Rev. Saúde Pública vol.46 número2
Texto
Imagem


Documentos relacionados
Portanto concluímos essa revisão bibliográfica que deixa evidente necessário de promover práticas educacionais voltadas para uma educação postural, com orientação, oficinas
Em pacientes com trauma craniomaxilofacial, esta técnica promove uma via aérea segura e permeável, proporcionando uma maior liberdade para o manejo e redução das fraturas de
It is extremely important to discuss the fac- tors that influenced the results observed in all the analyzed hospitalizations, especially those asso- ciated with the expansion of
Uma vez que o mercado de trabalho pode diferenciar-se de ilha para ilha, nomeadamente devido a uma maior localização de determinadas actividades nas ilhas de maior dimensão, a
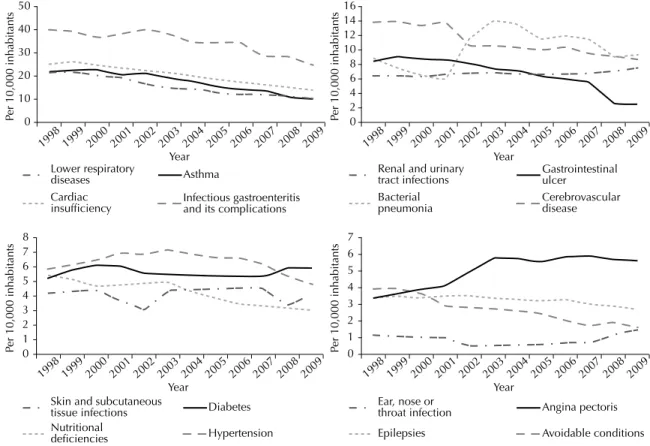
Results: the regression coefficient was 0.97, showing a decrease of 3% per year in hospitalizations owing to ambulatory care sensitive conditions, a three-fold increase in
The objective of the present study was to analyze the proportions of costs of hospitalizations for ambulatory care sensitive conditions (ACSC) in relation to total
Table 1 – Distribution of the included studies in the systematic review concerning the causes for general hospitalizations ambulatory care sensitive conditions related
However, with the creation of the Unified National Health System (Sistema Único de Saúde – SUS), for health researchers, and especially for those in collective health, the
