w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Review
article
Contraception
for
adolescents
with
chronic
rheumatic
diseases
Benito
Lourenc¸o
a,∗,
Katia
T.
Kozu
b,
Gabriela
N.
Leal
c,
Marco
F.
Silva
b,
Elisabeth
G.C.
Fernandes
b,
Camila
M.P.
Franc¸a
b,
Fernando
H.C.
Souza
d,
Clovis
A.
Silva
a,b,daUniversidadedeSãoPaulo(USP),FaculdadedeMedicina,UnidadedoAdolescente,SãoPaulo,SP,Brazil
bUniversidadedeSãoPaulo(USP),FaculdadedeMedicina,UnidadedeReumatologiaPediátrica,SãoPaulo,SP,Brazil cUniversidadedeSãoPaulo(USP),FaculdadedeMedicina,UnidadedeRadiologia,SãoPaulo,SP,Brazil
dUniversidadedeSãoPaulo(USP),FaculdadedeMedicina,DivisãodeReumatologia,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received9September2015 Accepted12June2016 Availableonline6August2016
Keywords:
Contraception
Chronicrheumaticdisease Systemiclupuserythematosus Antiphospholipidantibody Emergencycontraception
a
b
s
t
r
a
c
t
Contraception isanimportantissueandshouldbea matterofconcerninevery medi-calvisitofadolescentandyoungpatientswithchronicrheumaticdiseases.Thisnarrative reviewdiscussescontraceptionmethodsinadolescentswithjuvenilesystemiclupus ery-thematosus(JSLE),antiphospholipidsyndrome(APS),juvenileidiopathicarthritis(JIA)and juveniledermatomyositis(JDM).Barriermethodsaresafeandtheiruseshouldbe encour-agedforall adolescentswithchronicrheumaticdiseases.Combinedoralcontraceptives (COC)arestrictlyprohibitedforJSLEandAPSpatientswithpositiveantiphospholipid anti-bodies.Reversiblelong-actingcontraceptioncanbeencouragedandofferedroutinelytothe JSLEadolescentpatientandotherrheumaticdiseases.Progestin-onlypillsaresafeinthe majorityofrheumaticdiseases,althoughthemainconcernrelatedtoitsusebyadolescents ispooradherenceduetomenstrualirregularity.Depotmedroxyprogesteroneacetate injec-tionseverythreemonthsisahighlyeffectivecontraceptionstrategy,althoughitslong-term useisassociatedwithdecreasedbonemineraldensity.COCorothercombinedhormonal contraceptivemaybeoptionsforJIAandJDMpatients.Orallevonorgestrelshouldbe con-sideredasanemergencycontraceptionmethodforalladolescentswithchronicrheumatic diseases,includingpatientswithcontraindicationtoCOC.
©2016PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](B.Lourenc¸o).
http://dx.doi.org/10.1016/j.rbre.2016.07.016
2255-5021/© 2016 Published by Elsevier Editora Ltda. This is an open access article under the CC BY-NC-ND license (http://
Contracepc¸ão
para
adolescentes
com
doenc¸as
reumáticas
crônicas
Palavras-chave:
Contracepc¸ão
Doenc¸areumáticacrônica Lúpuseritematososistêmico Anticorpoantifosfolípide Contracepc¸ãodeemergência
r
e
s
u
m
o
A contracepc¸ão é umaquestãoimportante e deve serum motivode preocupac¸ão em todaconsultamédicadepacientesadolescentesejovenscomdoenc¸asreumáticas crôni-cas.Esta revisãonarrativadiscutemétodoscontraceptivosem adolescentescomlúpus eritematososistêmico(LES),síndromeantifosfolipídica(SAF),artriteidiopáticajuvenil(AIJ) edermatomiositejuvenil(DMJ).Osmétodosdebarreirasãosegurosetodososadolescentes comdoenc¸asreumáticascrônicasdevemserincentivadosausá-los.Oscontraceptivosorais combinados(COC)sãoestritamenteproibidosparapacientescomLESJeSAFcom anti-corposantifosfolípidespositivos.Acontracepc¸ãoreversíveldeac¸ãoprolongadapodeser incentivadaeoferecidarotineiramenteapacienteadolescentecomLESeoutrasdoenc¸as reumáticas.Aspílulasquecontêmsomenteprogestinasãosegurasnamaiorpartedas doenc¸asreumáticas,emboraaprincipalpreocupac¸ãorelacionadacomseuusopor ado-lescentessejaabaixaadesãoemdecorrênciadairregularidademenstrual.Asinjec¸õesde acetatodemedroxiprogesteronadedepósitoacadatrêsmesessãoumaestratégiaaltamente eficazdecontracepc¸ão,emboraoseuusoemlongoprazoestejaassociadoàdiminuic¸ãona densidademineralóssea.Contraceptivosoraiscombinadosououtroscontraceptivos hor-monaiscombinadospodemseropc¸õesparapacientescomAIJeDMJ.Olevonorgestreloral deveserconsideradocomoummétododecontracepc¸ãodeemergênciaparatodasas ado-lescentescomdoenc¸asreumáticascrônicas,incluindopacientescomcontraindicac¸ãopara COC.
©2016PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobuma licenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
The prevalence of chronic diseases has been rising worldwide.1Infact,approximately20%ofAmerican
adoles-cents(12–17years)haveonecurrentchronicdiseaseand13% havetwoormorecurrentchronicdiseasesnowadays.2
Adolescentsdiagnosedwithchronicillnessesand disabil-ities live longer now than in the past. Those individuals experiencethe enthusiasmofpuberty,rapidgrowth, phys-iologic changes and are usually engaged in socialization processes,asanyother adolescent.That said,the manage-mentofchronicdiseasesduringthisspecialperiodconstitutes amajorchallengefortheindividual,his/herfamilyandthe health-careteam.
Thefirstsexualintercoursehasbeingoccurringatearlier agesthroughouttheworld.3,4Adolescentswhoinitiatesexual
activityearlyinlifetendtohavemoresexualpartnersandare morepronetounintendedpregnancies,sincethisbehavior isgenerallyassociatedwithlowfrequencyofcontraceptive use.4,5
Althoughrates ofteenagepregnancy have declined sig-nificantlyinmostcountriesduringthelastdecades,alarge numberofpregnanciesstilloccurinthisagegroup.Around16 millionadolescentwomen(15–19years old)givebirtheach year,approximately 11%ofallbirthsworldwide.6 The2014
WorldHealth Statisticsshows thattheaverage globalbirth ratebetween15and19yearoldsis49per1000girls.7
Adolescentsappeartobeathigherriskforadverse preg-nancyoutcomes,suchaslow-birth-weightbabiesandinfant deaths.6,8–10Amulticountrystudythatincluded124,446
moth-ers ≤24 years, revealed that the risk of adverse outcome
remained increasedin adolescent (≤19 years) comparedto
young mothers after controlling for country, marital sta-tus, education levels and parity.10 Undesired pregnancies
may endinabortions,whichare usuallyunsafeinthisage group.
Pregnancyinadolescentswithchronicmedicalconditions hasbeenrarelystudied,althoughitisanimportantissuein clinicalpractice.Sexualdesireispresentinyouth, indepen-dentlytheseverityofapossiblechronicillness.11Pregnancy
canalsobeparticularlyriskyinfemaleadolescentwithactive diseaseorunderteratogenicmedication,making contracep-tionanimportantissueforthesewomen.
Despite adolescentcontraception hasbecomean impor-tantpublichealthissue,mostphysiciansarestillnotaware ofthenecessitytoprovidetherightinformationandsupport pregnancyprevention.12Effectivecontraceptionisparticularly
important foradolescents withchronic diseases,since the consequencesofanunwantedandunwishedpregnancycan bedevastating.
Inadolescent withchronicautoimmuneconditions, dis-easeactivity atthetimeofconceptionandthepresenceof antiphospholipid antibodies (aPL) are responsible formost complications. Diseaseflares,pre-eclampsia, and thrombo-sis constitute maternal complications in adolescent with systemiclupuserythematosus(SLE),whereasfetalloss, pre-maturebirthandintrauterinegrowthrestrictionarethemain fetalcomplications.Teratogenicdrugs,suchas immunosup-pressiveagents,impliestheuseofcontraceptives.13
rightstoconfidentialreproductivehealthcare,sexual func-tion and contraceptive methods. Contraception should be discussedineach medicalvisitwithadolescent andyoung patients.Arecentstudyshowedthatapproximately30–55% offemalepatientsinreproductiveagewithchronic inflam-matorydiseasesreportedthattheirconcernsrelatingtofamily planningwerenotadequatelyaddressedduringtheirmedical appointments.14
Cochrane Database study reviewed more then 41 tri-als(including morethat 95,000teens) and concluded that the combination of education and contraception promo-tion was highly successful in pregnancy prevention for adolescents.15
ThemostrecentYouthRiskBehaviorSurveillanceinUSA reportedthat41%ofhighschoolstudentsdidnotusea con-domand14%didnotuseanycontraceptivemethodsduring thelastsexualintercourse.16Therefore,totakeadailypillmay
bechallengingandothersurveyreportedthatteensaremore thantwiceaslikelytoexperienceapillfailureaswomenaged morethan30years.17
Afterthe contraceptivechoice,it ismandatoryto evalu-ateprospectivelythepossibleadverseeventsandadherence for this strategy. These are important issues and may be highlighted, particularly in adolescents with chronic diseases.
EligibilityCriteriaforContraceptiveUse,18currentlyinits
5th edition (2015), is a document published by the World HealthOrganization(WHO)whichincludesscientificevidence toguidedecisionmakingonthesafetyoftheuseofvarious contraceptivesinwomenwithoverthan 60medical condi-tions. In 2010, the Centers for Disease Control (CDC) also publishedadocumentforuseintheUSA,includedother med-icaldiseasesnotincludedintheWHOrecommendationsas bariatricsurgery,solidorgantransplantandotherchronic dis-eases,suchasinflammatoryboweldiseaseandrheumatoid arthritis.19 Bothdocumentscoversthe currentfamily
plan-ningmethods.17,18
Thebothguidelinesclassifiedcontraceptivemethodsfor various diseasesin 1–4categories: category1includes dis-easeswithoutrisktocontraceptiveuse;category2includes somemedicalrisktocontraceptive;category3risksusually outweighcontraceptivebenefitsandcontraceptivemethods arecontraindicatedincategory4.18,19
Theobjectiveofthisarticleisareviewregarding contra-ceptionforadolescentswithchronicautoimmunediseases.
Methods
We performed a narrative review and conducted a series of literature searches in the database MEDLINE/PubMed for English language articles focusing on contraception in adolescents with rheumatic diseases. The search strat-egy included a combination of medical subject headings and keywords. The search terms that we used were “con-traception”, “adolescent”, “combined oral contraceptive”, “pediatricautoimmunediseases”,“juvenileidiopathic arthri-tis”(JIA), “juvenilerheumatoidarthritis”,“juvenilesystemic lupuserythematosus”(JSLE),“childhood-onsetsystemiclupus erythematosus”, “antiphospholipid syndrome” (APS) and
Table1–Tenbasicprinciplesforchoosingan
appropriatecontraceptivestrategyforadolescentswith rheumaticchronicdiseases.
1. Consideradolescentwithrheumaticchronic diseaseasanindividualwithsexualdesires, shapedbytheirconditionandwithsexualand reproductiverights
2. Respectthebioethicalprinciplesofprivacyin careandconfidentialityofinformation 3. Adoptastrategyof“dualprotection”to preventionofpregnancyandsexually transmittedinfectionswithcondom 4. Considerthepracticaleffectivenessofeach
contraceptivemethodandunderstandthe typicaladolescentuse(nottheperfectuse) 5. Considertheeligibilitycriteriaofeachmethod
foreachclinicalcondition,consultingexisting guidelines(WHOorCDC)
6. Understandingtheadverseeffectsofthe methods,druginteractionanditspossible interferenceindiseaseprogression 7. Consideraccessibilityandavailabilityof
contraceptivemethodinthehealthsystemand thecostofmethod.
8. Assesstheteenager’sattitudetowardsthe exerciseoftheirsexuality,theirquestionsand myths
9. Encouragethepresenceandparticipationofthe partnerandtheexistenceoffamilyand/orsocial supportnetworktotheissueofcontraception 10. Developstrategiestotheteenagecouple.Healthy
providersareencouragedtohelpthenegotiation ofcontraceptiveusewithbothpartners
WHO,WorldHealthOrganization;CDC,CentersforDiseaseControl.
“juvenile dermatomyositis”. The search coveredthe period between1970and2015andincludedclinicalstudies, system-aticreviewsandanimalstudies.Allarticlesselectedforthis manuscriptwerefull-textorreviewpapers.
Table1includestheprinciplesforchoosinganappropriate
contraceptivestrategyforadolescentswithrheumaticchronic diseases.
Contraception
for
juvenile
systemic
lupus
erythematosus
JSLE isachronicautoimmune diseasethatcaninvolve any systemandmayleadtosignificantmorbidityandmortality. Approximately15–20%ofSLEhavediseasebefore18yearsof age.20Sexuallyactiveadolescentswithlupusareathighrisk
forpregnancy.Inadditiontopsychosocialrisksrelatedtoearly pregnancyinthelifeofateenager,risksforwomenwithSLE includediseaseflares,obstetricandfetalcomplications,and adverseeffectsofmedicationsonfetaldevelopment.14
A cohort of women with SLE reported a high risk for unplannedpregnancy,includingmanypatientsunder terato-genicmedications,59%reportednocontraceptivecounseling withinthepastyearand53%usedonlybarriercontraceptive methods.21
knowledge,thereis nostudy ofcontraceptivemethods for JSLEadolescents.Thisisaveryimportantpointtoconsider, since JSLE adolescents have a more severe disease course than adult-onsetSLE.Therefore, theyare prone todevelop significant damage due to the disease, comorbidities and treatments.22–24
According to the WHO and CDC guidelines,18,19 barrier
methodsformalecontraceptioncanbesafelyusedbypatients withSLE(category1).Thecondomuseshouldbereinforcedfor allmalepatients,especiallyunderbiologicaland immunosup-pressiveagents.Nonetheless,thesemethodshavehighfailure rateswhenusedasthe singlecontraceptivemethod, espe-ciallyinteenagers.15Thus,itismandatorytoindicateamore
reliablemethodinconjunctionwithbarriermethodstoavoid pregnancy.
Regardinghormonaltherapies,oneoftheconcernsabout combined oralcontraceptives(COC) toSLEpatients isthat estrogenseemstoplaya majorrolein lupus pathophysio-logy.JSLEoftenoccursinpost-pubertaladolescent,supporting thenotionthatSLEcanbeinducedbyestrogen.Indeed,some autoimmuneeffectsofestrogenshavebeenrelatedinvitro, suchasenhancedT-cellresistancetoapoptosisandincreased levelsofautoreactiveBcells.25,26
Despite the common use of COC, many physicians are reluctanttoprescribethiscontraceptivetofemaleSLEdueto concernsthatexogenousestrogenscouldprovokelupusflare. Anotherissueisthatestrogenhasbeenassociatedwitheither venousorarterialthrombosis.27
TheSELENA(SafetyofEstrogensinLupus Erythematosus-NationalAssessment)trialstudied183youngadultfemaleSLE patients,aged18years oldormore,withinactiveor stable disease.Previoushistoryofthrombosis,positivityfor anticar-diolipinantibodiesorlupusanticoagulantandhypertension wereexclusioncriteria. COCdidnotincreasetheincidence ofsevereormild/moderateflareswhencomparedtoplacebo. ThisstudyreinforcedsafetyofCOCforasubgroupoffemale SLEwhohadmild,stablediseaseandwithout antiphospho-lipidantibodies.28
Sanchez-Guerreroetal.29 studied162adultwomenwith
SLE in three different groups to evaluate the influence of contraceptive methods (COC, progestin-only pill or copper intrauterinedevice).Therewerenodifferencesbetweenthese groupsindiseaseactivity.Duringthestudyfourpatientshad thrombotic events,two in the COCs group and two inthe progestin-onlypillgroup.
AssociationbetweenCOCuseandvenousthrombosishad beenreported.30WHOandCDCguidelinessuggestthatCOCs
inthepresenceofantiphospholipidantibodiesarestrictly pro-hibitiveforSLEpatients(category4).Ontheotherhandfor otherSLEpatients,eventhosewithseverethrombocytopenia orimmunosuppressivetreatment,thismethodisclassifiedas category2.Itisimportanttonote thatforallcategories of SLE,classificationsarebasedontheassumptionthatnoother riskfactorsforcardiovasculardiseasearepresentandthese classificationsmustbemodifiedinthepresenceofsuchrisk factors.18,19 COC prescription iscontraindicated forarterial
hypertension(systolic>160ordiastolic>100mmHg)(category 3).18,19
MatureadolescentswithSLEwithnegative antiphospho-lipid antibodies,who are nonsmokers, withneither family
nor personal history of thrombosis and with the disease controlled, without renal involvement, may be eligible for COC. To minimize the risk of thrombotic events, a low-estrogenformulationshouldbechosen.31,32Nevertheless,the
majorityofadolescentswithlupusdonotpresentallthe pre-viouscharacteristics,thereforetheyarenotgoodcandidates forestrogen-containingcontraception,andotheralternatives shouldbeconsidered.31,32
Regardingprogestincontraceptive,Mintzetal.33reported
progestogen use in SLE patients, either intramuscular norethisteroneenanthateororallevonorgestrel.These contra-ceptiveswereconsideredtolerablemethods,inspiteof30%of thepatientshadexperiencedintermenstrualbleedings,which ledtomedicationwithdrawal.33 Inaddition,Julkunen etal.
alsoobservedhighwithdrawalrates(78%)ofprogestin-only pill(POP)preparationinSLEpatientsduetopoorgynecological tolerance,seeminglyvaginalbleeding.34
Alargeretrospectivestudywithmorethan74,000women that received progestogen presented augmented risks of thrombosis. However,the relativeriskwas muchhigherin women who used progestogens dueto another indication, but notasacontraceptionmethods.35 Researchaddressing
thromboticriskofprogestin-onlymethodsinhighrisk popu-lationsarenotavailable.
WHOrecommendsthatPOParesafeinthemajorityofSLE patients,eveninthepresenceofseverethrombocytopeniaor immunosuppressivedrugs(category2).Ifapatienthas posi-tiveantiphospholipidantibodies,themethodisclassifiedas category3.18Themainconcernrelatedtotheuseby
adoles-centsispooradherenceduetomenstrualirregularity. Depot medroxyprogesterone acetate (DMPA) injections, every three months, is a highly effective contraception method. However,ithas beenobservedthat long-termuse ofDMPAisassociatedwithdecreasedbonemineraldensity (BMD), although with no known association with fracture risks.ThedecreaseinBMDinhealthyadolescentsmaynotbe clinicallysignificant,neverthelessforateenagerwithlupus, whohaveanincreasedriskofosteopeniaduetoeitherdisease itselforchronicglucocorticoiduse,itmightbeaconcern.32
Supplementation ofcalcium and vitamin D isrequiredfor adolescentsunderDMPA.36
More recently, an implantable device with etonogestrel (subdermal implant), another progestin-only contraceptive method,canbeanoptionforfemaleSLE.Menstrual irregu-laritiesaredescribed,althoughthisimplantdoesnotappear tohaveaneffectonBMD.ThismethodisclassifiedinWHO guidelinewiththesamecategoriesforDMPA.
Long-acting reversible contraception (LARC) includes intrauterinedevices(IUDs)andsubdermalimplant.Although these methods are considered as one of the most effec-tivereversiblecontraceptionstrategies,traditionallyarenot offeredroutinelytotheadolescentpopulation.Thisconcept, however, hasbeen modifiedinrecentyears.Approximately 4.5%ofAmericangirls15–19yearsusesomeofthesemethods, mostlytheIUDs.37Recently,theAmericanCollegeof
Inadditiontothecontraceptivebenefits,theuseofLARC ensure optimal rates of adherence, an important parame-tertobeconsidered,particularlyinadolescentswithchronic diseases. Studies have demonstrated high rates of contin-uationofuse withthese methods, surpassing85%over 12 monthsbothin youngerwomen and older.39 This method
combinedwiththeuseofcondomsarealsorelevanttoreduce riskofsexuallytransmitteddiseasesandHIVinfection. Cur-rentevidenceisthatIUDsaresafe.Therelativeriskofpelvic inflammatorydiseaseisincreasedonlyinthefirst20days fol-lowingthedeviceinsertion,equalingthebaselinepopulation afterthisperiod.40TheIUDswithprogestinmaydecreasethe
pelvicinflammatorydiseaseriskbecausethethickeningofthe cervical mucus and endometrialthinning. Pelvicinfections werenotobservedinadultSLEpatients,neitherhemorrhagic complicationswiththismethod.29,34
AccordingtotheWHO,thebenefitofusingcopperIUD (Cu-IUD)and levonorgestrel-IUD(LNG-IUD) inwomen withSLE underimmunosuppressivetreatmentusuallyoutweighsthe risks(category2),exceptforpatientswithsevere thrombocy-topenia(category3forCu-IUDand2forLND-IUD).LNG-IUD forpatientswithantiphospholipidantibodieshasahighrisk (category3).18
Therefore, physiciansshould be consideringlong-acting reversibleandhighly-effectivecontraception,suchimplants and intrauterinedevices,forappropriatelyselected adoles-centswithSLE.
Contraception
for
antiphospholipid
syndrome
APSisan autoimmunedisorder characterizedby the pres-enceofantiphospholipidantibodiesandthrombosis.Itmay occurasanisolatedclinicalentityorinassociationwithother diseases,mainlySLE.
Lakasing and Khamashta41 found seven thrombotic
episodesin32COCusers(22%)innon-pregnantwomenwith APSwithout any additionalriskfactors.This ismorethan twicetheriskofthrombosisinnon-pregnantwomenwithAPS, withoutanyadditionalriskfactors.Thesedatasuggestthat womenwithAPSshouldnotusethisformofcontraception.
Someauthorshaveobservedanincreasedprevalenceof antiphospholipidantibodies inhealthy womenduringCOC therapy,predominantlyattheexpenseofanti-2-glycoprotein IIgGclass.42
InarandomizedstudyofSanchez-Guerreroetal.,29women
who used combined or progestin-only oral contraception had the same rateof thrombosis(2 of54 patients ineach group),andall4patientswiththrombosishadlowtitersof antiphospholipidantibodies.29 Asherson et al.43 described
10patientswithaPLdevelopingvascularcomplicationswhile takingCOCs.
APS is a well-characterized prothrombotic condition. Nevertheless, physicians’ ability to predict the risk of thromboembolicphenomenaforanasymptomatic antibody-positiveindividual isstilllimited. Theassociation between high dose of estrogen and venous thromboembolism has beenknownfordecadesandsomestudiesshowthat estro-gens and progestogensare thoughtto beimportantinthe
pathogenesisofarterialthrombosis.27,31,32Therefore,useof
COC exerts anadditive effect on therisk ofthrombosisin these patients, many ofthem mightnot beaware oftheir genetic phenotype. The combination of antiphospholipid antibodyandgeneticprothromboticriskfactorsincreasesthe riskofthrombosis.Eventhoughthisincreaseinrisk,routine screening in patientswithout apersonal or family history ofthrombosisbeforestartingCOCisnotrecommended.18It
isreasonabletoassumethatthefrequencyofthrombosisin womentakinghormonalcontraceptionisincreasedifthere isalreadyapredispositiontothromboembolicdisease, espe-ciallyinwomenwithunderlyingthrombophilias(congenital oracquired)andadditionalriskfactors.
Other risk factors for arterial events, like complicated migraines, atherosclerosis or hyperlipidemia, might be increasedinSLEpatientswithantiphospholipidantibodies, andcouldalsoincreaseriskofstrokeormyocardialinfarction. Asaresult,substantialconcernhasbeenexpressedregarding theprescriptionofCOCtosuchwomen.Itseemsreasonable toavoidCOC inall patientswithpositiveantiphospholipid antibodies.43–46
Recent systematic review and meta-analysis was con-ductedtoevaluatetheriskofvenousthromboembolicevents associated with the use of progestin-only contraception. The summary measure for the adjusted relative risk of a venous thromboembolic episode for users versus non-users ofa progestin-only contraceptive was, based on the randomeffectsmodel,1.03(95%CI0.76–1.39).Subgroup anal-ysis confirmed there was no association between venous thromboembolic risk and POP or a progestin intrauterine device.46
TheWHOguidelineconsiderstheuseofprogestogen-only pillsforSLE,category3forpatientswithpositive antiphos-pholipidantibodies,similartotheCDCguideline.18,19
DMPAcould beatherapeuticalternative toCOC in ado-lescents with antiphospholipid antibodies, since progestin onlycontraceptivesareassociatedwithalower,ifnotabsent, riskofvenousthromboembolicdisease.47DMPAmaycause
reversibleosteoporosisandthefertilitycouldbedelayedafter discontinuation. TheWHOguideline considersinitiation or continuationofDMPAforSLE, category3forpatientswith positive antiphospholipid antibodies.18 Similarly, the CDC
guidelineconsidersasacategory3thestartofDMPAforSLE withantiphospholipidantibodies(orunknown),aswellasthe continuationofthemethod.19
Other authorsalsoreportedthe safetyofDMPAfor con-traceptioninfemaleswithantiphospholipidantibodies.48In
addition,womenwithAPSunderwarfarinshouldhave ovula-tionsuppressedwithintramuscularDMPAtodecreasesevere hemorrhagic corpus luteum complicating anticoagulation. Hemorrhagicsitereactionwasnotobservedwiththis contra-ceptiveusingthisrouteofadministration.49
A notable decrease in menstrual blood flow is seen with medroxyprogesterone acetate and the levonorgestrel-releasing intrauterine system IUDs which might be par-ticularly beneficial in patients receiving treatment with warfarin.50
CompoundsofprogestinsandIUDsshouldbeusedwith cau-tion,mainlyinanticoagulatedadolescents andwithriskof reductionBMD.
Contraception
for
other
chronic
rheumatic
diseases
Toourknowledge,therewasnostudyregardingsafetyand efficacyofcontraceptioninjuvenileidiopathicarthritis pop-ulation. Britto et al.51 studied adolescent risky behaviors,
including sexual activities, in 178 patients with pediatric-onsetrheumaticdiseases,69%ofthemhadJIA.Sixtypercent ofthefemalesweresexuallyactiveand41%wereusing con-domsastheonlycontraceptivemethod.
Moreover,arecentAustralianstudy showedhigherrates ofmaternalmorbidity,pre-eclampsiaandpostpartum hem-orrhage in JIA patients.52 Therefore, it is of the utmost
importance to inform the need of contraceptive methods toavoidunplanned pregnancies. Rheumatoidarthritis(RA) wasadded asa newconditionspecific tothe USAcontext intheCDC adaptationofthe medicaleligibilitycriteria for contraceptiveuse fromWHO.19 Accordingtothisguideline,
theuseofcombinedhormonalcontraceptiveforrheumatoid arthritis (with or without immunosuppressive therapy) is category2.CDCrecommendsthatPOPissafeinRApatients (category1);DMPAisconsideredcategory2/3inpatientson immunosupressive therapy.LARC (LNG-IUD andCu-IUD) is a good option for rheumatoid arthritis patients (category 1) without immunosuppressive treatment; is considered category2forinitiation andcategory 1forcontinuationin patients on immunosuppressive treatment.19 JIA was not
includedintheWHOguidelines.PatientswithJIA,especially under immunosuppressive treatment, may possibly use
contraceptive recommendations such rheumatoid arthritis. However further studies regarding safety and efficacy of contraceptioninJIApatientswillbenecessary.
The risk of pregnancy loss and prematurity have been reportedinpatientswithinflammatorymyopathies.53
How-ever,toourknowledge,therewasnostudyregardingsafety and efficacy of contraception in juvenile dermatomyositis population.TheWHOandCDCguidelinesdidnotinclude con-traceptionfordermatomyositis.
Emergency
contraception
Although the eligibility criteria for contraceptive methods prescriptionfromWHO18andCDC19discusstheuseof
com-bination pills or others non-hormonal methods for some clinicalconditions,theemergencycontraception(EC)wasnot includedintheserecommendations.
ECwithorallevonorgestrelisawellunderstood,ethically and technicallylegitimatemechanismforemergency situa-tions, whereno other protectionmethod was used. Ithas no medicalcontraindicationsand therefore canbeusedin adolescentswithrheumaticchronicdiseases,includingthose withcontraindicationtoCOC.54,55
EC withorallevonorgestrel shouldbeused after unpro-tected sex.Itiseffectivewhenstartedlessthan 120hafter sexual activity.54 To improve compliance, the single-dose
levonorgestrel-onlytreatmentisindicated.
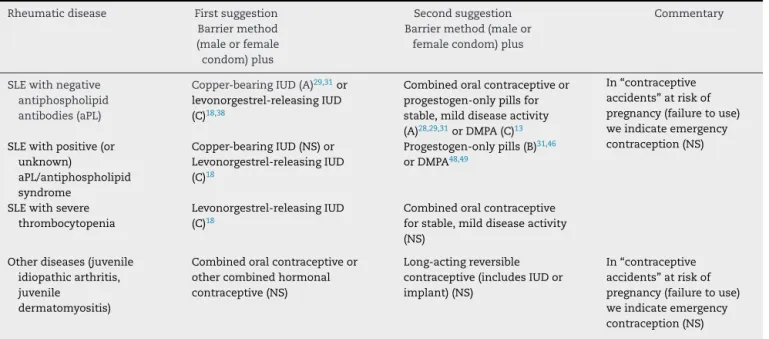
Table2illustratesthecontraceptivemethod
recommenda-tionsandlevelsofevidence56foradolescentswithrheumatic
chronicdiseases.
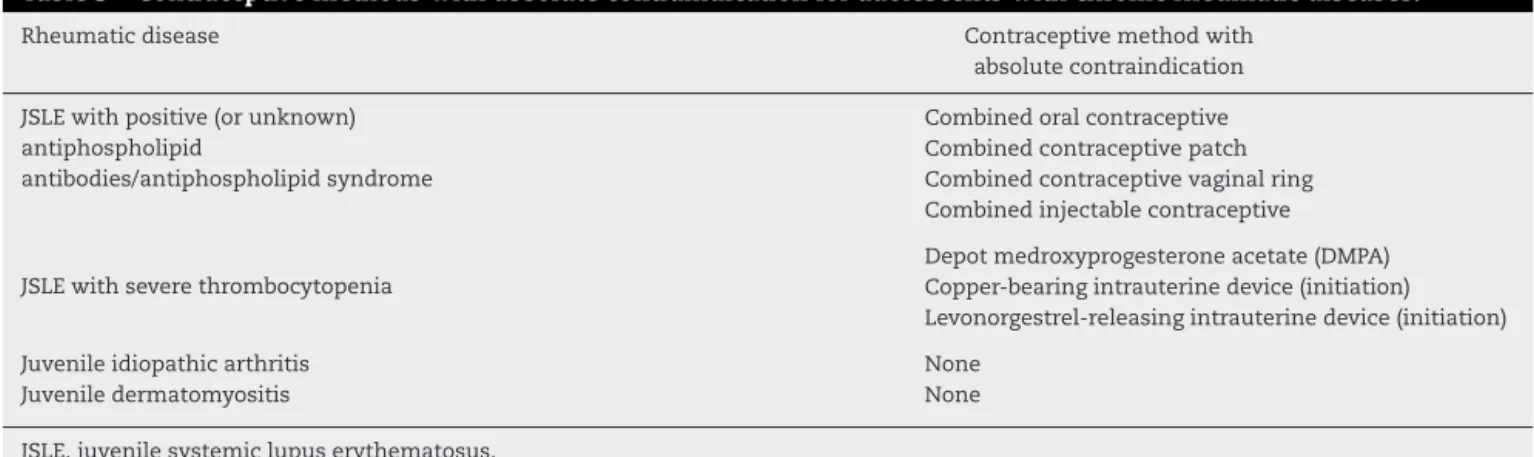
Table3showscontraceptivemethodswithabsolute
con-traindicationforadolescentswithchronicrheumaticdiseases.
Table2–Contraceptivemethodrecommendationsandlevelsofevidenceforpatientswithchronicrheumaticdiseases.
Rheumaticdisease Firstsuggestion Barriermethod (maleorfemale condom)plus
Secondsuggestion Barriermethod(maleor
femalecondom)plus
Commentary
SLEwithnegative antiphospholipid antibodies(aPL)
Copper-bearingIUD(A)29,31or
levonorgestrel-releasingIUD (C)18,38
Combinedoralcontraceptiveor progestogen-onlypillsfor stable,milddiseaseactivity (A)28,29,31orDMPA(C)13
In“contraceptive accidents”atriskof pregnancy(failuretouse) weindicateemergency contraception(NS) SLEwithpositive(or
unknown)
aPL/antiphospholipid syndrome
Copper-bearingIUD(NS)or Levonorgestrel-releasingIUD (C)18
Progestogen-onlypills(B)31,46
orDMPA48,49
SLEwithsevere thrombocytopenia
Levonorgestrel-releasingIUD (C)18
Combinedoralcontraceptive forstable,milddiseaseactivity (NS)
Otherdiseases(juvenile idiopathicarthritis, juvenile
dermatomyositis)
Combinedoralcontraceptiveor othercombinedhormonal contraceptive(NS)
Long-actingreversible contraceptive(includesIUDor implant)(NS)
In“contraceptive accidents”atriskof pregnancy(failuretouse) weindicateemergency contraception(NS)
Table3–Contraceptivemethodswithabsolutecontraindicationforadolescentswithchronicrheumaticdiseases.
Rheumaticdisease Contraceptivemethodwith
absolutecontraindication
JSLEwithpositive(orunknown) antiphospholipid
antibodies/antiphospholipidsyndrome
Combinedoralcontraceptive Combinedcontraceptivepatch Combinedcontraceptivevaginalring Combinedinjectablecontraceptive
JSLEwithseverethrombocytopenia
Depotmedroxyprogesteroneacetate(DMPA) Copper-bearingintrauterinedevice(initiation) Levonorgestrel-releasingintrauterinedevice(initiation)
Juvenileidiopathicarthritis None
Juveniledermatomyositis None
JSLE,juvenilesystemiclupuserythematosus.
Conclusion
Adolescenceisa periodto consolidateidentity,developing apositivebodyimage, toestablishsocialrelationshipsand toachieveindependenceandsexualidentity.Cliniciansmust understandthathavingpediatricrheumaticillness,evenwith disability,doesnotpreventtheiryouthfrom beingsexually active,becomingpregnant,orcontractingsexually transmit-teddiseases.Thepreventionofteenagepregnancyiscomplex anddynamicandthepopulationofyoungpeoplewithaccess toareliable sourceofinformation,adviceand supportare betterprepared toexercise ahealthy and responsible sex-uality. Based in our experience and to best adherence in youngpatients,werecommendthatthecontraceptivechoice forrheumatologicchronic disease should be prescribed by theirownrheumatologistsandeventuallywithagynecologist supervision.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
ThisstudywassupportedbygrantsfromFundac¸ãodeAmparo à Pesquisa do Estado de São Paulo (FAPESP 2009/51897-5, 2011/12471-2and2014/14806-0toCAS),ConselhoNacionalde DesenvolvimentoCientíficoeTecnológico(CNPQ 302724/2011-7toCAS),FedericoFoundation(toCAS),andNúcleodeApoio àPesquisa“SaúdedaCrianc¸aedoAdolescente”daUSP (NAP-CriAd)toCAS.
r
e
f
e
r
e
n
c
e
s
1. WHO.Theadolescentwithachroniccondition;2007. Availablefrom:http://www.who.int/maternalchild
adolescent/documents/9789241595704/en/[accessed
15.06.15].
2. NationalSurveyofChildren’sHealth.NSCH2011/12.Data queryfromthechildandadolescenthealthmeasurement
initiative,dataresourcecenterforchildandadolescent healthwebsite.Availablefrom:http://childhealthdata.
org/browse/survey/results?q=2473&r=1&g=448[accessed
07.06.15].
3.PiresR,Araújo-PedrosaA,PereiraJ,CanavarroMC.Preventing
adolescentpregnancy:biological,social,andpolitical
influencesonageatfirstsexualintercourse.JPrimary
Prevent.2014;35:239–54.
4.Oliveira-CamposM,GiattiL,MaltaD,BarretoSM.Contextual
factorsassociatedwithsexualbehavioramongBrazilian
adolescents.AnnEpidemiol.2013;23:629–35.
5.ShafiiT,StovelK,HolmesK.Associationbetweencondomuse
atsexualdebutandsubsequentsexualtrajectories:a
longitudinalstudyusingbiomarkers.AmJPublicHealth.
2007;97:1090–5.
6.WHO.WHOguidelinesonpreventingearlypregnancyand poorreproductiveoutcomesamongadolescentsin
developingcountries;2011.Availablefrom:http://whqlibdoc.
who.int/publications/2011/9789241502214eng.pdf?ua=1
[accessed10.06.15].
7.WHO.Adolescentpregnancy.FactSheet364.Availablefrom:
http://www.who.int/mediacentre/factsheets/fs364/en/
[accessed05.06.15].
8.ParanjothyS,BroughtonH,AdappaR,FoneD.Teenage
pregnancy:whosuffers?ArchDisChild.2009;94:239.
9.MalabareyOT,BalaylaJ,KlamSL,ShrimA,AbenhaimHA.
Pregnanciesinyoungadolescentmothers:a
population-basedstudyon37millionbirths.JPediatrAdolesc
Gynecol.2012;25:98–102.
10.GanchimegT,OtaE,MorisakiN,LaopaiboonM,Lumbiganon
P,ZhangJ,etal.Pregnancyandchildbirthoutcomesamong
adolescentmothers:aWorldHealthOrganization
multicountrystudy.BJOG.2014;121:40.
11.GreydanusDE,PrattHD,PatelDR.Conceptsofcontraception
foradolescentandyoungadultwomenwithchronicillness
anddisability.DisMon.2012;58:258–320.
12.HartmanLB,MonasterioE,HwangLY.Adolescent
contraception:reviewandguidanceforpediatricclinicians.
CurrProblPediatrAdolescHealthCare.2012;42:221–63.
13.SilvaCA,HilarioMO,FebronioMV,OliveiraSK,AlmeidaRG,
FonsecaAR,etal.Pregnancyoutcomeinjuvenilesystemic
lupuserythematosus:aBrazilianmulticentercohortstudy.J
Rheumatol.2008;35:1414–8.
14.ChacravartyE,ClowseME,PushparajahDS,MertensS,
GordonC.Familyplanningandpregnancyissuesforwomen
withsystemicinflammatorydiseases:patientandphysician
perspectives.BMJOpen.2014;4:e004081.
15.OringanjeC,MeremikwuMM,EcoH,SeuE,MeremikwuA,
amongadolescents.CochraneDatabaseSystRev. 2009;4:CD005215.
16.KannL,KinchenS,ShanklinSL,FlintKH,KawkinsJ,Harris
WA,etal.,CenterforDiseaseControlandPrevention.Youth
RiskBehaviorSurveillance—UnitedStates,2013.MMWR.
2014;63:1–168.
17.KostK,SinghS,VaughanB,TrusselJ,BankoleA.Estimatesof
contraceptivefailurefromthe2002NationalSurveyofFamily
Growth.Contraception.2008;77:10–21.
18.WHO.Medicaleligibilitycriteriaforcontraceptiveuse.5thed. Geneva:WHO;2015.Availablefrom:http://www.who.int/
reproductivehealth/publications/family
planning/Ex-Summ-MEC-5/en/.
19.CentersforDiseaseControlandPrevention.Medicaleligibility
criteriaforcontraceptiveuse,2010.AdaptedfromtheWorld
HealthOrganizationmedicaleligibilitycriteriafor
contraceptiveuse,4thedition.MMWR.2010;59:1–86.
20.SilvaCA,AvcinT,BrunnerHI.Taxonomyforsystemiclupus
erythematosuswithonsetbeforeadulthood.ArthritisCare
Res(Hoboken).2012;64:1787–93.
21.YazdanyJ,TrupinL,KaiserR,SchmajukG,GillisJZ,
ChakravartyE,etal.Contraceptivecounselinganduseamong
womenwithsystemiclupuserythematosus:agapinhealth
carequality?ArthritisCareRes.2011;63:358–65.
22.SilvaCA,HilárioMO,FebrônioMV,OliveiraSK,TerreriMT,
SacchettiSB,etal.Riskfactorsforamenorrheainjuvenile
systemiclupuserythematosus(JSLE):aBrazilianmulticentre
cohortstudy.Lupus.2007;16:531–6.
23.TuckerLB,UribeAG,FernándezM,ViláLM,McGwinG,Apte
M,etal.Adolescentonsetoflupusresultsinmoreaggressive
diseaseandworseoutcomes:resultsofanestedmatched
case–controlstudywithinLUMINA,amultiethnicUScohort
(LUMINALVII).Lupus.2008;17:314–22.
24.GormezanoNW,SilvaCA,OtsuziCI,BarrosDL,daSilvaMA,
SallumAM,etal.Higherprevalenceanddistinctfeaturesof
herpeszosterinfectioninchildrenthanadultswithsystemic
lupuserythematosus.PediatrInfectDisJ.2015;34:905–7.
25.PetriM.Sexhormonesandsystemiclupuserythematosus.
Lupus.2008;17:412–5.
26.GrimaldiCM.Sexandsystemiclupuserythematosus:therole
ofthesexhormonesestrogenandprolactinontheregulation
ofautoreactiveBcells.CurrOpinRheumatol.2006;18:
456–61.
27.StegemanBH,deBastosM,RosendaalFR,vanHylckamaVlieg
A,HelmerhorstFM,StijnenT,etal.Differentcombinedoral
contraceptivesandtheriskofvenousthrombosis:systematic
reviewandnetworkmeta-analysis.BMJ.2013;347:5298.
28.PetriM,KimMY,KalunianKC,GrossmanJ,HahnBH,
SammaritanoLR,etal.Combinedoralcontraceptivesin
womenwithsystemiclupuserythematosus.NEnglJMed.
2005;353:2550–8.
29.Sanchez-GuerreroJ,UribeAG,Jiménez-SantanaL,
Mestanza-PeraltaM,Lara-ReyesP,SeucAH,etal.Atrialof
contraceptivemethodsinwomenwithsystemiclupus
erythematosus.NEnglJMed.2005;353:2539–49.
30.WorldHealthOrganizationCollaborativeStudyof
CardiovascularDiseaseandSteroidHormonalContraception.
Venousthromboembolicdiseaseandcombinedoral
contraceptives:resultsofinternationalmulticenter
case–controlstudy.Lancet.1995;346:1575–82.
31.CulwellKR,CurtisKM,delCarmenCraviotoM.Safetyof
contraceptivemethoduseamongwomenwithsystemic
lupuserythematosus:asystematicreview.ObstetGynecol.
2009;114:341–53.
32.TesherMS,WhitakerA,GilliamM,Wagner-WeinerL,OnelKB.
Contraceptionforadolescentswithlupus.PediatrRheumatol
OnlineJ.2010;8:10.
33.MintzG,GutiérrezG,DelezéM,RodríguezE.Contraception
withprogestogensinsystemiclupuserythematosus.
Contraception.1984;30:29–38.
34.JulkunenHA,KaajaR,FrimanC.Contraceptivepracticein
womenwithsystemiclupuserythematosus.BrJRheumatol.
1993;32:227–30.
35.VasilakisC,JickH,Melero-MontesMM.Riskofidiopathic
venousthromboembolisminusersofprogestogensalone.
Lancet.1999;354:1610–1.
36.CromerBA,ScholesD,BerensonA,CundyT,ClarkMK,
KaunitzAM,SocietyforAdolescentMedicine.Depot
medroxyprogesteroneacetateandbonemineraldensityin
adolescents–TheBlackBoxwarning:apositionpaperofthe
SocietyforAdolescentMedicine.JAdolescHealth.
2006;39:296–301.
37.FinerLB,JermanJ,KavanaughMC.Changesinuseof
long-actingcontraceptivemethodsintheUnitedStates,
2007–2009.FertilSteril.2012;98:893–7.
38.McNicholasC,PeipertJF.Long-actingreversiblecontraception
foradolescents.CurrOpinObstetGynecol.2012;24:293–8.
39.PeipertJF,ZhaoQ,AllsworthJE,PetroskyE,MaddenT,
EisenbergD,etal.Continuationandsatisfactionofreversible
contraception.ObstetGynecol.2011;117:1105–13.
40.MohllajeeAP,CurtisKM,PetersonHB.Doesinsertionanduse
ofanintrauterinedeviceincreasetheriskofpelvic
inflammatorydiseaseamongwomenwithsexually
transmittedinfection?Asystematicreview.Contraception.
2006;73:145–53.
41.LakasingL,KhamashtaM.Contraceptivepracticesinwomen
withsystemiclupuserythematosusand/orantiphospholipid
syndrome:whatadviceshouldwebegiving?JFamPlann
ReprodHealthCare.2001;27:7–12.
42.VadS,LakosG,KissE,SipkaS,CsorbaR,PokaR.
Antiphospholipidantibodiesinyoungwomenwithand
withoutoralcontraceptiveuse.BloodCoagFibrinolys.
2003;14:57–60.
43.AshersonRA,HarrisEN,HughesGRV,FarquharsonRG.
Complicationsoforalcontraceptivesandantiphospholipid
antibodies.ArthritisRheum.1988;31:575–6.
44.ChoojitaromK,VerasertniyomO,TotemchokchyakarnK,
NantirujK,SumethkulV,JanwityanujitS.Lupusnephritisand
Raynaud’sphenomenonaresignificantriskfactorsfor
vascularthrombosisinSLEpatientswithpositive
antiphospholipidantibodies.ClinRheumatol.2008;27:
345–51.
45.WahlDG,GuilleminF,deMaistreE,PerretC,LecompteT,
ThibautG.Riskforvenousthrombosisrelatedto
antiphospholipidantibodiesinsystemiclupus
erythematosus–ameta-analysis.Lupus.1997;6:467–73.
46.ManthaS,KarpR,RaghavanV,TerrinN,BauerA,ZwickerJI.
Assessingtheriskofvenousthromboemboliceventsin
womentakingprogestin-onlycontraception:ameta-analysis.
BMJ.2012;345:e4944.
47.TincaniA,NuzzoM,LojaconoA,CattaliniM,MeiniA.
Contraceptioninadolescentswithsystemiclupus
erythematosus.Lupus.2007;16:600–5.
48.YamakamiL,SerafiniP,deAraujoD,BonfáE,LeonE,Baracat
E,etal.Ovarianreserveinwomenwithprimary
antiphospholipidsyndrome.Lupus.2014;23:862–7.
49.YamakamiLY,deAraujoDB,SilvaCA,BaracatEC,deCarvalho
JF.Severehemorrhagiccorpusluteumcomplicating
anticoagulationinantiphospholipidsyndrome.Lupus.
2011;20:523–6.
50.SchaedelZE,DolanG,PowellMC.Theuseofthe
levonorgestrel-releasingintrauterinesysteminthe
managementofmenorrhagiainwomenwithhemostatic
51.BrittoMT,RosenthalSL,TaylorJ,PassoMH.Improving
rheumatologists’screeningforalcoholuseandsexual
activity.ArchPediatrAdolescMed.2000;154:478–83.
52.ChenJS,FordJB,RobertsCL,SimpsonJM,MarchLM.
Pregnancyoutcomesinwomenwithjuvenileidiopathic
arthritis:apopulation-basedstudy.Rheumatology(Oxford).
2013;52:1119–25.
53.VancsaA,PonyiA,ConstantinT,ZeherM,DankóK.
Pregnancyoutcomeinidiopathicinflammatorymyopathy.
RheumatolInt.2007;27:435–9.
54.AmericanAcademyofPediatricsCommitteeonAdolescence.
Emergencycontraception.Pediatrics.2012;130:
1174–82.
55.ArmstrongC.ACOGrecommendationsonemergency
contraception.AmFamPhysician.2010;82:1278.
56.HadornDC,BakerD,HodgesJS,HicksN.Ratingthequalityof
evidenceforclinicalpracticeguidelines.JClinEpidemiol.