w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Poor
muscle
strength
and
function
in
physically
inactive
childhood-onset
systemic
lupus
erythematosus
despite
very
mild
disease
Ana
Jéssica
Pinto
a,
Fabiana
Braga
Benatti
b,
Hamilton
Roschel
a,b,
Ana
Lúcia
de
Sá
Pinto
b,
Clovis
Artur
Silva
c,
Adriana
Maluf
Elias
Sallum
c,
Bruno
Gualano
a,b,∗aUniversidadedeSãoPaulo(USP),GrupodePesquisaemFisiologiaAplicadaeNutric¸ão,SãoPaulo,SP,Brazil
bUniversidadedeSãoPaulo(USP),FaculdadedeMedicina,DivisãodeReumatologia,SãoPaulo,SP,Brazil
cUniversidadedeSãoPaulo(USP),FaculdadedeMedicina,InstitutodaCrianc¸a,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received22January2016 Accepted12April2016 Availableonline8August2016
Keywords: Musclefunction Strength
Rheumaticdisease Physicalactivitylevel
a
b
s
t
r
a
c
t
Objective:Tocomparemusclestrength(i.e.lower-andupper-bodystrength)andfunction betweenphysicallyinactivechildhood-onsetsystemiclupuserythematosuspatients(C-SLE) andhealthycontrols(CTRL).
Methods:Thiswasacross-sectionalstudyandthesampleconsistedof19C-SLE(agebetween 9and18years)and15CTRLmatchedbyage,sex,bodymassindex(BMI),andphysical activitylevels(assessedbyaccelerometry).Lower-andupper-bodystrengthwasassessed bytheone-repetition-maximum(1-RM) test.Isometricstrengthwasassessed througha handgripdynamometer.Musclefunctionwasevaluatedbythetimed-standstest(TST)and thetimed-up-and-gotest(TUG).
Results:When compared with CTRL,C-SLEshowed lower leg-press andbench-press 1-RM(p=0.026andp=0.008,respectively),andatendencytowardlowerhandgripstrength (p=0.052).C-SLEshowedlowerTSTscores(p=0.036)andatendencytowardhigherTUG scores(p=0.070)whencomparedwithCTRL.
Conclusion: PhysicallyinactiveC-SLEpatientswithverymilddiseaseshowedreduced mus-clestrengthandfunctionalitywhencomparedwithhealthycontrolsmatchedbyphysical activitylevels.ThesefindingssuggestC-SLEpatientsmaygreatlysufferfromaphysically inactivelifestylethanhealthycontrolsdo.Moreover,somesub-clinical“residual”effectof thediseaseoritspharmacologicaltreatmentseemstoaffectC-SLEpatientsevenwitha well-controlleddisease.
©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](B.Gualano). http://dx.doi.org/10.1016/j.rbre.2016.07.012
Reduc¸ão
na
forc¸a
muscular
e
capacidade
funcional
em
pacientes
fisicamente
inativos
com
lúpus
eritematoso
sistêmico
de
início
juvenil,
apesar
de
doenc¸a
muito
leve
Palavras-chave: Forc¸amuscular Capacidadefuncional Doenc¸areumática Níveldeatividadefísica
r
e
s
u
m
o
Objetivo: Compararaforc¸amuscular(ouseja,aforc¸amusculardosmembrosinferiorese superiores)eacapacidadefuncionaldepacientesfisicamenteinativoscomlúpus eritem-atososistêmicodeiníciojuvenilLESJcomcontrolessaudáveis(CTRL).
Métodos: Trata-sedeumestudotransversalcujaamostrafoicompostapor19pacientes comLESJ(idadesentre9a18anos)e15CTRLpareadosporidade,sexo,índicedemassa corporal(IMC)eníveldeatividadefísica(avaliadaatravésdousodeacelerômetros).Aforc¸a demembrosinferioresesuperioresfoiavaliadapelotestedeumarepetic¸ãomáxima (1-RM).Aforc¸aisométricafoiavaliadacomousodeumdinamômetro.Acapacidadefuncional foiavaliadapeloTimed-standstest(TST)eTimed-up-and-gotest(TUG).
Resultados:QuandocomparadosaosCTRL,ospacientescomLESJapresentarammenorforc¸a em1-RMnolegpressesupino(p=0,026ep=0,008,respectivamente),eumatendênciaa menorforc¸adepreensãomanual(p=0,052).OspacientescomLESJapresentarammenores escoresnoTST(p=0,036)eumatendênciaamaiortempodeexecuc¸ãonoTUG(p=0,070), quandocomparadosaogrupoCTRL.
Conclusão: PacientescomLESJ,fisicamenteinativos,comdoenc¸amuitolevemostraram reduc¸ão na forc¸a muscular e capacidade funcional quando comparados a controles saudáveispareadosporníveisdeatividadefísica.Estesachadossugeremquepacientes comLESJpodemapresentarmaisefeitosdeletériospormanterumestilodevida fisica-menteinativodoquecontrolessaudáveis.Alémdisso,algunsefeitos“residuais”subclínicos dadoenc¸aouotratamentofarmacológicoparecemafetarpacientescomLESJ,mesmocom umadoenc¸abemcontrolada.
©2016ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Childhood-onsetsystemiclupuserythematosus(C-SLE)isan
autoimmune diseasecharacterizedbyBand T cells
hyper-activity,formationanddepositionofantibodiesthroughout thebody,whichresultsinchronicsystemicinflammationand multi-organinvolvement(e.g.skin,kidney,muscle, cardiovas-cularsystem,etc.).1–4 C-SLEhasaprevalenceof3–24cases per100,000inhabitants5andhasbeenassociatedwithamore severediseasethanadult-SLE.6
Diseaseitself(e.g.systemicinflammation)and drug
reg-imen (e.g. prolonged corticoid use) may contribute to a
multitude of clinical manifestations (e.g. musculoskeletal disorders,physicaldysfunction and fatigue),7–9 which may, ultimately, predispose patients to a sedentary lifestyle. A sedentary lifestyle, in turn, may negatively affect physi-cal capacity, function, and health-related quality of life, in a vicious circle of physical inactivity and poor
clini-cal outcomes.10 A few studies have shown that pediatric
rheumatic populations are not engaged in sufficient
lev-els of physical activity compared to healthy children and adolescents.11–13However,althoughitisplausibletoassume thatasedentarybehaviormayaffectphysicalcapacity,this remainstobedetermined.
Theaimof this study was tocompare muscle strength
(i.e.lower-andupper-bodystrength) and functionbetween physically inactive C-SLE and healthy controls (CTRL). We
hypothesizedthatphysicallyinactivepatientswithlow dis-easeactivityandlowcumulativedamagewouldshowsimilar musclestrengthandfunctionwhencomparedtohealthy con-trolsmatchedforphysicalactivitylevels.
Patients
and
methods
Studydesignandpatients
Thiswasacross-sectionalstudyconductedinSaoPaulo,Brazil (ClinicalHospital,SchoolofMedicine,UniversityofSaoPaulo).
The sampleconsistedof 19C-SLE patients(age between9
and 18 years) and 15 healthy controls (CTRL) matchedfor
age,sex,bodymassindex(BMI),andphysicalactivitylevels (assessedbyaccelerometer).Aerobiccapacity,health-related quality oflife,andphysicalactivity leveldatafrom partof thissamplehasbeenreportedelsewhere.14 Diseaseactivity
wasdeterminedbymeansofSystemicLupusErythematosus
Exclusion criteria were as follows: (1) physically
active patients (according to general physical activity
recommendations)18;(2)cardiovascularandmusculoskeletal disorders;(3)kidneyandpulmonaryinvolvement;(4) periph-eralneuropathy,(5)secondaryrheumaticdisease(e.g.Sjögren syndrome,fibromyalgia,andantiphospholipidsyndrome).
TheCommitteeofEthicsinResearchoftheGeneral Hos-pitaloftheSchoolofMedicine,UniversityofSaoPaulo,Brazil (CAPPesq)approvedthestudyandalllegalguardiansprovided writteninformedconsent.
Physicalactivitylevelassessment
Physicalactivity was objectivelymeasured using Actigraph GT3X® accelerometers(ActiGraph,Pensacola,FL).All
partic-ipants were instructed to wear the accelerometer during
wakinghours,exceptwhenbathingorswimming,forseven
consecutive days.All participantsaccumulatedatleastten hours of valid activity recordings per day for atleast five
days. Data were exported from the device in 15-s epochs
forchildrenandadolescents,usingActiLife6software (Acti-Graph,Pensacola,FL).Eversoncut-pointswereusedtodefine epochsforchildrenandadolescentsasfollows:sedentarytime (<100counts/min), light-intensity physicalactivity (≥101 to <2295counts/min),andMVPA(moderate-to-vigorousphysical activity)(≥2296counts/min).19Physicalactivityguidelines
rec-ommendaminimumof60min/dayofMVPAforchildrenand
adolescents.18Thus,participantswereconsideredphysically activeiftheymetthisrecommendation.
Musclestrengthandfunction
Participantsperformedtwopreliminarysessions,separatedby atleast72hours,tofamiliarizethemselvestothemain exer-cisetests.Theseconsistedofone-repetition-maximum(1-RM)
tests to determine both upper- and lower-body muscular
strength,asassessedbybench-pressandleg-pressexercise, respectively.Priortothe1-RM test,twolightwarm-upsets interspersedbytwo-minuteintervalswereperformed. Subse-quently,participantsachieved1-RMforeachexercisein1–5 attemptsinterspersedby3-minintervals.201-RMtestswere conductedbytwoexperiencedresearchersandverbal encour-agementwasprovidedduringtestingsessions.
Isometric strength was assessed through a handgrip
dynamometer(TakeiA5001HandGripDynamometer,Takei
ScientificInstrumentsCo.,Ltd.,Tokyo, Japan).Theprotocol consistedofthreemaximalisometriccontractionsof5s inter-spersedwith60-srecoveryperiods.Thetestwasperformedon theparticipant’sdominanthand.21
Musclefunctionwasevaluated bythe timed-standstest (TST)andthetimed-up-and-gotest(TUG).TSTassessesthe
maximumnumberofstand-upsthatasubjectcanperform
from a standard armless chairwithin30s,22 whereas TUG assesses the time required for the subject to rise from a standardarmchair,walktowarda3-meterslinedrawnonthe floor,turn,returntothechair,andsitdownagain.23
Statisticalanalysis
Data normality was tested using the Shapiro–Wilk W
-test.Independentsampleswere comparedusingeitherthe
unpaired T-test for normally distributed variables or the Mann–WhitneyU-testfornon-normallydistributedvariables. DataanalysiswasperformedusingtheSPSS(17.0)for Win-dows.Thelevelofsignificancewassetatp≤0.05.Dataare presentedasmean±standarddeviation(SD),95%confidence intervalofthedifference(CI)werealsocalculated.
Results
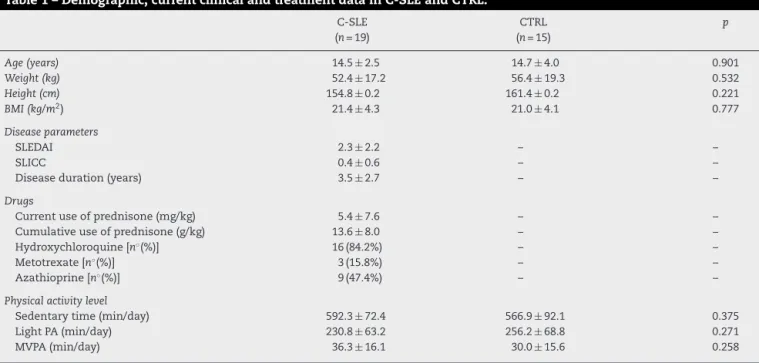
Table1showsdemographicdata,currentclinicaltreatment, diseaseactivityanddamageparametersinC-SLEandCTRL. Groupswerecomparableregardingage,sex,BMIandphysical activitylevels(p>0.05).
Musclestrengthandfunction
MusclestrengthandfunctiondataarepresentedinTable2. WhencomparedwithCTRL,C-SLEshowedlowerleg-pressand bench-press1-RM(p=0.026andp=0.008,respectively),anda tendencytowardlowerhandgripstrength(p=0.052).
Additionally,C-SLEshowedlowerTSTscores(p=0.036)and atendencytowardhigherTUGscores(p=0.070)when com-paredwithCTRL.
Discussion
Themainfindingofthisstudywasthatphysicallyinactive C-SLEpatientswithverymildandwell-controlleddiseasehad
impairedmusclestrengthandfunctionwhencomparedwith
healthycontrolsmatchedbyphysicalactivitylevels.
Disease-related symptoms and clinical manifestations
maypredisposethepediatricrheumaticpatienttoaphysically inactivelifestyle.10,24,25Physicalinactivityinchildhoodmay trackintoadulthoodandsenescence,andhasbeenassociated withahigherriskofdevelopingchronicdiseases(e.g.obesity, type2diabetes, hypertension),and all-causemortality.26–28
Moreover, physical inactivity may result in weakness and
muscledysfunction,ultimatelyleadingtopoorhealth-related quality of life.10,26 In this study, we expected that C-SLE patientswithverymilddisease(i.e.lowcumulativedamage andlowdiseaseactivity)wouldshowsimilarlevelsofmuscle strengthandfunctionwhencomparedwithcontrolsmatched by physical inactivity. Based on our findings, nonetheless, onemayassumethatinsufficientphysicalactivitylevelmay imposeagreater“cost”toC-SLEthantohealthycontrolsin relationtoweaknessandmuscledysfunction.
Itisnotclearwhy musclestrength and functionhighly differphysicallyinactivewell-controlledC-SLEpatientsand healthycontrols.Toavoidanyapparentdisease-related symp-tomsthatcouldpotentiallyaccountfordifferencesinphysical capacity,weselectedonlypatientswithlowdiseaseactivity (meanSLEDAI=2),lowcumulativedamage(meanSLICC=0.4),
and free of musculoskeletal involvement. Yet, remarkable
Table1–Demographic,currentclinicalandtreatmentdatainC-SLEandCTRL.
C-SLE (n=19)
CTRL (n=15)
p
Age(years) 14.5±2.5 14.7±4.0 0.901
Weight(kg) 52.4±17.2 56.4±19.3 0.532
Height(cm) 154.8±0.2 161.4±0.2 0.221
BMI(kg/m2) 21.4±4.3 21.0±4.1 0.777
Diseaseparameters
SLEDAI 2.3±2.2 – –
SLICC 0.4±0.6 – –
Diseaseduration(years) 3.5±2.7 – –
Drugs
Currentuseofprednisone(mg/kg) 5.4±7.6 – –
Cumulativeuseofprednisone(g/kg) 13.6±8.0 – –
Hydroxychloroquine[n◦(%)] 16(84.2%) – –
Metotrexate[n◦(%)] 3(15.8%) – –
Azathioprine[n◦(%)] 9(47.4%) – –
Physicalactivitylevel
Sedentarytime(min/day) 592.3±72.4 566.9±92.1 0.375
LightPA(min/day) 230.8±63.2 256.2±68.8 0.271
MVPA(min/day) 36.3±16.1 30.0±15.6 0.258
BMI,bodymassindex;MVPA,moderate-to-vigorous;PA,physicalactivity;SLEDAI,SystemicLupusErythematosusDiseaseActivityIndex;SLICC, SystemicLupusInternationalCollaboratingClinics/ACRDamageIndex.
Dataareexpressedasmeans±SD.
Table2–MusclestrengthandfunctioninC-SLEandCTRLgroups.
C-SLE (n=19)
CTRL (n=15)
p 95%CI
Lower Upper
Legpress(kg) 96.9±39.3 135.9±50.9 0.026a −72.93 −4.99
Benchpress(kg) 17.7±5.7 24.6±8.3 0.008a −11.85 −1.93
Handgrip(kg) 21.3±6.7 26.0±6.3 0.052 −9.36 0.04
Timedstandstest(reps) 18.1±1.6 19.6±2.2 0.036a −2.83 −0.11
Timedup&gotest(s) 5.5±0.5 5.2±0.3 0.070 −0.04 0.62
Dataareexpressedasmeans±SD. CI,confidenceintervals.
a Significantdifferencewhencomparedtohealthycontrolgroups.
explain,at least partially, the reductionin physical capac-ity experienced by C-SLE patients. Moreover, studies have shownthatC-SLEpatientsmayhaveselectiveatrophyof type-IImusclefiber,impairedexcitation–contractioncoupling,and microcirculatorylesions,30,31whichcoulddirectlyaffect mus-clestrength and function inthis disease.The influenceof potentialabnormalmusclemorphologyuponmuscle dysfunc-tioninC-SLEremainsunclear,aswewereunabletomeasure musclemassoranyothermusclephysiologicalparametersin thisstudy.
Adult-SLE populations appear to have reduced physical
capacity (e.g. aerobic conditioning, muscle strength and
function),higherfatigueanddisabilitywhencomparedwith theirhealthcounterparts.32–34Tothebestofourknowledge, onlyonestudyshowedloweraerobiccapacity,higherfatigue, andpoorerhealth-relatedqualityoflifeinaC-SLEcohort,35 although physicalactivity level was not well-controlled in this investigation.From ourfindings, it ispossibleto infer thatphysical inactivitycan contributeto aggravatemuscle
function deficitsseen inC-SLEpatientstoa greaterextent thaninhealthycontrols.Furtherstudiesinvolvingonly phys-icallyactivepatientsandcontrolsmayprovidenovelinsights onthe impactofabroaderrangeofphysicalactivity levels onstrengthandfunction,allowingtestingwhetherincreased physicalactivitymayovercomemuscledysfunctioninC-SLE. Increased activity levels through exercise training
pro-grams have been proven to be effective on counteracting
disease-relatedsymptomsandimprovephysicalcapacityin several rheumatic populations.10,25,36–38 To the best of our knowledge,however, asinglecasereport andasingle
ran-domized controlled trial have been conducted to test the
efficacyofaerobictraininginC-SLEpatients,36,39withbothof themshowingpositivefindingsinrelationtoimprovements inphysicalcapacity, disease symptoms,and health-related qualityoflife.Furtherstudiesareclearlynecessaryto inves-tigatetheefficacyandsafetyofmorecomplexinterventions inC-SLE(e.g.structuredandnon-structuredactivitiesaimed
children-oriented physical activities, programs focused on reducingsedentarytime,individualandcollectivesports).
Inconclusion,physicallyinactiveC-SLEpatientswithvery milddiseaseshowedreducedmusclestrengthand functional-itywhencomparedwithhealthycontrolsmatchedbyphysical activity levels. These findings suggest C-SLE patients may greatlysufferfromaphysicallyinactivelifestylethanhealthy controlsdo.Moreover,somesub-clinical“residual”effectof thediseaseoritspharmacologicaltreatmentseemstoaffect C-SLEpatientsevenwithawell-controlleddisease.
Conflict
of
interests
Theauthorsdeclarenoconflictofinterests.
Acknowledgements
TheauthorsarethankfultoFundac¸ãodeAmparoàPesquisa do Estado de São Paulo for the financial support (FAPESP: 2013/13126-2).
r
e
f
e
r
e
n
c
e
s
1. GuerraSG,VyseTJ,CunninghameGrahamDS.Thegenetics oflupus:afunctionalperspective.ArthritisResTher. 2012;14:211.
2. ChaiHC,PhippsME,ChuaKH.Geneticriskfactorsof systemiclupuserythematosusintheMalaysianpopulation:a minireview.ClinDevImmunol.2012;2012:963730.
3. RahmanA,IsenbergDA.Systemiclupuserythematosus.N EnglJMed.2008;358:929–39.
4. MavrogeniS,ServosG,SmerlaR,Markousis-MavrogenisG, GrigoriadouG,KolovouG,etal.Cardiovascularinvolvement inpediatricsystemicautoimmunediseases:theemerging roleofnoninvasivecardiovascularimaging.InflammAllergy DrugTargets.2015;13:371–81.
5. MalattiaC,MartiniA.Paediatric-onsetsystemiclupus erythematosus.BestPractResClinRheumatol. 2013;27:351–62.
6. BrunnerHI,GladmanDD,IbanezD,UrowitzMD,Silverman ED.Differenceindiseasefeaturesbetweenchildhood-onset andadult-onsetsystemiclupuserythematosus.Arthritis Rheum.2008;58:556–62.
7. HershA,vonSchevenE,YelinE.Adultoutcomesof childhood-onsetrheumaticdiseases.NatRevRheumatol. 2011;7:290–5.
8. MunozLE,JankoC,SchulzeC,SchornC,SarterK,SchettG, etal.Autoimmunityandchronicinflammation–two clearance-relatedstepsintheetiopathogenesisofSLE. AutoimmunRev.2010;10:38–42.
9. LaxerRM.Long-termtoxicityofimmunesuppressionin juvenilerheumaticdiseases.Rheumatology(Oxford). 1999;38:743–6.
10.GualanoB,SaPintoAL,PerondiB,LeitePradoDM,OmoriC, AlmeidaRT,etal.Evidenceforprescribingexerciseas treatmentinpediatricrheumaticdiseases.AutoimmunRev. 2010;9:569–73.
11.HendersonCJ,LovellDJ,SpeckerBL,CampaigneBN.Physical activityinchildrenwithjuvenilerheumatoidarthritis: quantificationandevaluation.ArthritisCareRes. 1995;8:114–9.
12.MaggioAB,HoferMF,MartinXE,MarchandLM,BeghettiM, Farpour-LambertNJ.Reducedphysicalactivityleveland
cardiorespiratoryfitnessinchildrenwithchronicdiseases. EurJPediatr.2010;169:1187–93.
13.Kashikar-ZuckS,FlowersSR,VerkampE,TingTV, Lynch-JordanAM,GrahamTB,etal.Actigraphy-based physicalactivitymonitoringinadolescentswithjuvenile primaryfibromyalgiasyndrome.JPain.2010;11:885–93. 14.PintoAJ,MiyakeCNH,BenattiFB,SilvaCA,SallumAME,
BorbaE,etal.Reducedaerobiccapacityandqualityoflifein physicallyinactivepatientswithsystemiclupus
erythematosuswithmild/inactivedisease.ArthritisCareRes (Hoboken).2016,doi:10.1002/acr.22905.
15.GladmanDD,IbanezD,UrowitzMB.Systemiclupus erythematosusdiseaseactivityindex2000.JRheumatol. 2002;29:288–91.
16.GladmanD,GinzlerE,GoldsmithC,FortinP,LiangM,Urowitz M,etal.Thedevelopmentandinitialvalidationofthe SystemicLupusInternationalCollaboratingClinics/American CollegeofRheumatologydamageindexforsystemiclupus erythematosus.ArthritisRheum.1996;39:363–9.
17.HochbergMC.UpdatingtheAmericanCollegeof Rheumatologyrevisedcriteriafortheclassificationof systemiclupuserythematosus.ArthritisRheum. 1997;40:1725.
18.WHO.Globalrecommendationsonphysicalactivityfor health.Geneva:WorldHealthOrganization;2010[Accessedin 2015].Availablein:http://www.who.int/dietphysicalactivity/ factsheetrecommendations/en/.
19.EvensonKR,CatellierDJ,GillK,OndrakKS,McMurrayRG. Calibrationoftwoobjectivemeasuresofphysicalactivityfor children.JSportsSci.2008;26:1557–65.
20.BrownLE,WeirJP.ASEPProceduresRecommendationI: AccurateAssessmentOfMuscularStrengthAndPower. JEPonline2001.p.1–21.
21.LohmannTG,RocheAF,MartorellR.Anthropometric standardizationreferencemanual.Champaign:Human KineticsBooks;1988.p.177.
22.NewcomerKL,KrugHE,MahowaldML.Validityandreliability ofthetimed-standstestforpatientswithrheumatoid arthritisandotherchronicdiseases.JRheumatol. 1993;20:21–7.
23.PodsiadloD,RichardsonS.Thetimedup&go:atestofbasic functionalmobilityforfrailelderlypersons.JAmGeriatrSoc. 1991;39:142–8.
24.TakkenT,vanderNetJ,KuisW,HeldersPJ.Physicalactivity andhealthrelatedphysicalfitnessinchildrenwithjuvenile idiopathicarthritis.AnnRheumDis.2003;62:885–9. 25.KlepperSE.Exerciseinpediatricrheumaticdiseases.Curr
OpinRheumatol.2008;20:619–24.
26.HardyLL,DobbinsTA,Denney-WilsonEA,OkelyAD,Booth ML.Sedentariness,small-screenrecreation,andfitnessin youth.AmJPrevMed.2009;36:120–5.
27.deRezendeLF,RodriguesLopesM,Rey-LopezJP,MatsudoVK, LuizOdoC.Sedentarybehaviorandhealthoutcomes:an overviewofsystematicreviews.PloSOne.2014;9:e105620. 28.TremblayMS,LeBlancAG,KhoME,SaundersTJ,LaroucheR,
ColleyRC,etal.Systematicreviewofsedentarybehaviour andhealthindicatorsinschool-agedchildrenandyouth.IntJ BehavNutrPhysAct.2011;8:98.
29.KasturiS,SammaritanoLR.CorticosteroidsinLupus.Rheum DisClinNorthAm.2016;42:47–62.
30.OxenhandlerR,HartMN,BickelJ,ScearceD,DurhamJ,Irvin W.Pathologicfeaturesofmuscleinsystemiclupus
erythematosus:abiopsyserieswithcomparativeclinicaland immunopathologicobservations.HumPathol.1982;13: 745–57.
32.StocktonKA,KandiahDA,ParatzJD,BennellKL.Fatigue, musclestrengthandvitaminDstatusinwomenwith systemiclupuserythematosuscomparedwithhealthy controls.Lupus.2012;21:271–8.
33.TenchC,BentleyD,VleckV,McCurdieI,WhiteP,D’CruzD. Aerobicfitness,fatigue,andphysicaldisabilityinsystemic lupuserythematosus.JRheumatol.2002;29:474–81.
34.KeyserRE,RusV,CadeWT,KalappaN,FloresRH,Handwerger BS.Evidenceforaerobicinsufficiencyinwomenwith systemiclupuserythematosus.ArthritisRheum. 2003;49:16–22.
35.HoughtonKM,TuckerLB,PottsJE,McKenzieDC.Fitness, fatigue,diseaseactivity,andqualityoflifeinpediatriclupus. ArthritisRheum.2008;59:537–45.
36.PradoDM,BenattiFB,deSa-PintoAL,HayashiAP,GualanoB, PereiraRM,etal.Exercisetraininginchildhood-onset
systemiclupuserythematosus:acontrolledrandomizedtrial. ArthritisResTher.2013;15:R46.
37.PerandiniLA,Sales-de-OliveiraD,MelloS,CamaraNO, BenattiFB,LimaFR,etal.Inflammatorycytokinekineticsto singleboutsofacutemoderateandintenseaerobicexercise inwomenwithactiveandinactivesystemiclupus
erythematosus.ExercImmunolRev.2015;21:174–85. 38.OmoriCH,SilvaCA,SallumAM,RodriguesPereiraRM,
LuciadeSaPintoA,RoschelH,etal.Exercisetrainingin juveniledermatomyositis.ArthritisCareRes.2012;64: 1186–94.