www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Speech
perception
performance
of
subjects
with
type
I
diabetes
mellitus
in
noise
夽
Bárbara
Cristiane
Sordi
Silva
a,
Erika
Barioni
Mantello
a,∗,
Maria
Cristina
Foss
Freitas
b,
Milton
César
Foss
b,
Myriam
de
Lima
Isaac
a,
Adriana
Ribeiro
Tavares
Anastasio
aaUniversidadedeSãoPaulo(USP),FaculdadedeMedicinadeRibeirãoPreto(FMRP),DepartamentodeOftalmologia,
OtorrinolaringologiaeCirurgiadeCabec¸aePescoc¸o,RibeirãoPreto,SP,Brazil
bUniversidadedeSãoPaulo(USP),FaculdadedeMedicinadeRibeirãoPreto(FMRP),DivisõesdeEndocrinologiaeMetabologiae
Nutric¸ão,RibeirãoPreto,SP,Brazil
Received5May2016;accepted17July2016 Availableonline9August2016
KEYWORDS
Type1diabetes mellitus;
Speechperception; Hearing;
Auditoryperception
Abstract
Introduction:Diabetes mellitus(DM) isa chronicmetabolic disorderofvarious origins that occurswhenthepancreasfailstoproduceinsulininsufficientquantitiesorwhentheorganism failstorespondtothishormoneinanefficientmanner.
Objective:ToevaluatethespeechrecognitioninsubjectswithtypeIdiabetesmellitus(DMI) inquietandincompetitivenoise.
Methods:Itwasadescriptive,observationalandcross-sectionstudy.Weincluded40 partici-pantsofbothgendersaged18---30years,dividedintoacontrolgroup(CG)of20healthysubjects withnocomplaintsorauditorychanges,pairedforageandgenderwiththestudygroup, consist-ingof20subjectswithadiagnosisofDMI.First,weappliedbasicaudiologicalevaluations(pure toneaudiometry,speechaudiometryandimmittanceaudiometry)forallsubjects;afterthese evaluations,weappliedSentenceRecognitionThresholdinQuiet(SRTQ)andSentence Recog-nitionThresholdinNoise(SRTN)infreefield,usingtheListofSentencesinPortuguesetest.
Results:Allsubjectsshowednormalbilateralpuretonethreshold,compatiblespeech audiom-etry and ‘‘A’’ tympanometry curve. Group comparison revealed a statistically significant differenceforSRTQ(p=0.0001),SRTN(p<0.0001)andthesignal-to-noiseratio(p<0.0001).
Conclusion:TheperformanceofDMI subjectsinSRTQandSRTN wasworsecomparedtothe subjectswithoutdiabetes.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
夽 Pleasecitethisarticleas:SilvaBC,MantelloEB,FreitasMC,FossMC,IsaacML,AnastasioAR.Speechperceptionperformanceinsubjects
withtypeIdiabetesmellitusinnoise.BrazJOtorhinolaryngol.2017;83:574---9.
∗Correspondingauthor.
E-mail:[email protected](E.B.Mantello).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.07.003
PALAVRAS-CHAVE Diabetesmellitus
tipoI;
Percepc¸ãodefala; Audic¸ão;
Percepc¸ãoauditiva
Desempenhodapercepc¸ãodefalanoruídoemindivíduoscomdiabetes mellitus tipoI
Resumo
Introduc¸ão: Odiabetesmellitus(DM)eumdisturbiometabolicocronicodevariasorigens,que ocorrequandoopancreasdeixadeproduzir insulinaemquantidadesuficiente ouquandoo organismonaoconsegueresponderaessehormoniodemaneiraeficiente.
Objetivo: AvaliaroreconhecimentodefalaemindividuoscomdiabetesmellitustipoI(DMI) nosilencioenoruidocompetitivo.
Método: Estudodescritivo, observacionaletransversal.Foramincluidos 40participantesde ambos os sexos entre18 e 30 anos, divididosem um grupocontrole (GC)de20 individuos saudaveissemqueixasoualterac¸oesauditivas,pareadosporidadeesexocomogrupodeestudo, compostopor 20 individuoscom diagnosticode DMI. Inicialmenteaplicou-seuma avaliac¸ao audiologica(audiometriatonal,logoaudiometriaeimitanciometria)paratodososindividuos;a seguir,osmesmosforamavaliadosparaoLimiardeReconhecimentodeSentenc¸asnoSilencio (LRSS)eLimiardeReconhecimentodeSentenc¸asnoRuido(LRSR),emcampolivre,pormeio dotesteListadeSentenc¸asemPortugues.
Resultados: Todos os participantes apresentaram audiometria tonal dentro dos padroesde normalidade bilateralmente, logoaudiometria compativel e curva timpanometrica do tipo A. A comparac¸aodos grupos revelouumadiferenc¸a estatisticamentesignificantepara LRSS (p=0,0001),LRSR(p<0,0001)earelac¸aosinal-ruido(p<0,0001).
Conclusões: OdesempenhodosindividuoscomDMIparaLRSSeLRSRfoipioremcomparac¸ao comosindividuossemdiabetes.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Diabetesmellitus(DM)isachronicmetabolicdisorderof var-iousoriginsthatbeginswhenthepancreasfailstoproduce insulininsufficientquantitiesorwhentheorganismfailsto respondtothishormoneinanefficientmanner.Thisleads toaconditioncharacterizedbyhyperglycemia,whichmay damagecertainorgans,especiallytheeyes,kidneys,nerves, heart,andbloodvessels.1,2
One of the less explored or reported consequences for patients with diabetes is dysfunction of the auditory system.3PatientswithDMIdonotsecreteendogenousinsulin or do so in a reduced manner due to the destruction of their pancreatic beta-cells. This situation affects about 20% of casesand is morecommonly identified inchildren and adolescents.2 In Brazil thereare nostudies reporting the exactprevalence of chronic complications in diabetic patients, such as retinopathy, nephropathy, neuropathy, arterialhypertension,cardiovascularchanges,and otoneu-rologic symptoms such as tinnitus, vertigo and hearing loss.4---6Thismaybeduetotwoparticularfactors:affected personsbeingunawareoftheirdiseases,andthefactthat, althoughawareoftheirchronicmetabolicdisorders,several affectedindividualsdonotseekformedicalcare.4
Somestudies haveaimedtodeterminetherelationship betweenDMandhearingloss,butthereisnoconsensusin theinternationalliteratureaboutthecorrelationbetween thesetwoconditions.Nodefinitecause---effectrelationship has been confirmed between diabetes and deafness, and controversiesregardingtheaudiologicaland histopatholog-icalfindingsattributedtodiabetesstillremain.2,3,7---9
Changesinthehearingfunctionofdiabeticpatientshave beenidentifiedthroughaudiometryevaluations,7---10through otoacousticemissions,11---14andthroughbrainstemauditory evoked potentials.8,12,13,15---17 Several studies have investi-gatedthemechanismbywhichchangesinglucoseandinsulin mayproducechangesinhearingperceptionandvestibular function.Labyrinthinestructures,especiallythestria vascu-laris,areknowntobeextremelymetabolicallyactive,and thus are susceptible to oxygen and glucose levels and to theavailabilityofadenosinetriphosphate,necessaryforthe preservationof the endocochlearpotential.Thus,glucose metabolismsignificantlyinfluencesthenormalperformance of the inner ear considering that both hypoglycemia and hyperglycemiacouldimpairitsaverageperformance.18,19
Todaythereisnoconsensusintheinternationalliterature concerningtheetiopathogenesisofhearinglossindiabetics. Someinvestigatorshave arguedthat hearingchangesmay occurbecauseofneuropathywhileothershaveclaimedthey occurduetoangiopathy.Someinvestigationsalsocombine thetwocauses.7---13,15---19
Itshouldalsobepointedoutthatevensubjectswith nor-malhearingasmeasuredbypuretoneandspeechinquiet testsmayhaveimpairedspeechrecognitioninsituationsof adversesignal-to-noise(S/N)ratios.21,22
Testsofsentencerecognitioninquietandinnoiseallow more direct measurements for subjects’ communication abilities,23---25 thusrepresenting valuableaudiological eval-uationtoolsfortheanalysisofhearingabilitiesinsituations similartodailyauditoryexperiences.26---28
Thisstudyaimedtoevaluatespeechrecognitionin sub-jectswithtypeIDMinquietandincompetitivenoise.
Methods
The study was approved by the Ethics Committee of the involved institution (protocol number 12609/2012). The applicationoftheaudiologicalexaminationslasted,on aver-age,1hand30minandwasconcludedonasingleday.
Patients
Thiswasadescriptive,observationalandcross-sectionstudy conductedwith40individualsofboth gendersaged18---30 years.Theparticipantsweredividedintotwogroups: con-trolgroup (CG), 20 healthy young adultswith nohearing complaintsorchanges,andnosystemicdiseases;andstudy group (SG), 20 patients with a diagnosis of type I DM, matchedtothecontrolgroupforageandgender.
The CG was recruited through posters hanging on the walls of the MedicalSchool and throughinvitations made to the persons accompanying the patients, while the SG subjectswererecruitedat theEndocrinologyClinicofthe involvedinstitution.
The exclusion criteriafor both groups were:history of continuedexposuretohighlevelsofsoundpressure,history ofrepeatedand/or chronic otitismedia,otologic surgery, temporal bone trauma, prolonged use of ototoxic drugs, conductive,mixedor sensorineuralhearinglossofmild to profounddegree.
Materialandprocedures
All participants were first submitted to clinical interview and inspection of the ear canal, followed by basic audi-ological evaluation consisting of pure tone audiometry (PTA)(250---8000Hz),speechaudiometry(SpeechReception Threshold ---SRT andthe SpeechRecognition Index--- SRI) andacousticimmittancemeasures.Speechaudiometrywas carriedoutwiththesubjectswearingheadphones.29 Immit-tanceaudiometrywasperformedtoexcludeanymiddleear pathology.
Allprocedureswerecarriedoutinanaudiometricbooth usingatwo-channeldigitalaudiometermodelAC40 (Inter-acoustics), headphones (TDH39P, Telephonics®), and an
amplificationsystemforfreefieldaudiometry,110/220Volts AC current, 50---60Hz, box power of 100Watts each. The acousticimmittancemeasureswerecarriedoutbyOtoflex 100(GNResound)with3AInsertEarphone.
Afterthebasic audiological evaluation,weappliedthe List of Sentences in Portuguese test (LSP).This test
con-sists of a list of 25 sentences in Brazilian Portuguese (List 1A), seven lists of 10 sentences each (1B---7B), and speech-spectrumnoise.28Thesentencesandthenoisewere recorded in independentchannels ona compact diskand wereplayedinaDigitalPanasonicCDPlayer,modelSL-SX430 coupledtothe audiometer. A digital soundpressure level meterinstrument,InstruthermmodelDEC-420,wasusedto determinethesoundpressurelevel(SPL)ofthesentences andfreefieldnoise.Toestablishtheparametersfor calibra-tionof thephrasechannel, we usedthepure toneof the firstCDtrack,inchanneloneasreference.Asforthenoise reference,asitisacontinuoussound,thenoiseitselfwas usedforcalibration.Theoutputof eachchannelwas cali-bratedusingtheVU-meteroftheaudiometer,withboththe puretone(channel1)andthenoise(channel2)setatzero level.
The LSPtest wasapplied infree fieldin an audiomet-ricboothwiththeparticipantpositionedata1-mdistance fromthesoundsourceat0◦azimuth,withnodislocationon thehorizontalorverticalplane.Thesubjectwasinstructed to repeateach sentence exactly ashe or she understood immediatelyafterthepresentation.First,thesubjectwas trainedtobecomefamiliarwiththetestanditsdynamics. Thedatacollectedinthistrainingphasewasnotconsidered intheanalysisoftheresults.
Inthetest phase,theresponsewasconsideredcorrect whenthesubjectwasabletorepeatthepresentedsentence infull,withnoerrorsoromissions.Thus,whentheanswer wascorrect,theintensityofthesentencewasreducedby 4dB.Theuseof4dBintervalsisrecommendedforthe pre-sentation of the stimuliuntil the firstchange in the type ofresponseoccurs,andthen2dBintervalsuntiltheendof thelist.Thisprocedurewasfollowedforthemeasurements inquiet (List1B)andinnoise(List 2B),andthe presenta-tionlevelsofeachsentencewererecorded.Thefinalresult ofthetestisrepresentedbythemeanvalueofthe inten-sitylevelsofthesentencepresentation,calculatedfromthe degreeofperformancethatoccurredatthefirstchangein thetypeofresponsetothelevelofpresentationofthelast sentence onthe list.The signal tonoise ratio (S/Nratio) wasobtainedbysubtractingthestandardoftheintensityof noisepresent(fixedat65dBHL)fromthemeanintensityof sentencepresentation.Thus,theS/Nratiocorrespondedto thedifferenceindBbetweenthespeechrecognition thresh-old test in noise (SRTN) value and the competitive noise value. The S/N ratiowasidentified asthe level at which the subject was able torecognize about 50% of the sen-tencespresented.Differentlistsusedwiththeintentionof eliminatingthepossibilityofa betterperformancedueto sentencememorization.28
Statisticalanalysis
The mean audiometric thresholds were analyzed accord-ing tothe band frequencies, i.e. L1(250Hz to1kHz), L2 (2---4kHz) and L3 (6---8kHz). Analysis of variance (ANOVA) with repeatedmeasures wasused to compare the audio-metricthresholds,thespeechreceptionthresholdsandthe speechrecognitionindexbetweenthetwogroups.
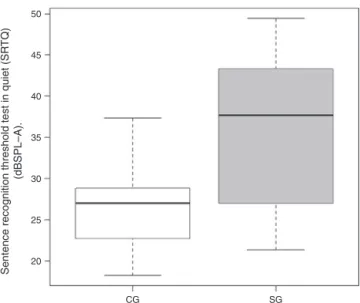
Thresh-50
Sentence recognition threshold test in quiet (SR
TQ)
(dBSPL–A).
45
40
35
30
25
20
CG SG
Figure1 Comparison ofSRTQ resultsbetween CG andSG. Note:Controlgroup(CG),studygroup(SG).
oldTestinQuiet(SRTQ),andSRTNvalues,andtheStudent’s
t-testforindependentdatausedforintergroupcomparison ofmeanSRTQandSRTNvalues.Thelevelofsignificanceset at5%forallanalyses.
Results
Atotalof40participants,aged18---30years(23years aver-age) were evaluated: 20 type 1 diabetics and 20 healthy controlgroup,matchedforageandgender.Thedurationof thediseasewas<5yearsin15%,5---15yearsin55%and>15 yearsin30%thepatients,respectively.
All participants had normal bilateral audiometric thresholds.29 Whentheaudiometricthresholds,thespeech receptionthresholdsandthespeechrecognitionindexwere comparedbetweentherightandleftearsofthetwogroups, therewasnoevidenceofastatisticallysignificantdifference (ANOVA),whichallowedpoolingtheresultsforeachearinto asinglesample.
There was no significant difference in audiometric thresholds according to band frequency between the two groups (250Hz to 1kHz, p=0.12; 2---4kHz, p=0.79; and 6---8kHz,p=0.89).
Thespeechaudiometrytestswerecompatiblewithpure tone threshold,an expected resultsinceboth groups had normalhearingacuity.29
AllparticipantshadatypeAtympanometrycurve indi-catingnormalmobilityofthetympanic-ossicularsystem.30
Mean SRTQ, SRTN and S/N ratio were 25.79, 49.03 and −15.96dBHL for CG subjects and 35.69, 62.62 and −2.38dBHLforSGsubjects,respectively.
Comparison of mean SRTQ and SRTN values revealed a significant difference between CG and SG subjects (Figs.1and2).
ComparisonoftheS/Nratiorevealedasignificant differ-ence(p<0.0001)betweenCGandSGsubjects(Fig.3).
IntragroupcomparisonofmeanSRTQandSRTNthrough Studentt-testrevealedasignificantdifference(p<0.0001) forallparticipants(n=80ears).
Sentence recognition threshold test in noise
(SR
TN) (dBSPL–A).
70
60
50
40
30
CG SG
Figure 2 Comparison of mean SRTN between CG and SG. Note:Controlgroup(CG),studygroup(SG).
0
–10
Signal/Noise r
atio (S/N) (dBSPL–A)
–20
–30
CG SG
Figure3 ComparisonofS/NratiosbetweenCGandSG.Note: Controlgroup(CG),studygroup(SG).
Discussion
Currently,thereisnoconsensusinthespecializedliterature fromtheaudiologicalandhistopathologicalviewpoint con-cerningthecorrelation ofDMwithhearingloss,i.e. there is no sufficient scientific evidence characterizing a clear cause---effectrelationship.
Severalstudieshaveinvestigatedwhetherthereis hear-inglossinherenttoDMandwhichfactorscanbeassociated withthisloss.Thestudiesarecontroversialandhighly vari-ableregardingtheincidenceofhearinglossinpatientswith diabetes.5
In the present study,therewas nodifferencein mean tonehearingthresholdsbetweendiabeticsubjectsand con-trolgroupsubjects.
In a study on the influence of DMI on the hearing of youngadults,Doricci6appliedpuretoneaudiometry thresh-oldtohealthyanddiabeticsubjectsandfoundastatistically significantincreaseinmeanpuretonethresholdsatall fre-quenciesstudiedindiabeticpatients.
AccordingtoMaia andCampos,5 thedeclineofhearing acuity in elderly diabetic individuals is even higher than wouldbeexpectedfortheirageduetopresbyacusis.
WhenyoungsubjectswithDMI,withshortdurationofthe diseaseandwithoutevidentclinicalhearingmanifestations wereevaluated,theirpuretonethresholdswerefoundtobe significantlyhigherathighfrequenciesandpartiallyhigher atmediumfrequenciescomparedtohealthysubjects.3 Sim-ilarfindingswereobtainedinotherstudies.1---3,5,6
HenriquesandCosta32 warned thatobtainingpuretone thresholdandapplyingtestswithseparatewordsisnot suf-ficient for a more extensive and reliable detection of an individual’scommunicativeability.Therefore,applying sen-tencerecognitiontestsinquietandinnoiseisessentialas theypermittheanalysisofthehearingabilitiesinsituations similartorealdailyhearingexperiences.
We found a statistically significant difference in mean SRTQ,SRTNand S/Nratio betweenthe subjectswithand withoutDMI. Inthe literaturereview,we didnotfindany studiesinvestigatingspeechperceptioninquietandinnoise indiabeticsubjectsusingtheLSPtest.20Thespeech percep-tiontestsappliedtoDMIsubjectsconsistedofmonosyllabic wordsinquietandinnoise.Thespeechperceptionabilityof thesesubjectsreducedforwordsinquietandparticularlyin thepresenceofnoisecomparedtocontrol,with20%lower scores.33 These results confirm the importanceof speech perceptionanalysisincompetitivenoise,andillustratethat theuseofsentencesismoreappropriatethansimplywords, becausethe use of sentencesresemblesthe participants’ dailylisteningexperience.
Thetemporalresolutionhearingabilitiesofsubjectswith DMI may be impaired and may thus explain how these subjects are less able to use relatively rapid periods of quiet within the fluctuating environmental noise in order tounderstandthespeechsignal.33,34Thestatistically signif-icantdifferenceobservedinthesentencerecognitiontests inquiet andin noiseapplied tothe participantswithand withoutDMIintheabsenceofhearingcomplaints,hearing lossorboth,revealsthatimpairmentofspeechperception inbothcontexts(quietandnoise)mayoccurduetochanges inthefunctioningofthecentralauditorysystemasa conse-quenceofDM.Furtherstudiesarenecessarytoinvestigate speechperception withacompetitivemessageindiabetic subjects.
Thedifferenceinsentencerecognitionbetweenthe pres-enceandabsenceofnoisewasalsoobservedinthecontrol group. Young people with typical hearing and no clinical complaintsofdifficultyinunderstandingspeechmayshow impaired speech recognition in situations of adverse S/N ratios.Thisproblemmaybeattributed,inpart,tothe neg-ativeeffectsofnoise onneural synchrony,whichresultin degradedspeechrepresentationatcorticalandsubcortical levels.35
Varioushearingabilitiesarerequiredtoreachthesame degree of speech recognition, demonstrating that more detailedsensoryinformationisnecessaryunderdifficult lis-teningconditions.36Furtherstudiesareneededtoelucidate thepresence of impairmentin theperipheral andcentral auditory system, especially regarding possible damage to speechrecognitionfordifferentlisteningconditionsin dia-beticsubjects.AudiologicfollowupofsubjectswithDMis recommended.
Conclusion
Speechrecognitionperformanceinquietandincompetitive noise wasworse in subjects withtype Idiabetes mellitus comparedtosubjectswithoutdiabetes.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
Fundac¸ão de Amparo à Pesquisa do Estado de São Paulo (FAPESP)Grant:2012/07490---0.
References
1.AmericanDiabetesAssociation.Diagnosisandclassificationof diabetesmellitus.DiabetesCare.2007;30:42---7.
2.AmericanDiabetesAssociation.Diagnosisandclassificationof diabetesmellitus.DiabetesCare.2010;33:62---9.
3.DabrowskiM,Mielnik-NiedzielkaG,NowakowskiA.Involvement oftheauditoryorganintype1diabetesmellitus.JEndocrinol. 2011;2:138---44.
4.GrossJL,NehmeM.Detecc¸ãoetratamentodascomplicac¸ões crônicasdodiabetesmelito:ConsensodaSociedadeBrasileira deDiabeteseConselhoBrasileirodeOftalmologia.RevAssoc MedBras.1999;3:279---84.
5.MaiaCAS,CamposCAH.DiabetesMellituscomocausadeperda auditiva.BrazJOtorhinolaryngol.2005;71:208---14.
6.DoricciGP(Master’sthesis)Achadosaudiológicosemportadores deDiabetesMellitusinsulinodependentes.RibeirãoPreto: Fac-uldade de Medicina de Ribeirão Preto, Universidade de São Paulo;2008.p.106.Dissertac¸ãodemestrado.
7.VirtaniemiJ,LaaksoM,Nuutinen J,KarjalainenS,Vartiainen E.Hearingthresholdsininsulindependentdiabeticpatients.J LaryngolOtol.1994;108:837---41.
8.PessinABB,MartinsRHG,PimentaWDP,SimoesACP,Marsiglia A,AmaralAV,etal.Auditoryevaluationinpatientswithtype1 diabetes.AnnOtolRhinolLaryngol.2008;117:366---70. 9.PudarG,VlaˇskiL,Filipovi´cD,TanackovI.Correlationofhearing
functionfindings inpatientssufferingfrom diabetesmellitus type1inregardtoageandgender.MedPregl.2009;62:395---401. 10.ElaminA,FadlallahM,TuvemoT.Hearinglossinchildrenwith
type1diabetes.IndianPediatr.2005;42:15---21.
11.DiLeoMA,DiNardoW,CerconeS,CiervoA,LoMonacoM,Greco AV,etal.CochleardysfunctioninIDDMpatientswithsubclinical peripheralneuropathy.DiabetesCare.1997;20:824---8. 12.LisowskaG,NamyslowskG,MorawskiK,StrojekK.Early
identi-ficationofhearingimpairmentinpatientswithtype1diabetes mellitus.OtolNeurotol.2001;22:316---20.
13.OttavianiF,DozioN,NegliaCB,RiccioS,ScaviniM.Absenceof otoacousticemissionsininsulin-dependentdiabeticpatients.Is thereevidencefordiabeticcochleopathy?JDiabetesComplic. 2002;16:338---43.
14.HilaliAV,BoultonA.Astudyofotoacousticemissionsintype1 diabetesmellitus.AudiolMed.2003;1:255---60.
15.VirtaniemiJ,LaaksoM,KärjäJ,NuutinenJ,KarjalainenS. Audi-torybrainstemlatenciesintype1(insulin-dependent)diabetic patients.AmJOtolaryngol.1993;14:413---8.
17.Niedzielska G, Katska E. ABR disturbances in children with insulin-dependent diabetes mellitus. Int J Pediatr Otorhino-laryngol.1998;44:1---4.
18.Bittar RSM, Sanchez TG, Santoro PP, Medeiros IRT. O metabolismodaglicoseeoouvidointerno.Arquivos Int Oto-rrinolaringol.1998;1:4---8.
19.LavinskyM,WolffFH,LavinskyL.Estudode100pacientescom clínicasugestivadehipoglicemiaemanifestac¸õesdevertigem, surdezezumbido.BrazJOtorhinolaryngol.2000;7:8---12. 20.RissatoMR,SantosTMM.Limiarestonaisemfrequências
ultra-altasereconhecimentodefaladeportadoresdeperdaauditiva neurossensorial.RevCEFAC.2003;5:279---83.
21.Caporali SA, Silva JA. Reconhecimento de falano ruído em jovenseidososcomperdaauditiva.BrazJOtorhinolaryngol. 2004;70:525---32.
22.BeckerKT, Costa MJ,Lautenschlager L,Tochetto TM,Santos SN.Reconhecimentodefalaemindivíduoscomesemqueixa clínicadedificuldadeparaentenderafalanoruído.Arquivos IntOtorrinolaringol.2011;15:276---82.
23.Plomp R, Mimpen AM. Improving the reliability of testing the speech reception threshold for sentences. Audiology. 1979;18:43---52.
24.HagermanB.Efficiencyofspeechaudiometryandotherstests. BrJAudiol.1993;27:423---5.
25.CerveraT,Gonzalez-AlbernazJ.TestofSpanishsentencesto measurespeechintelligibilityinnoiseconditions.BehavRes. 2011;43:459---67.
26.HenriquesMO, MirandaEC, CostaMJ.Limiares de reconhec-imentode sentenc¸as no ruído, em campo livre: valores de referênciaparaadultosnormo-ouvintes.BrazJ Otorhinolaryn-gol.2008;74:188---92.
27.Henriques MO, Costa MJA. Limiares de reconhecimento de sentenc¸asemindivíduosnormo-ouvintesnapresenc¸aderuído incidente de diferentes ângulos. Rev Soc Bras Fonoaudiol. 2011;16:54---8.
28.Costa MJ. Lista de sentenc¸as em português: apresentac¸ão e estratégiasdeaplicac¸ãonaaudiologia.1998.SantaMaria: Pal-lotti;1998.p.26---36.
29.Santos TMM, Russo ICP. A prática da audiologia clínica. São Paulo:CortezEditora;1986.p.232.
30.JergerJ.Clinicalexperiencewithimpedanceaudiometry.Arch Otolaryngol.1970;92:311---24.
31.Marchiori LLM, Gibrin PCD. Diabetes mellitus: prevalên-cia de alterac¸ões auditivas. Arq Bras Endocrinol Metabol. 2003;47:82---6.
32.Henriques MO, Costa MJ. Reconhecimento de sentenc¸as no ruído,emcampolivre,emindivíduoscomesemperdaauditiva. RevCEFAC.2011;13:1040---7.
33.RanceG,ChisariD,O’HareF,RobertsL,ShawJ,Jandeleit-Dahm K,etal.Auditoryneuropathyinindividualswithtype1diabetes. JNeurol.2014;261:1531---6.
34.ZengFG,Kong YY,MichaelewskiHJ,StarrA.Perceptual con-sequencesofdisruptedauditorynerveactivity.JNeurophysiol. 2005;93:3050---63.
35.Anderson S,SkoeE,ChandrasekaranB, KrausN.Neural tim-ing is linked to speech perception in noise. J Neurosci. 2010;30:4922---6.