w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Leptin
and
adiponectin
in
patients
with
systemic
lupus
erythematosus:
clinical
and
laboratory
correlations
Vitalina
de
Souza
Barbosa
a,∗,
Paulo
Luiz
Francescantônio
b,
Ni´lzio
Antônio
da
Silva
aaUniversidadeFederaldeGoiás,Goiânia,GO,Brazil
bPontifíciaUniversidadeCatólicadeGoiás,Goiânia,GO,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received19January2014 Accepted26August2014 Availableonline2February2015
Keywords:
Systemiclupuserythematosus Leptin
Adiponectin
a
b
s
t
r
a
c
t
Objective:To evaluate the serumlevels ofleptin and adiponectininpatients with
sys-temiclupuserythematosus(SLE)andcorrelatetheirlevelswithdiseaseactivity,presence ofautoantibodiesandclinicalmanifestations.
Methods:52womenwithSLEand33healthywomenwereevaluated.Thepatientswere
dividedintotwogroups,thefirstwithactiveSLEandthesecondwithinactiveSLE.Patients withSLEDAI≥3wereconsideredactive. Serumlevelsofleptin(ng/mL)andadiponectin (g/mL)weremeasuredbyenzymeimmunoassay.
Results:There was a significant difference in leptin levels between SLE and controls
(20.7±17.1vs.8.0±5.0ng/mL,p<0.001),butnosignificantdifferenceinadiponectin lev-els(875±69.7vs.118.1±70.6pg/mL,p=0.053).Nosignificantdifferenceinlevelsofleptin andadiponectinwasnotedbetweeninactiveandactiveSLEgroups.Therewasasignificant associationbetweenlowlevelsofleptinandpositivityforanticardiolipin(aCL)(p=0.025) andlupusanticoagulant(LA)(p=0.003)andasignificantassociationbetweenhighlevels ofleptinandthepresenceofrenaldisease(p<0.001).However,therewasnoassociation betweenadiponectinlevelswithautoantibodiesandclinicalfeaturesinSLEpatients.
Conclusion:PatientswithSLEhadelevatedleptinlevels,withassociationwithrenal
involve-ment.Leptinandadiponectinwerenotcorrelatedwithdiseaseactivity.Lowlevelsofleptin havebeenassociatedwiththepresenceofLAandaCL.
©2014ElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](V.deSouzaBarbosa).
http://dx.doi.org/10.1016/j.rbre.2014.08.013
Leptina
e
adiponectina
no
lúpus
eritematoso
sistêmico:
correlac¸ões
clínicas
e
laboratoriais
Palavras-chave:
Lúpuseritematososistêmico Leptina
Adiponectina
r
e
s
u
m
o
Objetivo:Avaliarosníveisséricosdeleptinaeadiponectinaempacientescomlúpus
eritem-atososistêmico(LES)ecorrelacionarseusníveiscomatividadeinflamatória,presenc¸ade autoanticorposemanifestac¸õesclínicas.
Métodos: Foramavaliadas52mulherescomLESe33mulheressaudáveis.Aspacientes
foramdivididasemdoisgrupos,oprimeirocomLESativoeosegundocomLESinativo. ForamconsideradasematividadeaspacientecomSledai≥3.Osníveisséricosdeleptina (ng/mL)eadiponectina(ug/mL)forammedidosporensaioimunoenzimático.
Resultados: Houve diferenc¸a significativa nos níveis de leptina entre LES e controle
(20,7±17,1vs.8,0±5,0ng/mL,p<0,001),masnãohouvediferenc¸asignificativanosníveis deadiponectina(87,5±69,7vs.118,1±70,6ug/mL,p=0,053).EntreLESinativoeativo,não houvediferenc¸asignificativadosníveisdeleptinaeadiponectina.Houveumaassociac¸ão significativaentre osbaixosníveisde leptina epositividadeparaanticardiolipina (aCL) (p=0,025)eanticoagulantelúpico(LA)(p=0,003)eumaassociac¸ãosignificativaentreníveis elevadosdeleptinaedapresenc¸ademanifestac¸ãorenal(p<0,001).Noentanto,nãohouve associac¸ãoentreadiponectinacomautoanticorposecaracterísticasclínicasnaspacientes.
Conclusão: PacientescomLESapresentaramnívelelevadodeleptina,comassociac¸ãoao
envolvimentorenal.Aleptinaeaadiponectinanãosecorrelacionaramcomaatividadeda doenc¸a.Baixosníveisdeleptinaforamassociadoscomapresenc¸adeLAeaCL.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Inrecent years,amajor routelinking metabolismand the immunesystemhasbeendescribed,afterverificationofan inflammatorystateinobesity.1Theadiposetissueisanorgan
thatperformsneuroendocrine andimmune functions, pro-ducing various cytokines that include IL-6 and TNF-alpha, leptin,adiponectinandresistin,knownasadipokines.These cytokinesparticipateinavarietyofphysiologicalprocesses, suchasfoodintake,insulinsensitivity,atherosclerosis, immu-nity and inflammation.2 They represent a new group of
proteinsreleasedfromadipocytes,whichactasmodulators of the immune system.3 Studies demonstrate the
partici-pationofthesesubstancesinrheumaticand inflammatory diseases.4–7
Leptinactsontheimmunesystemasaproinflammatory cytokine.Inanimalmodels,itsdeficiencyisassociatedwith an increased susceptibility to infection and reducing the inflammation.8Itpromotestheproliferationandactivationof
TlymphocytesandinducesproductionofTh1cytokines.1,9,10
Studieshavereportedincreasedleptinlevelsinsystemiclupus erythematosus(SLE)patients.11–13
Adiponectinhasanti-inflammatoryaction.14Itinhibitsthe
proliferationandactivationofTlymphocytes,aswellas lym-phopoiesisandBlymphocytes.15Highlevelsofadiponectin
werefoundinpatientswithSLE,12,16,17althoughthereisstill
controversy.
Theaimofthisstudywastoevaluatethelevelsofleptinand adiponectininpatientswithSLEanditspossiblecorrelation withdiseaseactivity,presenceofautoantibodiesandclinical manifestations.
Patients
and
methods
52femalepatientswhomettheAmericanCollegeof Rheuma-tology (ACR) classification criteria for SLE,18 hospitalized
and/orinoutpatientcareattheRheumatologyDepartment, HospitaldasClínicas,MedicineSchool,UniversidadeFederal deGoiás(HC/FM/UFG)wereincluded.
Thepatientsweredividedintotwosubgroups:asubgroup ofpatientswithactiveSLE(n=21)andanothersubgroupof patientswithinactivedisease(n=31).Thecontrolgroup com-prised 33 healthy women matched for age. The exclusion criteriawere:patientsyoungerthan18yearsold,pregnancy, history of myocardial infarction or diabetes, liver disease, renal failure, prednisone >20mg/dayand body mass index (BMI)>30kg/m2.
ThestudywasapprovedbytheResearchEthicsCommittee oftheHC/UFGandallparticipantswhoagreedtoparticipate signedaninformedconsentform.
Theevaluationofpatientsincludeddemographics,ageat disease onset,diseaseduration,clinicalmanifestationsand physicalexamination.Atthetimeofevaluation,lipidprofile, fastingglucoseandtestsofinflammatoryactivitywerealso obtainedforeachpatient.Autoantibodiesfoundintheclinical recordwereconsidered;forthosepatientsforwhom autoan-tibodieswerenotfound,thesewererequestedatthetimeof theirinclusioninthestudy.
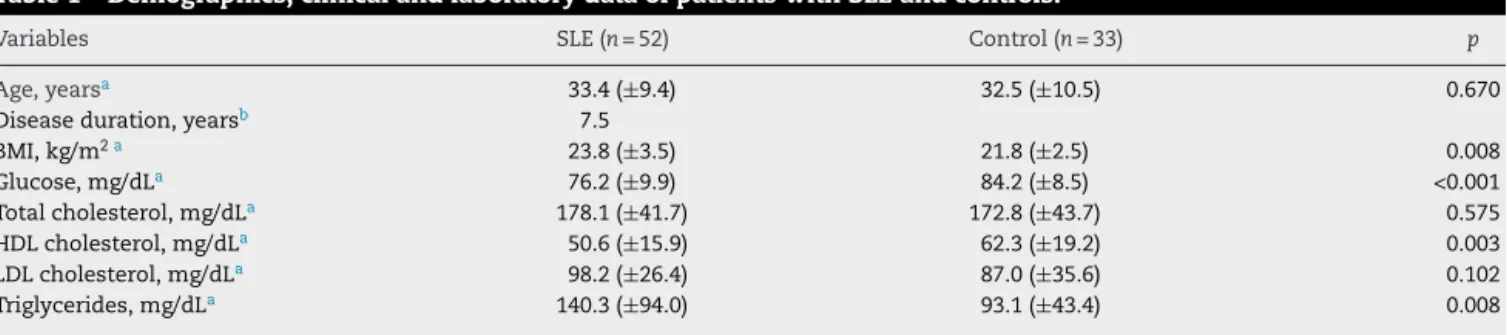
Table1–Demographics,clinicalandlaboratorydataofpatientswithSLEandcontrols.
Variables SLE(n=52) Control(n=33) p
Age,yearsa 33.4(±9.4) 32.5(±10.5) 0.670
Diseaseduration,yearsb 7.5
BMI,kg/m2a 23.8(±3.5) 21.8(±2.5) 0.008
Glucose,mg/dLa 76.2(±9.9) 84.2(±8.5) <0.001
Totalcholesterol,mg/dLa 178.1(±41.7) 172.8(±43.7) 0.575
HDLcholesterol,mg/dLa 50.6(±15.9) 62.3(±19.2) 0.003
LDLcholesterol,mg/dLa 98.2(±26.4) 87.0(±35.6) 0.102
Triglycerides,mg/dLa 140.3(±94.0) 93.1(±43.4) 0.008
SLE,systemiclupuserythematosus;BMI,bodymassindex;HDL,highdensitylipoprotein;LDL,lowdensitylipoprotein.
a Datapresentedasmean(±standarddeviation).
b Datapresentedasmean.
on Crithidia lucillae. A survey of antibodies to extractable
nuclear antigens(ENA),anti-Ro, anti-La, anti-Smand anti-RNP, as well as to anticardiolipin, was performed in the General Laboratory, HC/FM/UFG, by ELISA (Enzyme Linked ImmunoSorbentAssay).
Diseaseactivity was assessedatinclusion in the study, usingSLEDAI(SystemicLupusErythematosusDisease Activ-ityIndex).19PatientswithSLEDAI≥3wereconsideredactive.
Inpatientswithdiseaseactivity,onlyanti-DNAand comple-ment(C3andC4)levelsbroughtatthetimeofinclusionwere considered.
Forthedeterminationofleptin,theELISAtechniquewas used,inatypicalcaptureassayintwostages,orin“sandwich”, accordingtothemanufacturer’sinstructions(DBC– Diagnos-ticsBiochemCanada).Theassaysensitivitywas100ng/mL. ThelevelofadiponectinwasalsoobtainedbyELISAina quan-titativesandwich,according tothemanufacturer’s protocol (MBLInternationalCorp.,Woburn,MA,USA),andthe sensi-tivityoftheassay was100pg/mL,withamean recoveryof 90–105%ofadiponectin.
Statistical
analysis
All statisticalanalysiswere performedusing theStatistical PackageforSocialSciences (SPSSInc.,Chicago,IL)for Win-dows,version18.Student’st-testwasusedforindependent samples;equivalentvariancesweredefinedbyLevene’sF-test. Theverificationofthenormalityofthedistributionwasdone byKolgomorovandSmirnovtest.TheMann–Whitneytestwas usedforquantitativevariables thatwere notnormally dis-tributed.CorrelationswerecalculatedbyPearsoncorrelation. Categoricalvariableswereanalyzedbythechi-squaredtest(a measureofassociation).Forallstatisticalevaluations,p<0.05 wasconsideredstatisticallysignificant.
Results
Therewasnostatisticaldifferencebetweenthemeanageof SLEpatientsandcontrols(33.4±9.4yearsvs.32.5±10.5years,
p=0.670).Thebodymassindex washigherin SLEpatients compared to controls (23.8±3.5kg/m2 vs. 21.8±2.5kg/m2,
p=0.008).Themetabolicevaluationbetweengroupsshowed nodifferenceinlevelsoftotalandLDLcholesterol,butthere wasadifferenceinbloodglucoselevels,HDLandtriglycerides (Table1).
Table2–CharacteristicsofpatientswithSLE(n=52), accordingtothediseaseactivity.
ActiveSLE (n=21)
InactiveSLE (n=31)
p
Age,years* 33.4(±9.9) 33.6(±9.1) 0.861a
BMI,kg/m2* 23.7(±3.5) 24.0(±3.6) 0.760a
Diseaseduration,years* 6.0(±6.6) 9.0(±6.4) 0.110a
ESR,mm/L2h* 64.7(±35.4) 31.8(±21.6) <0.001a
ANA-positive,% 90.5% 93.5% 0.170b
Anti-ENA,% 85.7% 61.3% 0.056b
Anti-DNA,% 52.4% 35.5% 0.223b
LA,% 19% 9.7% 0.331b
aCL,% 14.3% 9.7% 0.610b
SLEDAI* 7.42(±3.9) 0.20(±0.8) <0.001c
SLE,systemiclupuserythematosus;BMI,bodymassindex;ESR,
erythrocytesedimentationrate;ANA,antinuclearfactor;Anti-ENA,
anti-extractablenuclearantigenantibody;LA,lupusanticoagulant;
aCL,anticardiolipin;SLEDAI,SystemicLupusErythematosus
Dis-easeActivityIndex.
∗ Datapresentedasmean(±standarddeviation).
a t-Test.
b Chi-squaredtest.
c Mann–Whitneytest.
Table2presents thecharacteristics ofSLEpatientswith active disease (n=21). The mean age in the active SLE groupwassimilartothegroupofpatientswithinactiveSLE (33.4±9.9yearsvs.33.6±9.1years,p=0.861).BMIdidnotdiffer betweenpatientswithactiveSLEandpatientswithinactive disease (24.0±3.6kg/m2 vs. 23.7±3.5kg/m2, p=0.760).
Dis-easedurationwasnotsignificantlydifferentbetweenthetwo groups(9.0±6.4yearsvs.6.0±6.6years,p=0.110).Themean durationofdiseaseactivitywas5.6months.Withregardsto autoantibodies(ANA,anti-ENA,anti-DNA,LAandaCL),there wasnostatisticaldifferencebetweengroups.
Adiponectin levelswere lower inSLEpatients, although therewasnosignificantdifferencewhencomparedwith con-trols (87.5±69.7 vs.118.1±70.6g/mL, p=0.053). Therewas also no significant difference betweenpatients withactive and inactive SLE(88.8±74.4 vs.85.5±95.9g/mL,p=0.866). Leptin levels in SLE patients and controls are shown in
Figs. 1and2. Leptinlevelswere significantlyhigherinSLE patientscomparedtocontrols(20.7±17.1vs.8.0±5.0ng/mL,
80
70
60
50
40
30
20
10
0 SLE 20.7 (17.1)
Control 8.0 (5.0) p<0.001
Leptin ng/ml
Figure1–Serumleptinlevels(DP)inSLEpatientsand controls.
The correlation between leptin levels and lipid profile, bloodglucoseandBMIshowedapositiveassociationbetween leptin levels and HDL (r=0.34, p=0.014) and between lep-tin levels and BMI (r=0.34, p=0.014) only in SLE patients. Adiponectinlevelswerenotcorrelatedtothevariablesstudied inSLEpatients.
There was no significant correlation of leptin with ESR (r=−0.062,p=0.666)orSLEDAI(r=−0.053,p=0.710),andthere wasalsonocorrelationofadiponectinwiththesevariables (ESR,r=0.047;p=0.743andSLEDAI,r=0.169,p=0.230).
No association of adiponectin with autoantibodies and clinicalfeaturesofSLEwasobserved(Table3).However,a sig-nificantassociationbetweenlowlevelsofleptinandpositivity foraCLandLAwasobserved,aswellasasignificant associ-ationbetweenhighlevelsofleptinandthepresenceofrenal involvement(Table4).
Discussion
Leptin isa proinflammatory cytokine thatappears to con-tributetosystemicinflammationinautoimmunerheumatic diseases,including SLE.4,5 Inthe present study, leptin
lev-els were significantly higher when compared with the control group, a finding that was alsoobserved in several studies.11–13,20–23
80
70
60
50
40
30
20
10
0
SLE-inactive 21.1 (19.8)
SLE-active 20.4 (15.3) p=0.84
Leptin ng/ml
Figure2–Serumleptinlevels(DP)ininactiveandactive SLEpatients.
However,Wislowskaetal.24foundnodifferenceinserum
leptinlevelsbetweenSLEpatientsandcontrols,whileDe Sanc-tis et al.25 observeda significantly lower level ofleptin in
patientswithSLE.
Inourstudy,nosignificantdifferencesinadiponectinlevels betweenpatientsandcontrolswasobserved,althoughthere wasatrendtowardlowerlevelsofadiponectininSLEpatients, whichwassimilartotheresultsfoundbyVadaccaetal.21,22
andMcMahonetal.23
DifferentresultswerefoundbySadaetal.12Chungetal.20
andDeSanctisetal.,25whoobservedasignificantincreasein
adiponectinlevelsinpatientswithSLE.Asadiponectinplays an anti-inflammatory, anti-atherogenic and anti-diabetic role,14thosestudiesthatfoundahigherlevelofadiponectin
soughttojustifythisfindingasacompensatoryeffect.20,26
One possible explanation for the different activities of adiponectin is that low molecular weight adiponectin has anti-inflammatory activity,whereas high molecular weight adiponectinhasproinflammatoryaction,thelatterbeingmost commonlyfoundinplasma.14,27
In the present study, there was a positive association betweenleptinandBMIinpatientswithSLE,butnotinthe controlgroup.ThesamewasobservedbyChungetal.20We
observedanassociationofleptinlevelswithHDL-cholesterol but notwithLDL-cholesterolandtriglycerides,asfoundby Chungetal.20
Regardingadiponectin,therewasnocorrelationwithany ofthevariablesstudied,althoughChungetal.20havefound
anegativeassociationofadiponectinwithBMIandapositive associationwithHDL-cholesterol.
Inthisstudy,therewasnostatisticalcorrelationbetween the levels of leptin and adiponectin with disease activ-ity, measured by SLEDAIand ESR. Thelack ofrelationship betweendiseaseactivityandleptinwasalsoobservedinother studies.11,20,24,25,28
However,instudiesconductedbyVadaccaetal.,21,22 the
authorsobservedacorrelationbetweenleptinlevelsand activ-ity indices(SLEDAI and ECLAM) inSLE, but no correlation whatsoeveroftheseindiceswithadiponectin.Althoughleptin levelsarehigherinpatientswithSLE,thesedonotappearto beassociatedwithdiseaseactivityand,therefore,wouldnot beamarkerofdiseaseactivity.
Moststudies11–13,20,23–25includepatientswithlowdisease
activity,asthosewithhighactivityaregenerallytakinghigh dosesofcorticosteroidsand,thus,areexcluded.Therelation ofleptininpatientswithSLEactivitymaybefurtherclarified bystudiesinvolvingpatientswithhigherSLEDAIandwithout priortreatment.
In this study, there was no association between ANA, anti-ENA and anti-DNA autoantibodies with levels of lep-tin and adiponectin,but therewasan associationbetween low levelsofleptin andthe presenceofLAandaCL. None of the patients included in the study presented antiphos-pholipidsyndrome.Inourliteraturesurvey,wedidnotfind studies presenting a correlation between the presence of antiphospholipidantibodiesandleptininSLEpatients.Only Garcia-Gonzalezetal.11evaluatedthepresenceofanti-DNA
andleptinlevels,andfoundnocorrelation.
Table3–Associationofadiponectinlevelswiththepresenceofautoantibodiesandclinicalmanifestationsin52patients withsystemiclupuserythematosus.
Variables(n) Presentation(n) Adiponectin p
Normal(<11g/mL) High(≥11g/mL)
ANA(52) Positive(47) 13 34 0.136
Negative(5) 3 2
Anti-Ro(49) Positive(22) 5 17 0.280
Negative(27) 10 17
Anti-La(49) Positive(7) 1 6 0.310
Negative(42) 14 28
Anti-Sm(49) Positive(20) 7 13 0.580
Negative(29) 8 21
Anti-RNP(50) Positive(25) 6 19 0.355
Negative(25) 9 16
Anti-DNA(45) Positive(22) 6 16 0.815
Negative(23) 7 16
aCL(37) Positive(6) 2 4 0.959
Negative(31) 10 21
LA(41) Positive(6) 2 4 0.926
Negative(35) 11 24
Clinical
manifestation(21)
Renal(15) 5 10 0.472
CNS(2) 0 2
Cut/art(4) 2 2
ANA,antinuclearantibody;Anti-Ro,anti-SSA;Anti-La,anti-SSB;Anti-Sm,anti-Smith;Anti-RNP,anti-U1ribonucleoprotein;Anti-DNA, anti-deoxyribonucleicacid;aCL,anticardiolipin;LA,lupusanticoagulant;CNS,centralnervoussystem;Cut/art,cutaneousandarticular.
Chi-squaredtestofPearson.
withrenalinvolvement.Wislowskaet al.24 showedalower
levelofleptininpatientswitharthritisandCNSinvolvement compared to patients without such manifestations. How-ever,Kimetal.13foundnocorrelationbetweenleptinlevels
withclinicalmanifestations.Also,nostudiescorrelatingrenal involvementandleptinlevelswerefound.
Wang et al.29 demonstrated that the signaling pathway
of Jak/STAT plays an important role in the progression of nephritis in mice models. Considering that this signal-ing pathway is activated by leptin, maybe it could be the explanation of the correlation of renal disease and lep-tin.
Table4–Associationofleptinlevelswiththepresenceofautoantibodiesandclinicalmanifestationsin52patientswith systemiclupuserythematosus.
Variables(n) Presentation(n) Leptin p
Low(<3.7ng/mL) Normal(3.7–11.1ng/mL) High(>11.1ng/mL)
ANA(52) Positive(47) 11 8 28 0.200
Negative(5) 0 0 5
Anti-Ro(49) Positive(22) 5 1 16 0.210
Negative(27) 4 6 17
Anti-La(49) Positive(7) 1 1 5 0.830
Negative(42) 8 7 27
Anti-Sm(49) Positive(20) 5 3 12 0.394
Negative(29) 3 5 21
Anti-RNP(50) Positive(25) 6 3 16 0.465
Negative(25) 3 5 17
Anti-DNA(45) Positive(22) 5 6 11 0.120
Negative(23) 3 2 18
aCL(37) Positive(6) 4 0 2 0.025
Negative(31) 5 8 18
LA(41) Positive(6) 4 2 0 0.003
Negative(35) 5 5 25
Clinical
manifestation(21)
Renal(15) 4 0 11 <0.001
CNS(2) 0 2 0
Cut/art(4) 3 0 1
ANA,antinuclearantibody;Anti-Ro,anti-SSA;Anti-La,anti-SSB;Anti-Sm,anti-Smith;Anti-RNP,anti-U1ribonucleoprotein;Anti-DNA, anti-deoxyribonucleicacid;aCL,anticardiolipin;LA,lupusanticoagulant;CNS,centralnervoussystem;Cut/art,cutaneousandarticular.
Noneofthepatientsinthisstudyshowedimpairedrenal function, although higher levels of leptin in patients with chronickidneydiseaseweredescribedintheliterature.30This
studydidnotevaluatetheurinarylevelofleptin,andmore studiesareneededtodeterminewhetherhigherleptinlevels maybeamarkerofrenalactivity.
Currently,advancesinresearchrelatedtoSLEshowthatthe adipokinesmayrepresentanimportantgroupforthe discov-eryofcytokinesthathelptounderstandthepathophysiology ofthisdiseaseandthatcanalsoserveasaserologicmarker, assistingintheidentificationofpatientsatriskofdeveloping severeformsorbeingapredictorofdiseaseactivity.
Inconclusion,leptinlevelsarehigherinpatientswithSLE andtherewasatrendtoloweradiponectinlevels.High lep-tinlevelsdonotseemtoreflectthe activityofthedisease. Renalinvolvementwasthe onlyclinical manifestationthat wasassociatedwithincreasedleptinlevels,andtherewasan inverseassociationofserumlevelsofleptinwiththepresence oflupusanticoagulantandanticardiolipin.Theroleofleptin inSLEneedstobebetterclarified,andstudiesincludinglarger numbersofpatients,differentstagesofdiseaseanddifferent clinicalpresentationsarerequired.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. FantuzziG.Adiposetissue,adipokines,andinflammation.J AllergyClinImmunol.2005;115:911–9.Quiz20.
2. Antuna-PuenteB,FeveB,FellahiS,BastardJP.Adipokines:the missinglinkbetweeninsulinresistanceandobesity.Diabetes Metab.2008;34:2–11.
3. TilgH,MoschenAR.Adipocytokines:mediatorslinking adiposetissue,inflammationandimmunity.NatRev Immunol.2006;6:772–83.
4. KrysiakR,Handzlik-OrlikG,OkopienB.Theroleofadipokines inconnectivetissuediseases.EurJNutr.2012;51:513–28.
5. GomezR,CondeJ,ScoteceM,Gomez-ReinoJJ,LagoF,Gualillo O.What’snewinourunderstandingoftheroleofadipokines inrheumaticdiseases?NatRevRheumatol.2011;7:528–36.
6. ScoteceM,CondeJ,GomezR,LopezV,LagoF,Gomez-ReinoJJ, etal.Beyondfatmass:exploringtheroleofadipokinesin rheumaticdiseases.ScientificWorldJ.2011;11:1932–47.
7. LagoF,GomezR,CondeJ,ScoteceM,Gomez-ReinoJJ,Gualillo O.Cardiometaboliccomorbiditiesandrheumaticdiseases: focusontheroleoffatmassandadipokines.ArthritisCare Res(Hoboken).2011;63:1083–90.
8. LamQL,LuL.Roleofleptininimmunity.CellMolImmunol. 2007;4:1–13.
9. LaCavaA,MatareseG.Theweightofleptininimmunity.Nat RevImmunol.2004;4:371–9.
10.MatareseG,MoschosS,MantzorosCS.Leptininimmunology. JImmunol.2005;174:3137–42.
11.Garcia-GonzalezA,Gonzalez-LopezL,Valera-GonzalezIC, Cardona-MunozEG,Salazar-ParamoM,Gonzalez-OrtizM, etal.Serumleptinlevelsinwomenwithsystemiclupus erythematosus.RheumatolInt.2002;22:138–41.
12.SadaKE,YamasakiY,MaruyamaM,SugiyamaH,Yamamura M,MaeshimaY,etal.Alteredlevelsofadipocytokinesin associationwithinsulinresistanceinpatientswithsystemic lupuserythematosus.JRheumatol.2006;33:1545–52.
13.KimHA,ChoiGS,JeonJY,YoonJM,SungJM,SuhCH.Leptin andghrelininKoreansystemiclupuserythematosus.Lupus. 2010;19:170–4.
14.GuzikTJ,MangalatD,KorbutR.Adipocytokines–novellink betweeninflammationandvascularfunction?JPhysiol Pharmacol.2006;57:505–28.
15.YokotaT,MekaCS,KouroT,MedinaKL,IgarashiH,Takahashi M,etal.Adiponectin,afatcellproduct,influencesthe earliestlymphocyteprecursorsinbonemarrowculturesby activationofthecyclooxygenase–prostaglandinpathwayin stromalcells.JImmunol.2003;171:5091–9.
16.RovinBH,SongH,HebertLA,NadasdyT,NadasdyG, BirminghamDJ,etal.Plasma,urine,andrenalexpressionof adiponectininhumansystemiclupuserythematosus.Kidney Int.2005;68:1825–33.
17.ReynoldsHR,BuyonJ,KimM,RiveraTL,IzmirlyP,TunickP, etal.AssociationofplasmasolubleE-selectinand adiponectinwithcarotidplaqueinpatientswithsystemic lupuserythematosus.Atherosclerosis.2010;210:569–74.
18.HochbergMC.UpdatingtheAmericanCollegeof Rheumatologyrevisedcriteriafortheclassificationof systemiclupuserythematosus.ArthritisRheum. 1997;40:1725.
19.UribeAG,VilaLM,McGwinGJr,SanchezML,ReveilleJD, AlarconGS.Thesystemiclupusactivitymeasure-revised,the MexicanSystemicLupusErythematosusDiseaseActivity Index(Sledai),andamodifiedSledai-2Kareadequate instrumentstomeasurediseaseactivityinsystemiclupus erythematosus.JRheumatol.2004;31:1934–40.
20.ChungCP,LongAG,SolusJF,RhoYH,OeserA,RaggiP,etal. Adipocytokinesinsystemiclupuserythematosus:
relationshiptoinflammation,insulinresistanceandcoronary atherosclerosis.Lupus.2009;18:799–806.
21.VadaccaM,MargiottaD,RigonA,CacciapagliaF,CoppolinoG, AmorosoA,etal.Adipokinesandsystemiclupus
erythematosus:relationshipwithmetabolicsyndromeand cardiovasculardiseaseriskfactors.JRheumatol.
2009;36:295–7.
22.VadaccaM,ZardiEM,MargiottaD,RigonA,CacciapagliaF, ArcareseL,etal.Leptin,adiponectinandvascularstiffness parametersinwomenwithsystemiclupuserythematosus. InternEmergMed.2011;30.
23.McMahonM,SkaggsBJ,SahakianL,GrossmanJ,FitzGeraldJ, RagavendraN,etal.Highplasmaleptinlevelsconfer increasedriskofatherosclerosisinwomenwithsystemic lupuserythematosus,andareassociatedwithinflammatory oxidisedlipids.AnnRheumDis.2011;70:1619–24.
24.WislowskaM,RokM,StepienK,Kuklo-KowalskaA.Serum leptininsystemiclupuserythematosus.RheumatolInt. 2008;28:467–73.
25.DeSanctisJB,ZabaletaM,BiancoNE,GarmendiaJV,RivasL. Serumadipokinelevelsinpatientswithsystemiclupus erythematosus.Autoimmunity.2009;42:272–4.
26.ToussirotE,StreitG,WendlingD.Thecontributionofadipose tissueandadipokinestoinflammationinjointdiseases.Curr MedChem.2007;14:1095–100.
27.SongH,ChanJ,RovinBH.Inductionofchemokineexpression byadiponectininvitroisisoformdependent.TranslRes. 2009;154:18–26.
28.AlM,NgL,TyrrellP,BargmanJ,BradleyT,SilvermanE. Adipokinesasnovelbiomarkersinpaediatricsystemiclupus erythematosus.Rheumatology(Oxford).2009;48:497–501.
29.WangS,YangN,ZhangL,HuangB,TanH,LiangY,etal. Jak/STATsignalingisinvolvedintheinflammatoryinfiltration ofthekidneysinMRL/lprmice.Lupus.2010;19:1171–80.