Birth cohort differences in the use of medications
in a Brazilian population of older elderly:
the Bambuí Cohort Study of Aging
(1997 and 2008)
Diferenças de coorte por nascimento no uso de
medicamentos em uma população brasileira
de idosos mais velhos: Estudo de Coorte
de Idosos de Bambuí (1997 e 2008)
1 Núcleo de Estudos em Saúde Pública e Envelhecimento, Fundação Oswaldo Cruz/Universidade Federal de Minas Gerais, Belo Horizonte, Brasil.
2 Escola de Enfermagem, Universidade Federal de Minas Gerais, Belo Horizonte, Brasil.
Correspondence A. I. Loyola Filho
Núcleo de Estudos em Saúde Pública e Envelhecimento, Fundação Oswaldo Cruz/ Universidade Federal de Minas Gerais.
Av. Augusto de Lima 1715, 6o andar, Belo Horizonte, MG 30190-003, Brasil. [email protected]
Antônio Ignácio de Loyola Filho 1,2 Josélia O. A. Firmo 1
Elizabeth Uchôa 1
Maria Fernanda Lima-Costa 1
Abstract
This study examined differences in the use of medications in two birth cohorts (born from 1916 to 1926 and from 1927 to 1937) among old-er eldold-erly in the population-based cohort study in Bambuí, Minas Gerais State, Brazil. The study used data on participants who were 71-81 years of age in the baseline survey in 1997 (n = 492) and in the 11th wave, in 2008 (n = 620). The number of medications currently consumed (mean = 4.6 and 3.4, respectively) and prevalence of polyphar-macy (46.6% and 29.1%, respectively) were higher in the more recent cohort as compared to the ear-lier one. These differences were independent of gender, age, schooling, number of medical visits in the previous 12 months, and number of chron-ic conditions. The more recent cohort showed significant differences in the use of psychoactive drugs, lipid modifying agents, drugs for diabetes, and antithrombotic agents, as well as changes in drugs used for arterial hypertension. In general, these changes are consistent with those observed in elderly populations in high-income countries.
Drug Utilization; Aged; Cohort Studies
Introduction
Brazil has experienced a rapid demographic change marked by population aging. From 1970 to 2000, the proportion of elderly (60 years or older) increased from 5.1% to 8.6% 1, reaching
10% by 2009 (Departamento de Informática do SUS. Informações Demográficas. http://tabnet. datasus.gov.br/cgi/tabcgi.exe?ibge/cnv/popuf. def, accessed on 27/Oct/2010). With population aging, chronic health conditions gain greater visibility in the healthcare scenario, due to the increase in their prevalence and the presence of comorbidities 2.
The high prevalence of chronic illnesses among the elderly is associated with high con-sumption of medications by this population group 3. In the elderly population, the risks
as-sociated with consumption of medications com-pete with the expected benefits, due to the physi-ological changes proper to aging, including the decrease in muscle mass and body water, with effects on the pharmacodynamics and pharma-cokinetics of medications. Thus, unwanted ef-fects (adverse efef-fects and drug-drug interactions) are more likely to occur 4.
The prevalence of polypharmacy is high in the elderly 5,6,7, and is one of the strongest
pre-dictors of health problems associated with use of medications 4. Polypharmacy is defined as the
quantita-tive concept, which does not take the pertinence of their utilization into account 8. The
charac-teristics most consistently associated with poly-pharmacy are female gender, more advanced age, chronic illness, and greater utilization of health services 6,7,9. Increasing polypharmacy has been
observed in elderly populations in high-income countries 10,11.
Studies in other countries 12,13,14 and in
Bra-zil 15,16 have identified drugs for the
cardiovas-cular system, central nervous system, metabo-lism, and alimentary tract as the most frequent-ly consumed among the elderfrequent-ly. More recentfrequent-ly, changes in the pattern of use of some drug class-es have been observed in some populations, class- es-pecially in the pattern of consumption of drugs for hypertension 17,18, as well as an increase in
the use of lipid modifying 5,17, psychoactive 19,20,
and antiepileptic drugs 21.
In Brazil, pharmacoepidemiological studies have described the prevalence of polypharmacy and associated factors and the most widely con-sumed drug classes among the elderly popula-tion 7,15,16. However, to our knowledge, no study
has been done on differences over time in drug use patterns in this population.
The current study used data from the baseline (1997) and the 11th wave (2008) from the
Bam-buí Cohort Study of Aging in order to investigate birth cohort differences in polypharmacy and the amounts and classes of drugs used.
Methodology
Study area and population
The Bambuí Cohort Study of Aging has been conducted in the city of the same name (with some 15,000 inhabitants), located in the State of Minas Gerais, in Southeast Brazil. The popu-lation for the baseline cohort was identified through a complete census of the city conducted in November-December 1996. Among the 1,742 residents 60 years or older on January 1, 1997, 1,606 participated in the baseline cohort. Since then, members of cohort have been followed up annually. From 1997 to 2008 (the 11th wave),
641 participants died, and only 6% were lost to follow-up. Further details have been published elsewhere 22,23.
All the participants in the baseline survey and 11th wave and with ages between 71 and 81
years, corresponding to the births in 1916-1926 and 1927-1937, respectively, were selected for the present study.
Data collection and study variables
Information on consumption of medications was obtained through home interviews, with verification of the product package and/or medical prescription. All the medications were identified, broken down according to their ac-tive ingredients, and classified according to the Anatomical Therapeutic Chemical (ATC) Index (World Health Organization Collaborating Cen-tre for Drug Statistics Methodology. ATC/DDD Index 2011. http://www.whocc.no/atc_ddd_in dex/, accessed on Sep/2010). The current study used the classifications corresponding to levels 1 (anatomical) and 2 (therapeutic), considering over-the-counter and prescription drugs. The number of drugs consumed (counting variable) was truncated for the highest values (10 or more). Polypharmacy was defined as the use of five or more drugs 7,24.
The other study variables were gender, age, schooling (0-3 and ≥ 4 complete years), history of medical diagnosis for chronic illnesses (arte-rial hypertension, coronary disease – myocardial infarction and/or angina –, Chagas disease, dia-betes, and arthritis/rheumatism), and number of medical consultations in the previous 12 months. The number of chronic conditions and number of medical consultations were dichotomized (exposure was defined as values greater than the median).
The data collection instruments and proce-dures were the same in the 1997 and 2008 sur-veys. The interviews were conducted by mem-bers of the community with more than 11 years of schooling and who were certified after training by the research team.
Data analysis
Data analysis was based on the Pearson chi-square test (for comparison of frequencies) and the Student t test (for comparison of means). Univariate and multivariate Poisson regression models with robust variance were used to esti-mate prevalence ratios and respective 95% con-fidence intervals (95%CI) to examine the factors associated with use of medications. Gender, age, schooling, number of chronic conditions or ill-nesses, and number of medical consultations in the previous 12 months were considered a priori confounding variables in these analysis, since they had been described previously as fac-tors associated with the use of medications in the underlying population base for the Bambuí co-hort 6,25. All the analyses used Stata, version 10
The Bambuí Cohort Study of Aging was ap-proved by the Ethics Research Committee of the Oswaldo Cruz Foundation (Fundação Oswaldo Cruz), Rio de Janeiro, Brazil 22,23.
Results
All 492 participants in the 1997 survey ranging from 71 to 81 years of age had information on the use of medications and were included in the pres-ent analysis. Of the 657 cohort survivors in 2008 and in the same age bracket, 620 (94.4%) had the corresponding information and were included in this study. Participants and non-participants were similar in relation to gender (p = 0.106), age (p = 0.511), and schooling (p = 0.254).
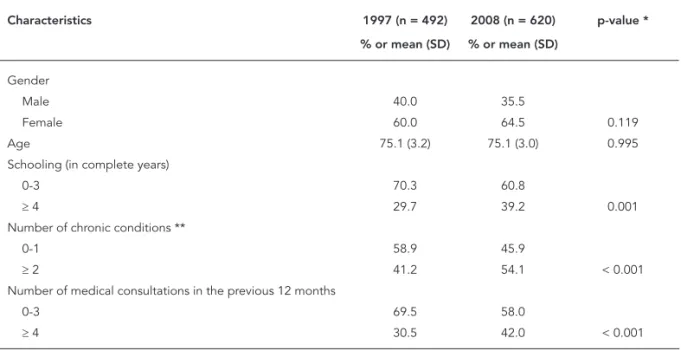
Table 1 shows some characteristics of the study participants in 1997 and 2008. No differ-ences were observed between the two groups in terms of gender (60% and 64.5% were women, respectively) or mean age (75.1 years in both years). From 1997 to 2008, there were significant increases in schooling (29.7% and 39.2% had ≥ 4 years of schooling, respectively), prevalence of two or more chronic illnesses (41.2% and 54.1%, respectively), and number of medical visits in the previous 12 months (30.5% and 42% had four or more medical visits, respectively).
Prevalence of the use of at least one medication (88.8% and 93.6%, respectively), mean number of medications used (3.4 and 4.6, respectively), and prevalence of polypharmacy (29.1% and 46.6%, respectively) were higher in the more recent co-hort as compared to the earlier one, as shown in Table 2. The association between birth cohort and number of medications consumed (PR = 1.19; 95%CI: 1.11-1.28) and prevalence of polyp-harmacy (PR = 1.35; 95%CI: 1.15-1.57) remained even after adjusting for age, gender, schooling, number of medical visits, and number of chronic illnesses. The association between birth cohort and use of at least one medication lost statistical significance after adjusting for these same vari-ables (PR = 1.03; 95%CI: 0.99-1.06).
Table 3 shows the number of medications consumed in each cohort, stratified by gender and age bracket. Significant increases were ob-served in the mean number of medications used in the more recent cohort as compared to the earlier one, both among men (from 2.6 to 3.6) and women (from 3.9 to 5.1). These increases were observed consistently in the 71-75-year age bracket (from 2.0 to 2.7 in men and from 2.8 to 4.1 in women) and the 76-81-year bracket (from 2.5 to 2.9 in men and from 4.0 to 5.2 in women). Overall, the mean number of medications con-sumed was consistently higher among women in both cohorts.
Table 1
Selected characteristics of study participants. The Bambuí Cohort Study of Aging, 1997 and 2008.
Characteristics 1997 (n = 492) 2008 (n = 620) p-value *
% or mean (SD) % or mean (SD)
Gender
Male 40.0 35.5
Female 60.0 64.5 0.119
Age 75.1 (3.2) 75.1 (3.0) 0.995
Schooling (in complete years)
0-3 70.3 60.8
≥ 4 29.7 39.2 0.001
Number of chronic conditions **
0-1 58.9 45.9
≥ 2 41.2 54.1 < 0.001
Number of medical consultations in the previous 12 months
0-3 69.5 58.0
≥ 4 30.5 42.0 < 0.001
SD: standard deviation.
Table 2
Use of medications by older elderly in the earlier cohort (born 1916-1926) and more recent cohort (born 1927-1937). The Bambuí Cohort Study of Aging, 1997 and 2008.
Use of medications Earlier cohort (n = 491)
Recent cohort (n = 620)
Adjusted PR * (95%CI)
Adjusted PR ** (95%CI)
Adjusted PR *** (95%CI)
Adjusted PR #
(95%CI)
Use of at least 1 medication (%) 88.8 93.6 1.05 (1.01-1.09) 1.05 (1.01-1.09) 1.04 (1.00-1.08) 1.03 (0.99-1.06)
Number of medications [mean (SD)] 3.4 (2.5) 4.6 (3.0) 1.31 (1.21-1.41) 1.31 (1.21-1.41) 1.24 (1.15-1.34) 1.19 (1.11-1.28) Polypharmacy ## (%) 29.1 46.6 1.56 (1.33-1.83) 1.58 (1.35-1.85) 1.46 (1.25-1.71) 1.35 (1.15-1.57)
PR (95%CI): prevalence ratio (95% confi dence interval) estimated by multivariate Poisson regression with robust variance. * Adjusted by gender and age;
** Adjusted by gender, age, and schooling;
*** Adjusted by gender, age, schooling, and number of medical consultations;
# Adjusted by gender, age, schooling, number of medical consultations, and number of chronic conditions/illnesses;
## Use of fi ve or more medications.
As shown in Figure 1, the most frequently consumed medications in both cohorts were those acting on the cardiovascular system (57.7% and 80.7%, respectively), followed by the nervous system (52.6% and 63.4%), and alimentary tract and metabolism (43.9% and 44.5%). The use of medications acting on the cardiovascular system (code C), nervous system (code N), and blood and blood forming organs (code B) was signifi-cantly higher in the more recent as compared to the earlier cohort. No statistically significant dif-ferences were observed between the two cohorts in the use of medications for the alimentary tract and metabolism (code A) or for drugs acting on the musculoskeletal system (code M).
As shown in Table 4, the five classes of medi-cations (level 2 therapeutic classification) most widely used by the elderly in the older cohort were, in decreasing order: diuretics (29.1%), vi-tamins (25.6%), cardiac therapy (24.8%), psycho-leptics (22.4%), and analgesics (19.5%). Among individuals from the more recent cohort, the highest prevalence rates were for consumption of agents acting on the renin-angiotensin system (48.2%), diuretics (41.6%), beta blocking agents (35.3%), antithrombotic agents (33.1%), and an-algesics (26.3%).
Differences between the two cohorts (Table 4) also included significant increases in vari-ous medications acting on the cardiovascular
Table 3
Mean number of medications consumed by older elderly in the earlier cohort (born 1916-1926) and more recent cohort (born 1927-1937). The Bambuí Cohort Study of Aging, 1997 and 2008.
Gender/Age bracket (years) Earlier cohort More recent cohort p-value *
Mean (DP) Mean (DP)
Men
71-75 2.4 (2.0) 3.3 (2.7) 0.003
76-81 2.8 (2.6) 4.1 (3.2) 0.003
Women
71-75 3.9 (2.5) 5.0 (2.9) < 0.001
76-81 4.0 (2.3) 5.2 (3.1) < 0.001
All men 2.6 (2.3) 3.6 (2.9) < 0.001
All women 3.9 (2.5) 5.1 (3.0) < 0.001
p-value * < 0.001 < 0.001
Figure 1
Use of medications by older elderly in the earlier cohort (born 1916-1926) and more recent cohort (born 1927-1937), according to level 1 of the Anatomical Therapeutic Chemical (ATC) Index *. The Bambuí Cohort Study
of Aging, 1997 and 2008.
Earlier cohort
More recent cohort 90,0
80,0 70,0 60,0 50,0 40,0 30,0 20,0 10,0 0,0
Alimentary tract and metabolism
Blood Cardiovascular Musculo-skeletal system
Nervous system p = 0.838
p < 0.001
p < 0.001
p < 0.001
p < 0.057
* World Health Organization Collaborating Centre for Drug Statistics Methodology (ATC/DDD Index 2011. http://www.whocc.no/atc_ddd_index/, accessed on Sep/2010).
Table 4
Use of medications by older elderly in the earlier cohort (born 1916-1926) and more recent cohort (born 1927-1937), according to level 2 of the Anatomical Therapeutic Chemical (ATC) Index *. The Bambuí Cohort Study of Aging, 1997 and 2008.
Medications (codes) Earlier cohort More recent cohort PR (95%CI)
% %
Cardiovascular system (C)
Cardiac therapy (C01) 24.8 19.2 0.76 (0.61-0.95)
Antihypertensives (C02) 8.5 6.6 0.76 (0.50-1.14)
Diuretics (C03) 29.1 41.6 1.41 (1.20-1.67)
Beta blocking agents (C07) 6.1 35.3 5.71 (3.97-8.20) Calcium channel blockers(C08) 13.2 18.9 1.40 (1.06-1.84) Agents acting on the renin-angiotensin system (C09) 10.4 48.2 4.61 (3.51-6.06) Lipid modifying agents (C10) 0.8 13.7 16.48 (6.09-44.57) Nervous system (N)
Analgesics (N02) 19.5 26.3 1.33 (1.06-1.65)
Antiepileptics (N03) 6.9 21.6 3.10 (2.17-4.42)
Psycholeptics (N05) 22.4 20.2 0.88 (0.70-1.10)
Psychoanaleptics (N06) 9.6 22.4 2.28 (1.68-3.10)
Alimentary tract and metabolism (A)
Drugs used in diabetes (A10) 6.9 18.4 2.64 (1.83-3.80)
Vitamins (A11) 25.6 12.3 0.47 (0.36-0.61)
Musculo-skeletal system (M)
Antiinflammatory and antirheumatic products (M01) 15.5 12.1 0.76 (0.57-1.02) Blood and blood forming organs (B)
Antithrombotic agents (B01) 17.5 33.1 1.88 (1.51-2.35)
system: lipid modifying agents (PR = 16.48; 95%CI: 6.09-44.57); beta blocking agents (PR = 5.71; 95%CI: 3.97-8.20); agents acting on the renin-angiotensin system (PR = 4.61; 95%CI: 3.51-6.06); diuretics (PR = 1.41; 95%CI: 1.20-1.67), and calcium channel blockers (PR = 1.40; 95%CI: 1.06-1.84); meanwhile, the use of car-diac therapy decreased significantly (PR = 0.76; 95%CI: 0.61-0.95). As for medications acting on the nervous system, there was an increase in the use of antiepileptics, psychoanaleptics, and analgesics, especially in the first two (PR = 3.10; 95%CI: 2.17-4.42 and PR = 2.28; 95%CI: 1.68-3.10, respectively). Medications acting on the alimen-tary tract and metabolism showed an increase in drugs used in diabetes (PR = 2.64; 95%CI: 1.83-3.80) and a decrease in the use of vitamins (PR = 0.47; 95%CI: 0.36-0.61). Finally, the more recent cohort showed an increase over the ear-lier cohort in the use of antithrombotic agents (PR = 1.88; 95%CI: 1.51-2.25).
Discussion
The current study’s findings showed an impor-tant increase in the number of medications con-sumed and in the prevalence of polypharmacy in the more recent cohort as compared to the ear-lier cohort. The association between birth cohort and use of medications was not affected by age, gender, or schooling. Adjustments according to number of medical visits and number of chronic illnesses attenuated these associations, but they still remained statistically significant.
The results are consistent with findings in elderly populations in high-income countries. Studies in Finland and the United States have shown an increase in both the number of medi-cations consumed by the elderly and polyphar-macy 10,11. The explanations for this increase
re-late to socio-cultural and political issues linked to healthcare and technological advances in this area. This includes issues with a greater supply and expanded access to health services, greater participation by medications in healthcare, ex-pansion of the therapeutic armamentarium, changes in treatment approaches, and prescrip-tion habits 10,12, in addition to growing
availabil-ity of over-the-counter drugs 26.
In the current study, women in both cohorts used more medications than men. These find-ings are consistent with previous observations in studies both in Brazil 16 and elsewhere 9,13,14.
Greater use of medications by women can be ex-plained, at least in part, by greater use of health-care services, greater knowledge of medications, quantitative and qualitative differences in
dis-ease patterns, and greater attention to their own health problems 16.
In the current study, the most widely used drug classes (cardiovascular, nervous system, al-imentary tract and metabolism, blood and blood forming organs, and musculoskeletal system) reproduce a consumption pattern observed in elderly populations in different countries 13,14
and in Brazil 15,16. The use of these drug classes
relates to treatment and prevention of typical health events for this phase of life, like hyper-tension, coronary disease, diabetes, and chronic pain.
Considering the therapeutic classification, the study showed important differences be-tween the two cohorts in the medications used for management of hypertension and more spe-cifically, an increase in the use of beta blocking agents, agents acting on the renin-angiotensin system, diuretics, and calcium channel block-ers. The increase in the use of medications is consistent with findings from other studies 17,18
and the prevailing guidelines for treatment of hypertension 27, as well as Brazilian Ministry of
Health (Ministério da Saúde) protocols for re-organization of treatment of hypertension 28.
Importantly, there was an important increase in the use of lipid modifying agents, a trend also present in other populations 5,17, as well as in the
use of antithrombotic agents. Both medications are used to decrease cardiovascular risk 17,29.
Among agents acting on the nervous system, there were important increases in the use of an-tiepileptics and psychoanaleptics in the more re-cent cohort. Rere-cent increases have been observed in the use of antiepileptics in other elderly popu-lations 21,30. The prevalence of epilepsy among
the elderly is relatively low, varying from 1% to 3%
31,32. Thus, it is unlikely that increases in the
inci-dence and/or prevalence of this condition would explain the increase from 7% to 22% in the use of antiepileptics in the current study. It is more likely that these medications are being used for other therapeutic purposes, such as pain relief, prevention of migraine, management of bipolar disorder, or neurological treatment of patients with a history of stroke 21,30. In addition,
stud-ies in high-income countrstud-ies 19,20 have shown an
increase in the use of psychoactive drugs, both psychoanaleptics and psycholeptics 33. The
cur-rent study showed an increase in the use of the former, but not the latter.
was a decrease in the use of vitamins in the more recent cohort as compared to the earlier. Vita-mins are viewed as maintaining overall health 3
and as a source of essential nutrients, and their consumption has decreased in recent years as a result of changes in eating habits 3,35. They are
commonly used in the absence of health prob-lems and without a medical prescription 36 and
concurrently with other prescribed medications, which increases the risk of drug-drug interac-tions 5. Thus, and given the lack of evidence of
the benefits of using such medications to prevent chronic illnesses 37, the decrease in prevalence of
their use, as observed here, can be considered a positive trend.
This study has advantages and limitations. The advantages include its population-based design and the uniformity of its data collection procedures, making the data comparable, in addition to the small losses to follow-up, which reduced the probability of a non-participation bias. The response rate was high in both 1997 and 2008. In the first year, all the participants had information on the use of medications. In 2008, the corresponding response rate was somewhat
lower (94.5%). However, this appears not to have affected the results, since participants and non-participants were similar in terms of age, gender, and schooling. Finally, this study was done in a population of older elderly living in the city of Bambuí, and it may not be possible to generalize the results to other populations. Still, it is impor-tant to highlight that the most imporimpor-tant findings were consistent with those in elderly populations in other countries.
In short, the current study’s findings show important changes in the pattern of medication use in the more recent birth cohort as compared to the earlier one. The main differences were in-creases in the number of medications consumed, polypharmacy, psychoactive drugs, lipid modify-ing drugs, drugs used in diabetes, and antithrom-botic agents, as well as changes in the drugs used to control hypertension. In general, these changes are consistent with findings in elderly populations in high-income countries. Further studies are recommended to examine the ben-efits or disadvantages of these changes for health conditions in the elderly.
Resumo
Foram examinadas diferenças de coorte (entre nasci-dos em 1916-1926 e em 1927-1937) no uso de medica-mentos entre idosos participantes do Estudo de Coorte de Idosos de Bambuí. Foram utilizados dados dos par-ticipantes com 71-81 anos de idade da linha de base em 1997 (n = 492) e do 11o ano de seguimento em 2008
(n = 620). O número de medicamentos consumidos (média = 4,6 e 3,4, respectivamente) e a prevalência da polifarmácia (46,6% e 29,1%, respectivamente) foram mais altos na coorte recente, em comparação à antiga. Essas diferenças foram independentes do sexo, idade, escolaridade, número de consultas médicas e número de doenças crônicas. Na coorte mais jovem, observa-ram-se aumentos significativos no uso de psicofár-macos, agentes modificadores de lipídios, hipoglice-miantes e antitrombóticos, assim como mudanças nos medicamentos utilizados para o controle da hiperten-são arterial. De maneira geral, essas mudanças hiperten-são consistentes com o observado em populações idosas de países de alta renda.
Uso de Medicamentos; Idoso; Estudos de Coortes
Contributors
A. I. Loyola Filho conceived the project, was responsi-ble for the data analysis and interpretation, drafted the article, and approved the final version. J. O. A. Firmo participated in the data collection, interpretation of the results, and critical analysis of the article. E. Uchôa and M. F. Lima-Costa collaborated in the project’s conceptu-alization, data collection, critical revision of the article, and approval of the final version.
Acknowledgments
References
1. Carvalho JAM, Garcia RA. O envelhecimento da população brasileira: um enfoque demográfico. Cad Saúde Pública 2003; 19:725-33.
2. Wolff JL, Starfield B, Anderson G. Prevalence, ex-penditures, and complications of multiple chronic conditions in the elderly. Arch Intern Med 2002; 162:2269-76.
3. Kaufman DW, Kelly JP, Rosenberg L, Anderson TE, Mitchell AA. Recent patterns of medication use in the ambulatory adult population of the United States. JAMA 2002; 287:337-44.
4. Tamblyn R. Medication use in seniors: challenges and solutions. Therapie 1996; 51:269-82.
5. Qato DM, Alexander GC, Conti BM, Johnson M, Schumm P, Lindau ST. Use of prescription and over-the-counter medications and dietary supple-ments among older adults in the United States. JAMA 2010; 300:2867-78.
6. Loyola Filho AI, Uchôa E, Firmo JOA, Lima-Costa MF. Influência da renda na associação entre dis-função cognitiva e polifarmácia: Projeto Bambuí. Rev Saúde Pública 2008; 42:89-99.
7. Rozenfeld S, Fonseca MJM, Acúrcio FA. Drug uti-lization and polypharmacy among the elderly: a survey in Rio de Janeiro city, Brazil. Rev Panam Sa-lud Pública 2008; 23:34-43.
8. Rollason V, Vogt N. Reduction of polypharmacy in the elderly: a systematic review of the role of the pharmacist. Drugs Aging 2003; 11:817-32.
9. Veehof L, Stewart R, Haaijer-Ruskamp F, Jong BM. The development of polyparmacy. A longitudinal study. Fam Pract 2000; 17:261-7.
10. Jylhä M. Ten-year change in the use of medical drugs among the elderly: a longitudinal study and cohort comparison. J Clin Epidemiol 1994; 47: 69-79.
11. Stewart RB, Moore MT, May FE, Marks RG, Hale WE. Changing patterns of therapeutic agents in the elderly: a ten-year overview. Age Ageing 1991; 20:182-8.
12. Linjakumpu T, Hartikainen S, Klaukka T, Veijola J, Kivelä SL, Isoaho R. Use of medications and polyp-harmacy are increasing among the elderly. J Clin Epidemiol 2002; 55:809-17.
13. Chen YF, Dewey ME, Avery AJ; Analysis Group of The MRCCFA Study; The Medical Research Council Cognitive Function and Ageing Study (MRC CFAS). Sel-reported medication use for old-er people in England and Wales. J Clin Pharm Thold-er 2001; 26:129-40.
14. Stewart RB, Moore MT, May FE, Marks RG, Hale WE. A longitudinal evaluation of drug use in an ambulatory elderly population. J Clin Epidemiol 1991; 44:1353-9.
15. Ribeiro AQ, Rozenfeld S, Klein CH, Cezar CC, Acúrcio FA. Inquérito sobre uso de medicamentos por idosos aposentados. Rev Saúde Pública 2008; 42:724-32.
16. Loyola Filho AI, Uchôa E, Lima-Costa MF. Estudo epidemiológico de base populacional sobre uso de medicamentos entre idosos na Região Metropoli-tana de Belo Horizonte, Minas Gerais, Brasil. Cad Saúde Pública 2006; 22:2657-67.
17. Ahola TL, Kantola IM, Puukka P, Kattainen A, Klaukka T, Reunanen A, et al. Positive change in the utilization of antihypertensive and lipid modi-fying drugs among adult CHD patients in Finland: results from a large national database between 2000 and 2006. Eur J Cardiovasc Prev Rehabil 2010; 17:477-85.
18. Wolf HK, Andreou P, Bata IR, Comeau DG, Gregor RD, Kephart G, et al. Trends in the prevalence and treatment of hypertension in Halifax County from 1985 to 1995. CMAJ 1999; 161:699-704.
19. Carrasco-Garrido P, Jiménez-García R, Astasio-Arbiza P, Ortega-Molina P, de Miguel G. Psycho-tropics use in the Spanish elderly: predictors and evolution between years 1993 and 2003. Pharma-coepidemiol Drug Saf 2007; 16:449-57.
20. Zuvekas SH. Prescription drugs and the changing patterns of treatment for mental disorders, 1996-2001. Health Aff 2005; 24:195-205.
21. Hollingworth SA, Eadie MJ. Antiepileptic drugs in Australia: 2002-2007. Pharmacoepidemiol Drug Saf 2010; 19:82-9.
22. Lima-Costa MF, Firmo JOA, Uchoa E. Cohort pro-file: The Bambuí (Brazil) Cohort Study of Ageing. Int J Epidemiol 2010; [Epub ahead of print]. 23. Lima-Costa MF, Firmo JOA, Uchôa E. The Bambuí
Cohort Study of Aging: methodology and health profile of participants at baseline. Cad Saúde Pública 2011; 27 Suppl 3:S327-35.
24. Klarin I, Fastbom J, Wimo A. A population-based study of drug use in the very old living in a rural district of Sweden, with focus on cardiovascular drug comsuption: comparison with an urban co-hort. Pharmacoepidemiol Drug Saf 2003; 12:669-78. 25. Loyola Filho AI, Uchôa E, Firmo JOA, Lima-Costa
MF. Estudo de base populacional sobre o consumo de medicamentos entre idosos: Projeto Bambuí. Cad Saúde Pública 2005; 21:545-53.
26. Lynd LD, Taylor J, Dobson R, Willison DJ. Prescrip-tion to over-the-counter deregulaPrescrip-tion: are we ready for it, or do we need to be? CMAJ 2005; 173:775-7. 27. Chobanian AV, Bakris GL, Black HR, Cushman WC,
Green LA, Izzo Jr. JL, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 Report. JAMA 2003; 289:2560-72. 28. Ministério da Saúde. Plano de Reorganização da
Atenção da Hipertensão Arterial e Diabetes Melli-tus: manual da hipertensão arterial e do diabetes mellitus. http://bvsms.saude.gov.br/bvs/publica coes/miolo2002.pdf (accessed on 27/Oct/2010). 29. Goldstein LB, Adams R, Alberts MJ, Appel LJ, Brass
30. Savica R, Beghi E, Mazzaglia G, Innocenti F, Bri-gnoli O, Cricelli C, et al. Prescribing patterns of an-tiepileptic drugs in Italy: a nationwide population-based study in the years 2000-2005. Eur J Neurol 2007; 14:1317-21.
31. Cloyd J, Hauser W, Towne A, Ramsay R, Mattson R, Gilliam F, et al. Epidemiological and medical as-pects of epilepsy in the elderly. Epilepsy Res 2006; 68 Suppl 1:S39-48.
32. Borges MA, Min LL, Guerreiro CAM, Yacubian EMT, Cordeiro JA, Tognola WA, et al. Urban preva-lence of epilepsy: populational study in São José do Rio Preto, a medium-sized city in Brazil. Arq Neuropsiquiatr 2004; 62:199-205.
33. Linjakumpu T, Hartikainen S, Klaukka T, Koponen H, Kivelä SL, Isoaho R. Psychotropics among the home-dwelling elderly: increasing trends. Int J Geriatr Psychiatry 2002; 17:874-83.
34. Freitas MPD, Loyola Filho AI, Lima-Costa AI. Dys-lipidemia and the risk of incident hypertension in a population of community-dwelling Brazilian elderly: the Bambuí Cohort Study of Aging. Cad Saúde Pública 2011; 27 Suppl 3:S351-9.
35. Balluz LS, Kieszak MA, Philen RM, Mulinare J. Vi-tamin and mineral supplement use in the United States. Arch Fam Med 2000; 9:258-62.
36. Hanlon JT, Fillenbaum GG, Ruby CM, Gray S, Bo-hannon A. Epidemiology of over-the-counter drug use in community dwelling elderly: United States perspective. Drugs Aging 2001; 18:123-31. 37. Huang HY, Caballero B, Chang S, Alberg AJ, Semba
RD, Schneyer CR, et al. The efficacy and safety of multivitamin and mineral supplement use to pre-vent cancer and chronic disease in adults: a sys-tematic review for a National Institutes of Health State-of-the-Science Conference. Ann Intern Med 2006; 145:372-85.
Submitted on 30/Nov/2010