www.revportcardiol.org
Revista
Portuguesa
de
Cardiologia
Portuguese
Journal
of
Cardiology
CASE
REPORT
Uhl’s
disease:
An
uncommon
presentation
of
a
rare
disease
Sílvia
Aguiar
Rosa
a,∗,
Ana
Figueiredo
Agapito
a,
Marta
António
b,c,
Lídia
de
Sousa
a,
José
Alberto
Oliveira
a,
Sérgio
Laranjo
b,
Susana
Martins
d,
Nuno
Jalles
Tavares
c,
Fátima
F.
Pinto
b,
Rui
Cruz
Ferreira
aaCardiologyDepartment,SantaMartaHospital,Lisbon,Portugal
bPaediatricCardiologyDepartment,SantaMartaHospital,Lisbon,Portugal cCentrodeRessonânciaCaselas,Lisbon,Portugal
dCardiologyDepartment,SantaMariaHospital,Lisbon,Portugal
Received28February2017;accepted11June2017 Availableonline9July2018
KEYWORDS Uhl’sdisease; Primaryright ventriculardisease; Cardiacmagnetic resonanceimaging
Abstract Uhl’sdisease,alsoknownasUhlanomaly,isararediseasesecondarytoselectivebut uncontrolledapoptosisofrightventricularmyocytesduringtheperinatalperiod,aftercomplete cardiacdevelopment,leadingtotheabsenceofrightventricularmyocardiumandthedirect appositionofendocardiumtoepicardiumwithoutamyocardiallayerinbetween,resultingin rightventricularfailure.
ThepresentpaperdescribesacaseofUhl’sdiseasewithanuncommonpresentation.A 28-year-oldmanwasadmittedwithdyspneaandcyanosis.Transthoracicechocardiographyshowed severedilationoftherightchambers,impairedrightventricularsystolicfunctionandalarge
ostiumsecundumatrialseptaldefect(ASD).Cardiaccatheterizationrevealedpulmonary hyper-tension,withincreasedpulmonarycapillarywedgepressure(mean19mmHg)andQp:QS0.88:1. Atthispoint,theauthorsconsideredthatamaindiagnosisofASDcouldnotexplaintheclinical featuresandhemodynamicdata.Aprimarydiseaseoftherightventriclewasthemostlikely hypothesisandcardiacmagnetic resonanceimaging wasperformed,which demonstratedan extremelythin-walledrightventricle,withalmostcompleteabsenceofrightventricularfree wallmyocardium,compatiblewithUhl’sdisease.
©2018SociedadePortuguesadeCardiologia.PublishedbyElsevier Espa˜na,S.L.U.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗Correspondingauthor.
E-mailaddress:[email protected](S.AguiarRosa).
https://doi.org/10.1016/j.repc.2017.06.025
0870-2551/©2018SociedadePortuguesadeCardiologia.PublishedbyElsevierEspa˜na,S.L.U.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
admitidopordispneiaecianose.Oecocardiogramatranstorácicodocumentoudilatac¸ãograve dascavidadesdireitas,compromissoda func¸ãosistólica doventrículo direitoe umagrande comunicac¸ãointerauricularostiumsecundum.Ocateterismocardíacorevelouhipertensão pul-monarcomaumentodapressãocapilar(média19mmHg); Qp:Qs0,88:1.Nestemomento,os autoresconsideraramqueacomunicac¸ãointerauricularcomodiagnósticoprincipalnão expli-cavaaapresentac¸ãoclínicaeosdadoshemodinâmicos.Doenc¸aprimáriadoventrículodireito tornou-seahipótesemaisprovável,peloqueserealizouumaressonânciamagnéticacardíaca quedemonstrouumventrículodireitocomparedeextremamentefina,comausência pratica-mentetotaldomiocárdiodaparedelivre,compatívelcomdoenc¸adeUhl.
©2018SociedadePortuguesadeCardiologia.PublicadoporElsevierEspa˜na,S.L.U.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Uhl’s anomaly was first described by Osler in 1905. The exactincidenceofthisrareconditionisunknown.In1993, Gerlis et al. concluded that many cases of arrhythmo-genic right ventricular dysplasia (ARVD) were incorrectly classifiedasUhl’s anomaly.Insaid paper,theauthors dis-cussed 84 real Uhl’s disease cases, and since then fewer cases have been reported.1 Uhl’s anomaly is a rare
dis-easesecondarytotheselectivebutuncontrolledapoptosis ofright ventricularmyocytes during theperinatal period, following complete cardiac development. This explains the absenceof the right ventricular myocardiumand the directappositionof endocardiumtoepicardium withouta myocardiallayerin between,resultingin rightventricular failure.2
Furthermore, some studies suggest that the overex-pressionof vascular endothelial growthfactor may playa roleinimpairingthedevelopmentofthe rightventricular myocardium.3
In Uhl’s disease, the absence of the right ventricular myocardium leads to a lack of contraction and, conse-quently, the chamber acts as a transition zone between the right atrium and pulmonary artery. Pulmonary cir-culation is maintained by the pumping action of the right atrium, whereas the right ventricle (RV) balloons aneurysmally in systole. The right atrium is enormous in size.4
In the past, diagnosis was performed during autopsy. However,nowadays,giventhedevelopmentofimaging tech-niques,diagnosisiscarriedoutviaechocardiographyormore sensitive and specific cardiac magnetic resonance (CMR) imaging.4 Moreover, therearealso publishedcases where
diagnosistookplaceduringprenatalscreening.5
Case
report
The authors report the case of a 28-year-old man, with no knownheart disease and an insignificant personal and familymedical history. However,hedid note that hehad sufferedcyanosisoverthepastthreeyears,whichwasnever investigated,andhadnoothersymptoms.Thepatientwas admitted to the hospital due to a respiratory infection, presenting withfever,dyspneaandhypoxemia (peripheral oxygensaturationof55%).
Electrocardiogram(ECG) showedatrialfibrillation(±77 bpm), right bundle branch block and a fragmented QRS complex --- despite normal left ventricular activation, rightventriculardepolarizationwasdelayedandprolonged (Figure1).
AchestX-rayrevealedcardiomegaly,withanarrow vas-cularpedicle(Figure1).Computedtomographyofthechest showeddilatedrightheartchambers,inferiorvenacavaand hepatic veins,withnodilatation of thepulmonary artery. Pulmonary ventilation/perfusion scintigraphy ruled out a pulmonary embolism and indicated a right-to-left shunt. Transthoracic echocardiography confirmed severe dilation oftherightheartchambersandimpaired rightventricular systolic function (Figure 1); a tricuspid valve with nor-malimplantationandmoderateregurgitation;anestimated pulmonary artery systolicpressureof 36 mmHg;a normal pulmonary arterydiameter; anda largeostium secundum
atrial septal defect (ASD) (38 mm), confirmed by trans-esophagealechocardiography.
Cardiac catheterization was performed, revealing an absence of gradient between the RV and pulmonary artery and post-capillary pulmonary hypertension (mean pulmonary artery pressure of 32 mmHg, with an ele-vated pulmonary capillary wedge pressure of 19 mmHg).
Figure1 A:ChestX-rayrevealingcardiomegalywithnopulmonaryarterydilatation;B:Electrocardiogramshowingatrial fibrilla-tionandrightbundlebranchblock.C:Transthoracicechocardiographyshowingsevererightchambersdilation,particularlyofthe rightatrium,andalargeostiumsecundumatrialseptaldefect.
Apulmonarybloodflow:systemicbloodflowratioof0.88:1 wasalsocalculated.
At this point, the authors felt that ASD as the pri-mary diagnosis could not explain the clinical features or hemodynamicdata.On onehand,therewasnoanomalous venousreturntojustifythecyanosisandmildpostcapillary pulmonary hypertension was not compatible with Eisen-menger’ssyndromeandtheconsequentright-to-leftshunt. Onthe otherhand, therewasnoevidenceofasignificant past or present left-to-right shunt, since the pulmonary arterywasnormalinsize.
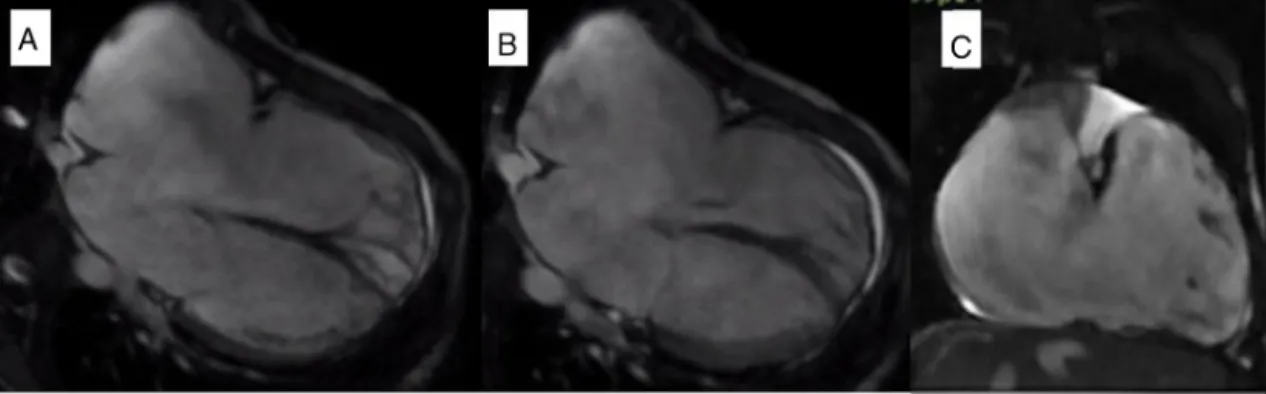
Primary right ventricular disease was the most likely hypothesisandCMR wasperformed, revealingsevere dila-tion of the right atrium (91×72 mm) and right ventricle (end-diastolicvolume355ml,207.9ml/m2),an extremely
thin-walledRVwithalmost completeabsenceof theright ventricularfreewallmyocardium,a paucityof apical tra-beculationsandimpairedsystolicfunction(ejectionfraction [EF] 25%) (Figure 2). The left ventricle was dilated with normalwallthicknessandanEFof41%.AnASDmeasuring over 30 mm was identifiedand late gadolinium enhance-mentwasobserved intheright ventricleandright atrium walls(Figure3).ThesefindingswerecompatiblewithUhl’s anomaly.
Cardiopulmonary exercise testing showed a moderate exercise capacity with a peak oxygen uptake of 27.6 ml/kg/min (55% of the value predicted for the patient’s genderandage)aswellasan oxygenuptakeatanaerobic thresholdof 20.5 ml/kg/min anda minute ventilation-to-carbondioxideoutputslopeof46.2.
The patientinitiated anticoagulationtherapywith war-farinandreceivedasubcutaneousimplantable cardioverter-defibrillatorforprimarypreventionofsuddencardiacdeath,
duetosevererightventriculardysfunction.Thepatientwill becloselymonitoredandhearttransplantationwillbe con-sideredintheeventhisfunctionalcapacitydeteriorates.
Discussion
Uhl’s disease is characterized by the absence of the RV myocardiumand the direct apposition of endocardium to epicardium.2
Histological examination confirms cardiac muscle wastage and replacement by fibrous tissue.6 However,
despitethisanomalyintheRVmyocardium,theseptaland leftventricularmyocardiumispreserved.4,7
In severe forms, RV failure develops during childhood, withpulmonary circulation being dependent onthe right atrium.Cyanosis is alsopresent in the event of an atrial shunt.4
Prior to the advent of current imaging methods, diag-nosiswasperformedduringautopsy.Nowadays,CMRisthe methodofchoicefordiagnosis,aswellasformorphologic andfunctionalevaluation.4
The association of Uhl’s disease with other congeni-tal heart defects had rarely been reported, namely with tricuspid valve dysplasia or absence, Ebstein’s anomaly, pulmonary atresia or regurgitation, patent ductus arte-riosus, ASD and hypoplasia of the mitral valve and left ventricle.1,8---12
AdifferentialdiagnosisshouldbeperformedwithARVD. Fromahistologicalpointofview,ARVDischaracterizedby fibrofattyinfiltrationoftherightventricularfreewallwhich is absent in Uhl’s disease, where fibrosis predominates.13
Figure2 Cardiovascular magnetic resonance: Steady-statefree precession imagingdocumenting severedilationofthe right atriumandrightventricle,anextremelythin-walledrightventriclewithalmostcompleteabsenceoftherightventricularfreewall myocardium,withapaucityofapicaltrabeculations,inafour-chamberviewindiastole(A)andsystole(B),andcoronalview(C). Anatrialseptaldefectmeasuringover30mmwasalsoidentified.
Figure3 Lategadoliniumenhancement(LGE)acquired10minutesafterintravenousgadoliniumadministration.LGEisevident intherightventricularandrightatriumwalls,inthefour-chamberview(A),rightventricleview(B)andshortaxisview(C).
heart failure, rather than arrhythmic events and sudden death.6,10FamilyhistoryisalsomorecommoninARVDthan
inUhl’sdisease.10
Regardingelectrocardiographicstudies,inARVD,T-wave inversionsinV1andV2arenoted,alongwithEpsilonwaves. Uhl’sdisease,ontheotherhand,presentsafragmentedQRS complex.7,13 In CMR, Uhl’s disease is characterized by an
extremelydilatedthin-walledRVwithseverehypokinesis,a paucityoftrabeculationsandnofatsignalintheRVwall,as seeninARVD.InARVD,focalwallmotionabnormalitiesare morefrequent,contrastingwiththeglobalhypokinesisseen inUhl’sdisease.4,7,13
Ebstein’s anomaly should also be considered in differ-entialdiagnosis.InUhl’sdiseasethetricuspidvalvehinges normallyandisnotdysplastic.4
Withregardtosurgicaltreatment, arightheart bypass canbeperformed.However,thisprocedurecarriesariskof clotsformingintherightventricleaswellasembolization, particularlyinthepresenceofabidirectionalGlennshunt.14
AnotheroptioninvolvesalmostentirelyresectingtheRVfree wall.15Possiblecomplicationsincluderecurrentventricular
dilatationandarrhythmias.Inthesecases,aresidualRVfree wallmustberuledoutandatotalcavopulmonaryconnection performed.16
Ifclinicaldeteriorationpersists,thetreatmentapproach shouldbeorthotopiccardiactransplantation.17
Inour case, the association of RV myocardium disease withalargeASDexplainsthepatient’suniqueclinical evo-lution.
CyanosisinthepresenceofanASD(witha‘‘normal’’RV) mayoccurintwocircumstancesthatwerenotpresentinthis case: severe pulmonary hypertension with Eisenmenger’s syndromeandtheconsequentright-to-leftshunt,or when ananomaloussystemicvenousreturnexists.
Furthermore,thelackofpulmonaryarterydilationshows that,althoughtheASDislarge,therewasprobablyno signif-icantleft-to-rightshunt.Theinexistenceofsuchashuntis duetothefactthatashuntisdependentofthecompliance ofbothventriclesinASDs,andinthiscaseonlytheRVwas affected.Overtheyears,progressiveRVdysfunctionledto aright-to-leftshuntandconsequentcyanosis.Moreover,the defectactsasanescape,whichhasuntilnowpreventedthe occurrenceofovertright-sidedheartfailure.
TheECGisalsonotable,withafragmentedQRScomplex, reflecting the delay and prolongation of right ventricular depolarization.
In conclusion, this case shows that clinical symptoms, hemodynamic data and imaging findings must be com-prehensively and thoroughly reviewed in congenital heart diseaseinordertoenablecorrectdiagnosis.PrimaryRV dis-easeshouldbeconsideredwhenRVfailureispresentinthe absenceofvalvediseaseandpulmonaryhypertension.Uhl’s
anomalyisararediseasethatconsistsintheabsenceofthe RVmyocardiumandprogressiveRVfailure.
Conflicts
of
interest
Theauthorshavenoconflictsofinteresttodeclare.
References
1.GerlisLM,Schmidt-OttSC,HoSY,etal.Dysplasticconditionsof therightventricularmyocardium:Uhl’sanomalyvs arrhythmo-genicrightventriculardysplasia.BrHeartJ.1993;69:142---50. 2.HébertJL,DuthoitG,Hidden-LucetF,etal.Imagesin
cardio-vascularmedicine,fortuitousdiscoveryofpartialUhlanomaly inamaleadult.Circulation.2010;121:e426---9.
3.Feucht M, Christ B, Wilting J. VEGF induces cardiovas-cular malformation and embryonic lethality. Am J Pathol. 1997;151:1407---16.
4.GreerML,MacDonaldC,AdatiaI.MRIofUhl’sanomaly. Circu-lation.2000;101:E230---2.
5.PhilipS,BharatiS,CherianKM,etal.Prenataldiagnosisofuhl anomalywithautopsycorrelation.AJPRep.2016;6:e91---5. 6.TanoueY,KadoH,ShiokawaY.Uhl’sanomalycomplicatedwith
criticalventriculararrhythmiaina2-month-oldinfant.EurJ CardiothoracSurg.2003;24:1040---2.
7.OtmaniA,LeborgneL,RenardC,etal.Imagesincardiovascular medicine,electrocardiogram,echocardiography,andmagnetic resonanceimagingcharacteristicsinUhl’sdisease.Circulation. 2007;115:e11---2.
8.vanderPalenRL,vanderWalAC,RoblesdeMedinaPG,etal. Uhl’sanomaly:clinicalspectrumandpathophysiology.IntJ Car-diol.2016;209:118---21.
9.TaksandeAM,GautamiV.Uhl’sanomalywithabsenttricuspid valveinaninfant.JCardiovascEchogr.2015;25:90---2. 10.IkariNM,AzekaE,AielloVD,etal.Uhl’sanomaly,differential
diagnosisandindicationforcardiactransplantationinaninfant. ArqBrasCardiol.2001;77:69---76.
11.Pamukcu O, Ozyurt A, Argun M,et al. Unusual right ventri-cleaneurysmanddysplasticpulmonaryvalvewithmitralvalve hypoplasia.AnnPediatrCardiol.2013;6:167---9.
12.VaidyanathanK,AgarwalR,JohariR, etal.Isolated congeni-talpulmonaryregurgitationwithrightventricularoutflowtract aneurysm --- a rare variant of Uhl’s anomaly. J Card Surg. 2010;25:415---7.
13.MarcusFI,McKennaWJ,SherrillD,etal.Diagnosisof arrhyth-mogenicrightventricularcardiomyopathy/dysplasia:proposed modificationofthetaskforcecriteria.Circulation.2010. 14.AzhariN,Assaqqat M,BulbulZ.Successfulsurgical repairof
Uhl’sanomaly.CardiolYoung.2002;12:192---5.
15.Yoshii S, Suzuki S, Hosaka S, et al. A case of Uhl anomaly treatedwithoneandahalfventriclerepaircombinedwith par-tialrightventriculectomyininfancy.JThoracCardiovascSurg. 2001;122:1026---8.
16.Sano S, Ishino K, Kawada M, et al. Total right ventricular exclusionprocedure:anoperationforisolatedcongestiveright ventricularfailure.JThoracCardiovasc.2002;123:640---7. 17.IkariNM,AzekaE,AielloVD,etal.Uhl’sanomaly,Differential
diagnosisandindicationforcardiactransplantationinaninfant. ArqBrasCardiol.2001;77:69---76.