Rev. Saúde Pública vol.35 número3
Texto
Imagem
Documentos relacionados
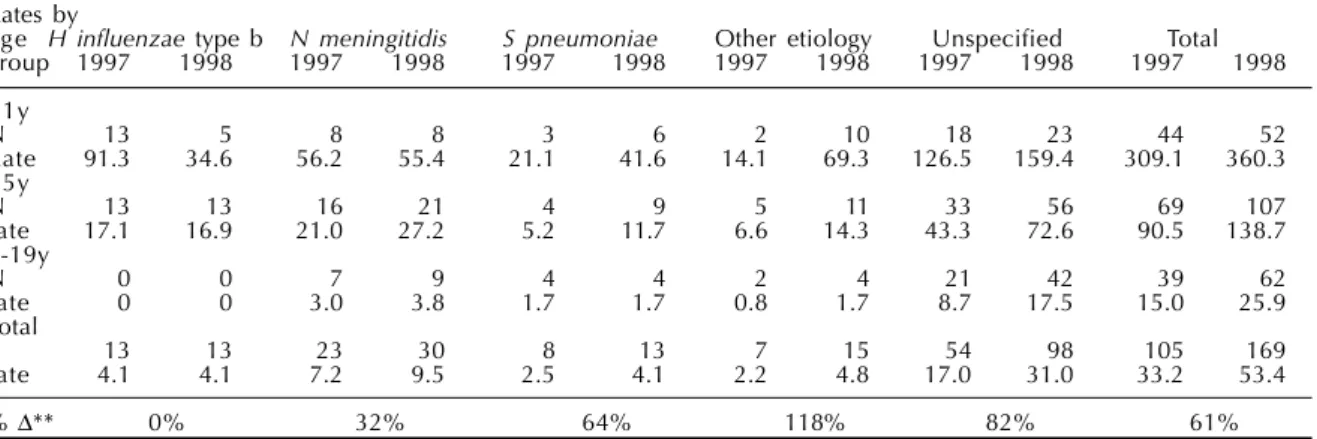
Incidence and mortality rates * and prevented cases and deaths ** from Haemophilus infl uenzae type b or unspecifi ed bacterial meningitis in children less than 5 years of
Através das fontes escritas, além de uma investigação da história da região e dos grupos estudados, pode-se averiguar se efetivamente havia indígenas na região,
Affievolito il corpo dalle sofferenze patite nella sua vita, pro- strato l'animo dall'idea fissa che i suoi compagni, che avevano militato con lui sotto la bandiera repubblicana
Ousasse apontar algumas hipóteses para a solução desse problema público a partir do exposto dos autores usados como base para fundamentação teórica, da análise dos dados
Em sua pesquisa sobre a história da imprensa social no Brasil, por exemplo, apesar de deixar claro que “sua investigação está distante de ser um trabalho completo”, ele
From the 12 studies included (13 entries) in this meta-analysis, they all started from the same research assumption, in which the elderly with classifications according to the
The study was based on the frequency and incidence of the disease, from the number of positive cases reported in the State, through active and passive search; the cases were
The prevalence of estruses with cloudy vaginal mucus in the present study was lower than some of the incidence rates previously reported for uterine infections –
