anxietiesandrationalities.2
Integrality isconsidered an essential constitutional and adoctrinal principle ofSUS;therefore, it is appreciated as a majorchallenge inhealth in Brazil, inthe construction, deploymentandimplementationprocessofacaremodelthat hasitsfoundationanditsguidelinesbasedonthepromotion, prevention, cure and rehabilitation. This implies practices focusedonpeople’squalityoflife.2
Inthissense,weare facedwithamajorchallengefora comprehensivehealthcareofstomaoncologypeople,since thestomizedpatients’qualityoflifeimpliesthemaximum achievementofwell-beingandautonomy.3,4
Colorectalcancerisoneoftheleadingcausesforthe mak-ingofastoma.Amongtheriskfactorsforthistypeofcancer, thereisadirectlinktothedietary pattern,representedby vicesandbadeatinghabitsthatpromotebacterialgrowthand theconsequentdegradationofbileacids,resultingin produc-tionofcarcinogens.3–5 Colorectalcanceristhesecondmost prevalentcancerintheworld,rankingthirdintermsof inci-denceformenandinsecondplaceforwomen,whichmakes thisneoplasminseriousworldwidepublichealthproblem.It isconsideredoneofthemostimportantcancersintheadult population,withincreasingincidenceandmortalityinmost countries.4–8
Furthermore,stomizedoncologicalpeople,although resist-ing against cancer, find themselves with decreased body
imageandself-esteem,andwithdesiresofrejection.The sig-nificanceofthechangeintheirphysicalbodyandthesuffering inthefaceofthenewlivingconditionaffecttheirphysicaland psychologicalaspects,aswellasthoseoftheirsocialand envi-ronmentalrelations,andtheresultisanimpairmentoftheir qualityoflife.4,5
It isessential, however, to implement healtheducation actionsintheperspectiveofintegrality,establishing compre-hensivecaretothestomizedoncologicalperson,sothat,in general,healthprofessionalsinvolvedwiththisuniverseof patientshaveabroadervisionwithrespecttotheemergent feelingsinthefaceofdisease,themakingofabowelostomy, itssequels,andofrehabilitation,inordertoensurea com-prehensivehealthcarethatwillcontributetoimprovingthe qualityoflifeofstomizedoncologicalpeople.
Basedonthisnotion,theaimofthisstudywastoassessthe qualityoflifeofstomizedoncologicalpeoplefromtheHealth Department,theFederalDistrict,Brazil,fromtheperspective ofintegralityoftheUnifiedHealthSysteminBrazil.
Material
and
methods
Studymethodology
Thisis across-sectional, exploratory and descriptivestudy withquantitativeandqualitativeapproach,inlightofthe con-tentanalysis.Participantsincludedinitbelongedtoagroup ofintestinalstomized peopledue tocolorectalcancer.The observationandmeasurementofthevariablesofinterestwere madesimultaneously,andworkedasastatisticalsnapshotof whatoccursatanygiventime.
The interview data collection was analyzed in light of BardinContentAnalysis,whichisfoundeduponthephaseof descriptionorpreparationofmaterial,inferenceordeduction, andinterpretation.9
thestudysignedaFreeandInformedTermofConsent,after receivingdetailed explanationson proposedobjectives and procedures.Participantshadassuredtheguaranteeofsecrecy aboutthe origin ofthe dataand alsoaboutthe anonymity ofvolunteers,asstatedinBrazilianregulationsforresearch involvinghumanbeings.10
Inthissense,torespecttheanonymityofvolunteers,each interviewismarkedwiththeletter“I”(individual)anda num-berindicatingtheorderofitsrealization.
Casesstudied
Ourswasaconveniencesample,consideringthespontaneous demandforparticipationinthestudy.Thesampleincluded 120subjectswithbowelostomyduetocolorectalcancerand registeredintheOutpatientCareProgramforStomized Peo-pleoftheHealthDepartment, Brasilia,theFederalDistrict, Brazil.
Theinclusioncriteriawere:patientsdiagnosedwith col-orectal cancer who underwent a stoma surgery and aged
≥20years.Children,adolescents,pregnantwomen,nursing mothers,bedriddensubjects,peoplewithother disabilities, and people who refused to participatein the survey were excluded.
Datacollection
Data was collected from March 2010 to August 2012. For data collection, two instruments were applied: a socio-demographicand clinical questionnaireand the WHOQOL-bref version validated for the Portuguese. This latter instrumentconsistsof26items:twogeneralquestionswhich refertotheperceptionofqualityoflifeandsatisfactionwith health.WHOQOL-brefiscomposedoffourdomains(Physical, Psychological,SocialandEnvironmentalAffairs).11
Followingeachreportcollection,theinterviewswere tran-scribedverbatim.Readingthespeecheswasheldseveraltimes and at various times in their entirety, to makeit possible tounderstandthespeeches,identifyingmainideasandkey words, and observing repetitions and similarities between interviews.Thenextstagewasthephaseofinterviewcutouts, tobeginthecategorization.
Statisticalanalysis
In addition to the interview, a descriptive statistical anal-ysis of the socio-demographic and clinical questionnaire wascarriedout.DatafromtheWHOQOL-brefquestionnaire wereanalyzedbycalculating themean,standard deviation and proportions, and by inferential analysis through the followingstatisticalprocedures:confidenceinterval95%, Stu-dent’sttestwithanormaldistribution,andMann–Whitney testwithout normal distribution, and Pearson’scorrelation coefficient.
StatisticalanalysiswasperformedwithSPSSsoftware (Sta-tisticalPackagefor the SocialSciences, SPSSInc., Chicago, USA) for Windows® version 20.0, as recommended by the World Health Organization. The statistical significance acceptedwas5%.
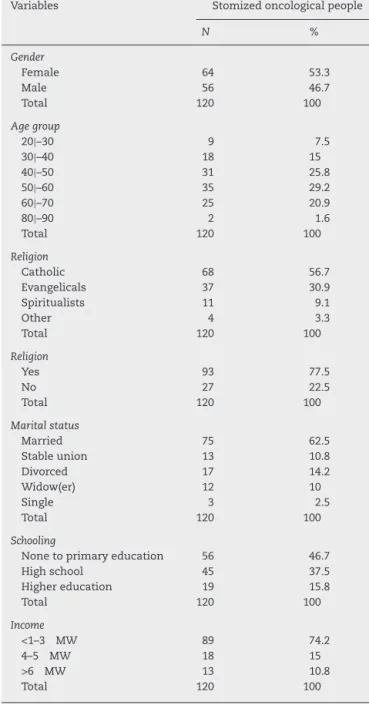
Table1–Stomizedoncologicalpeople’ssample, accordingtosociodemographiccharacteristics(Brasilia, theFederalDistrict,Brazil,2015).
Variables Stomizedoncologicalpeople
N %
Gender
Female 64 53.3
Male 56 46.7
Total 120 100
Agegroup
20|–30 9 7.5
30|–40 18 15
40|–50 31 25.8
50|–60 35 29.2
60|–70 25 20.9
80|–90 2 1.6
Total 120 100
Religion
Catholic 68 56.7
Evangelicals 37 30.9
Spiritualists 11 9.1
Other 4 3.3
Total 120 100
Religion
Yes 93 77.5
No 27 22.5
Total 120 100
Maritalstatus
Married 75 62.5
Stableunion 13 10.8
Divorced 17 14.2
Widow(er) 12 10
Single 3 2.5
Total 120 100
Schooling
Nonetoprimaryeducation 56 46.7
Highschool 45 37.5
Highereducation 19 15.8
Total 120 100
Income
<1–3 MW 89 74.2
4–5 MW 18 15
>6 MW 13 10.8
Total 120 100
Results
Table1liststhesociodemographiccharacterization.Themean
ageofparticipantswas58.72±12.56years;mostvolunteers were included in the age group between 50 and 69 years (n=66). A higher prevalence of females was noted, 53.3% (n=64).
Catholic religionisthe predominantfaith,56.7%(n=68), followedbyevangelicalcults,30.9%(n=37);and77.5%(n=93) ofparticipantsreportedbeingpractitionersofareligionand 22.5% (n=27) mentioned not being linked to any religious group.
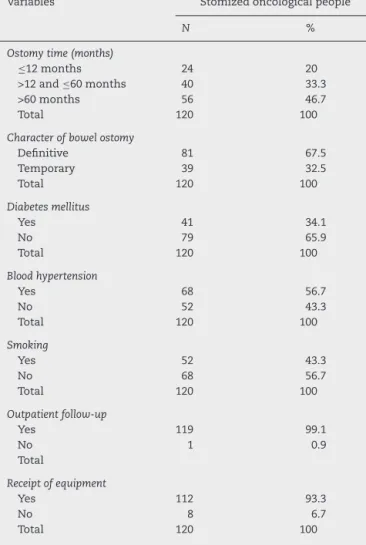
Table2–Stomizedoncologicalpeople’ssample, accordingtoclinicalcharacteristics(Brasilia,theFederal District,Brazil,2015).
Variables Stomizedoncologicalpeople
N %
Ostomytime(months)
≤12months 24 20
>12and≤60months 40 33.3
>60months 56 46.7
Total 120 100
Characterofbowelostomy
Definitive 81 67.5
Temporary 39 32.5
Total 120 100
Diabetesmellitus
Yes 41 34.1
No 79 65.9
Total 120 100
Bloodhypertension
Yes 68 56.7
No 52 43.3
Total 120 100
Smoking
Yes 52 43.3
No 68 56.7
Total 120 100
Outpatientfollow-up
Yes 119 99.1
No 1 0.9
Total
Receiptofequipment
Yes 112 93.3
No 8 6.7
Total 120 100
school.Asforemploymentstatus,themajorityofthegroup, 65.8%(n=79),consistedofretirees.Themonthlyincomemost relatedbytheparticipants,74.2%(n=89),stoodintherangeof 1–3timestheminimumwage.
Table2illustratesanoverviewofthe clinical aspectsof
volunteers.Thevariable“intestinalostomytimedueto col-orectalcancer”indicatedapredominanceintherangeof>60 months,correspondingto46.7%(n=56)ofparticipants, fol-lowedbyparticipantsintherangefrom>12to≤60months (33.3%,n=40).Regardingthecharacteroftheintestinalstoma, 67.5%(n=81),hadadefinitiveostomy.Withregardto comor-bidities,56.7%(n=68)sufferedfromhypertensionand34.1% (n=41)ofdiabetesmellitus.Inaddition,43.3%(n=52)ofthe respondentsweresmokers.Withregardtooutpatient moni-toringandreceiptofequipment,99.1%(n=119)aremonitored and93.3%(n=112)arereceivingequipment.
Theresults in Table 3showed astatistically significant difference in mean scores for the domains: physical, psy-chological, social relationships and environment, and for the quality of life in general, with statistical significance (p<0.0001).
Theresultsoftheinterviewshavecreatedthreecategories, namely:Complicationswiththestoma,Self-careand Compre-hensivehealthcare,whosepresentationisinTable4.
Table3–Meanscoresofdomainsandqualityoflifeof WHOQOL-brefofstomizedoncologicalpeople(Brasilia, theFederalDistrict,Brazil,2015).
Stomizedoncologicalgroup
Domains n Mean SD CI95% P
Physical 120 12.06 2.48 11.61–12.5 <0.0001 Psychological 120 12.40 2.94 11.87–12.93 <0.0001 Socialrelationship 120 12.64 2.97 12.10–13.18 <0.0001 Environment 120 12.22 2.43 11.78–12.66 <0.0001 GeneralQV 120 12.26 2.28 11.85–12.67 <0.0001
Discussion
Themeanagewas58.72±12.56years.Thisresultis compa-rabletothosefoundinotherstudiesindicatingprevalenceof colorectalcancerinthoseagedover50,notingthatmorethan 90%ofthesecancersoccurinpeopleagedover50years.4,5
Theresultspointedtoapredominanceoffemales,which agreeswithstudiesconductedbytheNationalCancer Insti-tuteinBrazilin2014,beingalsoconsideredvalidfortheyear 2015.Thisreportpointedtotheemergenceof14,180newcases ofcolorectalcancerinmenand15,960newcasesinwomen.12 It was observed that the prevailing religions were the Catholic profession, 56.7% (n=68), followed by evangelical cults,30.9%(n=37).ThisfindingisareflectionofBrazilian reli-giosity,asBrazilisthelargestCatholiccountryintheworld. Religiouspracticeinthepresenceofdiseasemayleadto spir-itualgrowth,asitbringstothepersons’mindtheirfragility andtheproximitytohumanfinitude.5,13
Regardingthevariable“maritalstatus,”ourstudyshowed that62.5%(n=75)ofpatientsweremarriedand10.8%(n=13)
Table4–Categorizationofinterviewsofstomized oncologicalpeople(Brasilia,theFederalDistrict,Brazil, 2015).
Complicationswiththestoma
“Ihadalotofirritationonmyskin[...].”(I1).
“OhmyGod,nowwiththehernia,thestomaismoretotheside[...]do
youunderstand?(sic),itismoreprominent.”(I2). “Ihavealwaysdermatitisinmystoma.”(I3).
“Mystomaisalmostalwaysfullwithcomplications[...]”(I4)
Self-care
”It’sverycomplicatedtohandlethisbag[...]”(I5)
“Atfirstitwasverydifficult,mywifehelpedmetochangethebag,I alwaysdependedonher;nowIcleanandexchangethebag,butstill feelsomedifficulty.”[...]“(I6)
“WhenIhadtoexchangethebag,Ifoundmyselfunclean,feltsick, angry,thesmellmademesick,Icriedalot[...]”(I7)(I7)
Comprehensivehealthcare
“Theoutpatientnurseguidesmehowtotakecareofthebag,andithelps me[...]”(I8)
“Nodoubt(sic),themonitoringbyaprofessionalwouldmakememore confidenttohandlethebag.”(I9)
“Idon’thaveadifferentmedicalappointment,I’mjustgoingtothe outpatientclinictopickupthebags”(I10)
“Ifeltalotofpainatthebeginningandalotofdoubtswiththebag, andIdidnothaveaprofessionaltohelpme[...]”(I11)
were in stable relationships. International and Brazilian studies whichincluded stomizedpersons duetocolorectal neoplasia,suggestthat mostpeople weremarried orliving withapartner.3–5,14,15 Thisknowledgeisimportantbecause, regardlessofmaritalclassification,thestatusofbeingmarried isaprotectivefactorforpeople,sincemarriedpeopleenjoy higherlevelsofphysicalandpsychologicalwell-beingversus singleindividuals,orseparatedordivorcedpeople.5,16,17
Regardingeducationandfamilyincome,itwasobserved thatthegroupconsistedofpeoplewithlowformaleducation: 46.7% (n=56) had onlycomplete or incomplete elementary schooleducation,whichrestrictstheiropportunitiesof inser-tionintheworkmarketandreflectsthelowwagesreceived (mean,2.25minimumwages).Thissituationemphasizesthe importanceofgovernmentassistance tothis populationof patientsandmayalsorepresentimpedimentsforthe preven-tionofcolorectalcancer.Inaddition, thelevel ofschooling interfereswithqualityoflife.4,5
Withrespecttothevariable“Situationinthefaceofwork,” therewasaprevalenceof65.8%(n=79)ofretireesandof17.5% (n=21)ofsubjectswithdrawnfromthelabormarketbythe National InstituteofSocialInsurance, Brazil.Ahigher per-centageofretireesamongpeoplewithpermanentostomyand olderthan60yearswasnoted,sincethatstomizedpeopleare consideredashavingspecialneeds,accordingtoDecreeNo. 5296ofDecember2,2004.4,5
Withregardtothevariable“characteroftheostomy,”a pre-ponderanceofpermanentostomy,67.5%(n=81)wasnoted. Thus,the bowel ostomysurgerydue toacolorectalcancer causesa numberofadaptationsasaresultofthechanges inthe patient’slife,withinterferencehis/herqualityoflife indifferentdimensions–physical,psychological,social rela-tions,andtheenvironment–regardlessofthetemporaryor permanentcharacterofthestoma.3,5,18
Regardingcomorbidities,theresultsindicatedthat34.1% (n=41)ofrespondentshaddiabetestypeII,whichisan impor-tantriskfactorforcolorectalcancer,becauseofthestateof hyperinsulinemiathatcharacterizestheearlystagesofthis neoplasm.Inthecaseofhighbloodpressure,itwasfoundthat 56.7%(n=68)ofparticipantswerehypertensive.The associa-tionofthesediseasescontributestothehighriskofdeveloping colorectalcancer.5,19–21
Theresults indicated that 43.3% (n=52) ofrespondents weresmokers.Althoughthecolonenvironmentisnotdirectly affected bythetobacco composition, thecarcinogenic sub-stancescarried bythe bloodstream haveanegativeimpact withrespecttotheriskofdevelopingacolorectalcancer.5,22
Despitethehighnumberofparticipantswithoutpatient follow-up,99.1%(n=119),andofthosereceivingequipment, 93.3%(n=112),inoursample,thisstudyrevealedthata con-tingent ofstomized oncological people does notenjoy the benefitsofacomprehensivehealthcare.
Themean scoresfor domainsand quality oflifeofthe WHOQOL-bref(Table3)enabletheverificationofstatistically significantdifferencesinmeanscoresforphysical, psycholog-ical,socialrelations,andenvironmentdomains,aswellasfor qualityoflifeingeneral.Thus,studieshavereportedonthe qualityoflifeinstomizedoncologicalpatients,showingthat themakingofanostomyresultsinchangesofthephysical body;andthatthesufferinginthefaceofthenewlifestyle
affectsthephysicalandpsychologicalaspects,aswellasthe socialrelationsandtheenvironment,compromisingthe qual-ityoflifeoftheseindividuals.3,5,6
Inthe“Complicationswiththestoma”category,reportswere identified from participants concerningcomplicationswith thestoma.Livingwithabowelostomyrequiresthatitsuser adoptseveralmeasuresofadaptationandadjustmenttodaily activities,includinglearningcareactionstargetedtohis/her ostomy andtotheperistomalskin,aswell asthe handling ofthecollectorequipment,inordertoavoidfuture complica-tionswiththeintestinalstoma.4,23
Theliteraturestatesthatthecareforcleaningand replace-mentofthecollectorequipmentareveryimportant,asaway to ensure the integrity ofthe skinand preventthe occur-renceofinfection.Toensurethatthesemeasuresarecarried outproperly,itiscriticalthatthestomizedpersonisguided byhealthprofessionals,sothathe/shecanassumethe self-care.4,23 Furthermore, dermatitis are considered the most commoncomplicationofanintestinalOstomy,asgenerallyits occurrenceistheresultofaninappropriateuseofthecollector device.4
In the“Self-care”category, stomizedoncologicalsubjects reportedthat,amongthedifficulties,liestheself-care. Consid-eringthisaspect,acomprehensivehealthassistanceisvitally important,particularlyinrelationtoostomyself-care.The cor-rect orientationon theexchangetechniqueofthecollector equipment,aswellasontheobservationofostomyduring theexchange,highlightstheimportanceofthehealth profes-sionalinhelpingtopreventcomplications,andalsotomake moremanageablethelifewiththestoma.4,24
Finally, inthe “Integralhealth assistance”category,several testimonies ofthe stomizedsubjectsrevealedthe lackofa comprehensivecare.Withthatinmind,thecomprehensive caregoesbeyondthehierarchicalandregionalized organiza-tionalframeworkofhealthcare,thatis,itextendsthroughthe realqualityofanindividualandcollectiveattention,afforded toallusersofthehealthsystem,andreinforcesthe commit-menttothecontinuouslearningandtothemultidisciplinary practice.1,5
However, the activities of the multidisciplinary team shouldbebasedontheholisticassessmentoftheindividual, sothatthepatientreceivesacomprehensive,individualized andsystematizedcare,alsofocusedonthesubjectiveaspects relatedtothesocialrepresentationoftheirnewlifestyle.5
Thus, itisunderstood that, toachievethe integralityin the care ofstomized oncologicalpeople, the user must be regarded asahistorical, socialand politicalsubject, articu-latedtohis/herfamilycontext,totheenvironmentandtothe societyinwhichhe/sheisinserted.
Conclusions
thattheymayhavetofacethroughoutthisdifficultadaptive process.
Therefore,itisevidenttheneedtorealizetheintegralityas aprincipleatvariouslevelsofdiscussionandpracticeofcare, basedonanewparadigm,withprofessionalsreadytolisten andunderstandand,fromthereon,toacceptthedemands andneedsofstomizedoncologicalpeople.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. MachadoMFAS,MonteiroEMLM,QueirozDT,VieiraNFC,
BarrosoMGT.Integralidade,formac¸ãodesaúde,educac¸ãoem
saúdeeaspropostasdoSUS–umarevisãoconceitual.
CiênciaSaúdeColetiva.2007;12(2):335–42.
2. ViegasSMF,PennaCMM.Aconstruc¸ãodaintegralidadeno
trabalhocotidianodaequipesaúdedafamília.EscAnnaNery.
2011;17:133–41.
3. KimuraCA,KamadaI,GuilhemD,MonteiroPS.Qualityoflife
analysisinostomizedcolorectalcancerpatients.J
Coloproctol.2013;33(4):216–21.
4. KimuraCA.Qualidadedevidadepacientesoncológicos estomizados.149f.Dissertac¸ão(MestradoemEnfermagem)– UniversidadedeBrasilia.2013.
5. KimuraCA,KamadaI,JesusCAC,GuilhemDB.Qualityoflife
ofcolorectalcancerpatientswithintestinalstomas.J
CarcinogenMutagen.2014;(5):1–7.
6. BaldwinCM,GrantMRN,WendelC,HornbrookMC,Herrinton
LJ,McMullenC,etal.Genderdifferencesinsleepdisruption
andfatigueonqualityoflifeamongpersonswithostomies.J
ClinSleepMed.2009;5(4):335–43.
7. KimuraCA,KamadaI,GuilhemD,FortesRC.Perceptionof
sexualactivitiesandthecareprocessinostomizedwomen.J
Coloproctol.2013;33(3):145–50.
8. RamirezM,McMullenC,GrantM,AltschulerA,Hornbrook
MC,KrouseRS.Figuringoutsexinareconfiguredbody.
Experiencesoffemalecolorectalcancersurvivorswith
ostomies.WomenHealth.2009;49(8):608–24.
9. Bardin,L.Análisedeconteúdo.Lisboa:Edic¸ões70,2008. 10.BrazilMinistryofHeatlh.NationalHealthCouncil.Resolution
N.466/2012.Guidelinesandregulingnormsforresearch
involvinghumansubjects.Brasilia:CNS;2012.Availableat:
http://conselho.saude.gov.br/resolucoes/1996/Res196en.pdf.
11.FleckMPA,LouzadaS,XavierM,ChachamovichE,VieiraG,
SantosL,etal.Aplicac¸ãodaversãoemportuguêsdo
instrumentoabreviadodeavaliac¸ãodaqualidadedevida
WHOQOL-bref.RevSaúdePública.2000;34(2):178–83.
12.MinistériodaSaúde(BR).SecretariadeAtenc¸ãoàSaúde.
InstitutoNacionaldeCâncer.Estimativas2014:incidênciade
câncernoBrasil.RiodeJaneiro:INCA;2014.
13.SaadM,NasriF.Gruposdereligiosidadeeespiritualidade.In:
KnobelE(Org),editor.PsicologiaeHumanizac¸ão:Assistênciaa
pacientesgraves.SãoPaulo:Atheneu;2008.p.349–59.
14.MohlerMJ,CoonsSJ,HornbrookMC,HerintonLJ,WendelCS,
GrantN,etal.Thehealth-relatedqualityoflifeinlong-term
colorectalcancersurvivorsstudy:objectives,methods,and
patientsample.CurrMedResOpin.2008;24(7):2059–70.
15.SchneiderEC,MalinJL,KahnKL,KoCY,AdamsJ,EpsteinAM.
Survivingcolorectalcancer:patient-reportedsymptom4
yearsafterdiagnosis.Cancer.2007;11(9):2075–82.
16.KaufmanG,TaniguchiH.Genderandmaritalhappiness
inlaterlife.JFamIssues.2006;27(1):735–57.
17.HawkinsD,BoothA.Unhappilyeverafter:affectsof
long-term,lowqualitymarriagesonwell-being.SocialForces.
2005;84(1):451–75.
18.DabirianA,YaghmaeiF,RassouliM,TafreshiMZ.Qualityof
lifeinostomypatients:aqualitativestudy.PatientPrefer
Adherence.2011;5:1–5.
19.CascaisAFMV,MartiniJG,AlmeidaPJS.Oimpactodaostomia
noprocessodeviverhumano.TextoContextoEnferm.
2007;16(1):169–77.
20.SeowA,YuanJM,KohWP,LeeHP,YuMC.Diabetesmellitus
andriskofcolorectalcancerintheSingaporeChineseHealth
Study.JNatlCancerInst.2006;98(1):135–8.
21.ChangCK,UlrichCM.Hyperinsulinaemiaand
hyperglycaemia:possibleriskfactorsofcolorectalcancer
amongdiabeticpatients.Diabetologia.2003;46(3):
595–607.
22.StürmerT,GlynnRJ,LeeIM,ChristenWC,HennekensCH.
Lifetimecigarettesmokingandcolorectalcancerincidencein
thePhysicians’HealthStudyI.JNatlCancerInst.
2000;92(14):1178–81.
23.MartinsPF,AlvimNAT.Perspectivaeducativadocuidadode
enfermagemsobreamanutenc¸ãodaestomiadeeliminac¸ão.
Revbrasenferm.2011;64(2):322–7.
24.MeisnerS,LehurPA,MoranB,MartinsL,JemecGB.Peristomal
skincomplicationsarecommon,expensiveanddifficultto
manage:apopulationbasedcostmodelingstudy.PlosOne.