www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Immediate
effects
of
an
anchor
system
on
the
stability
limit
of
individuals
with
chronic
dizziness
of
peripheral
vestibular
origin
夽
Almir
Resende
Coelho
a,∗,
Ana
Paula
do
Rego
Andre
b,
Júlia
Licursi
Lambertti
Perobelli
b,
Lilian
Shizuka
Sonobe
b,
Daniela
Cristina
Carvalho
de
Abreu
baUniversidadedeSãoPaulo(FMRP-USP),FaculdadedeMedicinadeRibeirãoPreto,ProgramaemReabilitac¸ãoeDesempenho
Funcional,RibeirãoPreto,SP,Brazil
bUniversidadedeSãoPaulo(FMRP-USP),FaculdadedeMedicinadeRibeirãoPreto,RibeirãoPreto,SP,Brazil
Received5October2015;accepted21December2015 Availableonline29March2016
KEYWORDS
Posturalbalance; Vestibulardiseases; Dizziness;
Hapticinformation
Abstract
Introduction:Thesymptomsassociated withchronicperipheralvestibulopathy exerta nega-tiveimpactontheindependenceandqualityoflifeoftheseindividuals,andmanyindividuals continuetosufferfromthesesymptomsevenafterconventionalvestibularrehabilitation. Objective: Toevaluatetheacuteeffectofananchorsystemforbalanceevaluationofpatients withchronicdizzinesswhofailedtorespondtotraditionalvestibularrehabilitation.
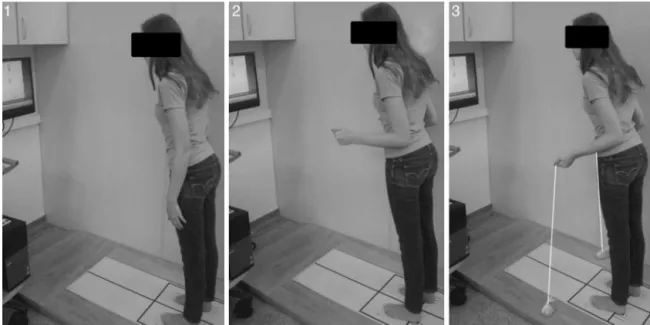
Methods:Subjectsover50yearsofage,presentingwithchronicdizzinessandpostural instabil-ityofperipheralvestibularorigin,participatedinthestudy.Thelimitofstabilitywasevaluated inthreepositionsusingtheBalanceMaster®system:Position1,standingwiththearmsalong
thebody;Position2,standingwiththeelbowsbentat90◦ (simulatingholdingtheanchors); andPosition3,withtheelbowsbentat90◦ holdingtheanchors.Thevariablesofmovement latency,endpointexcursionanddirectionalcontrolofmovementwereevaluated.
Results:Usingtheanchorsystem,significantreductionoftimeintheresponseatthebeginning ofthemovementcomparedtoPosition1(p<0.05);increasedendpointexcursionintheleft lateraldirectioncomparedtoPosition1(p<0.05);andmoredirectionalcontrolofmovement intheanteriorandposteriordirections(p<0.05)comparedtotheotherpositions,werefound.
夽 Pleasecitethisarticleas:CoelhoAR,doRegoAndreAP,PerobelliJL,SonobeLS,deAbreuDC.Immediateeffectsofananchorsystem
onthestabilitylimitofindividualswithchronicdizzinessofperipheralvestibularorigin.BrazJOtorhinolaryngol.2017;83:3---9. ∗Correspondingauthor.
E-mail:[email protected](A.R.Coelho).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2015.12.008
Conclusion:Whileusingthesystemanchor,individualswithchronicperipheralvestibulopathy showedanimmediateimprovementinthestabilitylimitinrelationtothemovementlatency, endpointexcursion,anddirectionalcontrolofmovementvariables,suggestingthatthehaptic informationaidsposturalcontrol.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Equilíbriopostural; Doenc¸asvestibulares; Tontura;
Informac¸ãoháptica
Efeitosimediatosdeumsistemadeâncorasnolimitedeestabilidadedeindivíduos comtonturacrônicadeorigemvestibularperiférica
Resumo
Introduc¸ão:Ossintomasassociadosàvestibulopatiaperiféricacrônicatêmimpactonegativo naindependênciaequalidadedevidadosindivíduos,emuitosdelescontinuamasofrerdesses sintomas,mesmodepoisdeterempassadopelareabilitac¸ãovestibularconvencional.
Objetivo:Avaliaroefeitoagudodeumsistemadeancoragemparaavaliac¸ãodoequilíbriode pacientescomtonturacrônicaquenãoresponderamàreabilitac¸ãovestibulartradicional. Método: Indivíduoscommaisde50anosqueseapresentaramcomtonturacrônicae instabili-dadeposturaldeorigemvestibularperiféricaparticiparamnoestudo.Olimitedeestabilidade foiavaliadoem trêsposic¸ões,comousodosistemaBalanceMaster®:Posic¸ão1, depécom
osbrac¸ospendentesaolongodocorpo;Posic¸ão2,depécomoscotovelosflexionadosem90◦ (simulandoaposic¸ãodesegurarasâncoras);ePosic¸ão3,comoscotovelosflexionadosem90◦ esegurandoasâncoras.Foramavaliadasasvariáveisdelatênciademovimento,pontofinalda excursãoecontroledirecionaldomovimento.
Resultados: Com o uso do sistema de âncoras, ocorreu reduc¸ão significante no tempo de respostanoiníciodomovimentoemcomparac¸ãocomaPosic¸ão1(p<0,05);aumentonoponto finaldaexcursãonadirec¸ãolateralesquerda,emcomparac¸ãocomaPosic¸ão1(p<0,05);emais controledirecionaldomovimentonasdirec¸õesanterioreposterior(p<0,05),emcomparac¸ão comasdemaisposic¸ões.
Conclusão:Enquantousavamosistemadeâncoras,osindivíduoscomvestibulopatiaperiférica demonstraram melhoraimediata nolimite daestabilidadeem relac¸ãoàs variáveislatência demovimento,pontofinaldaexcursãoecontroledirecionaldomovimento,sugerindoquea informac¸ãohápticaauxilianocontrolepostural.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
The majority of symptoms reported by elderly people, suchasdizziness,posturalinstability,gaitdisturbancesand fallingincidents,1 canbetheconsequencesof several
dis-easesoriginatinginthevestibularsystem.2Thesevestibular
systemdisordersareasignificantprobleminhealthcare. Dizzinessisprevalentin5---10%oftheworld’spopulation, anditistheseventhmostfrequentcomplaintinwomenand thefourthmostfrequentinmen.Approximately47%ofmen and61%ofwomenoverage70yearsareaffectedby dizzi-ness.Dizzinessoccursin65%ofsubjectsaged65yearsand older who livein the community and in 81---91% of those of the same age who are treated at geriatric outpatient clinics.3
The deterioration of vestibularfunction leadtofalling andhasmanyconsequences,includingphysicalimpairments (tissueinjuries,gaitchanges);psychologicalchanges(fearof falling,depression);socialchanges(isolation,dependency); andeconomicchanges(medicationcosts,rehabilitation).
Posturalcontrol,acomplexabilitythatinvolvespostural orientation and the maintenance of balance, depends on centralprocessinginputsrelatedtovisual,vestibular,and somatosensory afferent mechanisms,4 and to the
propor-tional neuromuscularaction of efferent mechanisms.The informationrelatedtovisual,vestibular,andsomatosensory systems should be integrated and selected in accordance withtheenvironmentandthetypeoftasktobeperformed inordertomaintainposturalstability.5
Inpatientswithvestibulardisorders,disturbancesof sen-sorial integrationor information processingthat generate conflictamongthevisual,vestibularandsomatosensory sys-temsmaybepresent,whichcouldexplainthepermanency of symptoms of chronic vestibular disorder, such as the inability tomodulatesensoryinformationin awaythat is adequatetoensureposturalbalance.2
oftherapycharacterizedbyitsphysiologicalactiononthe vestibular system, which acts on the central mechanisms of neuroplasticitytogenerate adaptation,habituation, or replacement mechanisms in the vestibular system and to relievevestibularsymptoms.6
It is believed that VR can promote healing in 30% of cases and can achieve other positive results in 85% of individuals.7Therefore,itisimportanttosearchfor
effec-tivewaystoimproveotoneurologicsymptomsandtoprevent falls,aswellasforclinicallyviableassessmentsthatcanbe introducedinthedailyclinicalpracticeforthispopulation. Mauerberg-Decastro8developedaninstrumentaimedat
improvingcorporalstabilitycalledtheanchorsystem,which works as a mediator of haptic information between the ground and the participant’s body. The haptic system, or touchfeedback,worksthroughtheactiveexplorationofthe environment(staticor dynamic),whichinvolvesthe inter-pretation of spatiotemporal stimuli as they interact with severaltypesofmechanoreceptors.9
Theanchorsystemcanhelpthevestibularsystemachieve anew adjustmentof sensorymechanismsand/or improve the somatosensory system through the conflict reduction of information processing, which contributes to balance improvement.Therefore,thisstudyaimedtoevaluatethe acuteeffectsoftheanchorsystem forbalance evaluation intheupright position(limitofstability)onsubjectswith chronic dizzinessof peripheral vestibularorigin whohave notrespondedtotraditionalVR.
Methods
Sampleandsetting
Thesamplewascomposedofsubjectsover50yearsofage ofbothsexeswhopresentedwithchronicdizzinessand bal-anceinstabilityofperipheralvestibularoriginastheirmain complaint.
These patients were admitted to Otorhinolaryngology Outpatient Clinic of the Department of Ophtalmology, OtorhinolaryngologyandHeadandNeck Surgery,Schoolof Medicine,UniversityofSãoPaulo(FMRP-USP),inthecityof RibeirãoPreto,stateofSãoPaulo,Brazil,wheretheywere diagnosedbyadoctorspecializinginOtorhinolaryngology.
Patientswithchronic dizzinessof peripheral vestibular origin(i.e.,withsymptomsthathad occurredfor atleast threemonths afterthe firstepisode withnotreatment)10
werereferredtotheDepartmentofSpeechTherapy,where theyweretreatedwithconventional VR.Patientswhodid not respondpositively torehabilitation for at least three monthswerereferredtotheLaboratoryofAssessmentand Rehabilitation of Equilibrium (LARE) toparticipate in this study.
The eligibility criteria included subjects of both sexes over 50yearsofage diagnosedwithchronic dizzinessand decreased posturalbalance ofperipheral vestibularorigin unspecifieddizzinessorsensationsofdizzinesswith periph-eral etiology daily, weekly, and monthly episodes for at leastsix months;andsymptoms ofvertigo, dizziness, and lack of postural stability that did not respond positively to conventional VR, including the reorganization of the vestibulo-ocularreflex(VOR).
Included (30)
Man (0)
Woman (30)
Evaluated (40)
Excluded (10)
Man (3)
Central Vestibular
(2)
MMSE low** (1)
Woman (7)
*VR (4)
MMSE low** (3)
Figure 1 Flowchart ofthe sample (*VR, conventional ves-tibular rehabilitation in progress; **MMSE, Mini-Mental State Examination).
Theexclusioncriteriafortheresearchincludedpatients whoreceiveddrugs (benzodiazepinesandanticonvulsants) thataffectbalanceorcalciumchannelblockers(cinnarizine andflunarizine)thosewhoshowedrestrictedmobility,visual restriction, and cognitive constraint that precluded the developmentoftheassessmentsandinterventionproposed orthosewhopresentedwithsystemicdiseaseswithoutany drugcontrol.Thosewhodidnotmeettheeligibility crite-riaordidnotagreetoparticipateintheprotocolreceived guidelineswithregardtotheimportanceofbalance reha-bilitationthroughphysiotherapeuticcare(Fig.1).
The Mini-Mental State Examination (MMSE) was used to exclude those who presented with cognitive impairments.3,11
This cross-sectional study was approved by the Ethics CommitteeonHumanResearchoftheRibeirãoPreto Clin-icsHospitalMedicineSchool,UniversityofSãoPaulo,Brazil, protocolN.3350/2013.Allparticipantswereinformedabout thestudy andagreedtoparticipatebyprovidinginformed consent.
Outcomemeasures
Thebalanceassessmentwasperformedduringthelimitof stability(LOS)testusingtheBalanceMaster®system (Neuro-comInternational,Inc.,Clackamas,OR,UnitedStates).12---14
The LOS test is a dynamic test that analyzes an indi-vidual’s ability to move the center of pressure (COP) in predetermineddirectionsbyaskingthevolunteerto trans-ferhisweightasfar ashecan in eightpre-setdirections aroundhiscentralaxis,usingtheanklestrategyinsteadof thehip,andwithoutchangingthesupportbase.These tar-getsarerepresentedonthemonitor,inrealtime,infront oftheindividualineightpointsarrangedinacircle.Each pointisseparatedintoanglesof45◦andatadistancefrom
Figure2 PositionsadoptedduringevaluationsusingtheBalanceMaster®equipment.Position1,standingwiththearmsalongthe body;position2,standingwiththeelbowsbentat90◦ (simulatingholdingtheanchors);andposition3,withelbowsbentat90◦
holdingtheanchors.
stabilitylimitpreviouslycalculatedbythemachine,based on the individual’s height. In this study, the points were establishedand represented bythe numbers 1 (anterior), 3(leftlateral),5 (posterior),and 7(right lateral)to rep-resent COP displacement in the anterior---posterior and medial---lateraldirections.
ToavoidinadequateposturalstrategiesfortheLOStest, whichisnotintuitive,15allparticipantswereallowed5min
tobecomefamiliarwiththeplatformandweregivenvisual feedback andguidelines regarding strategies for COP dis-placementduringthemovementstobeperformed.
The individual was evaluated in three positions: posi-tion1, standingwiththearmsalongthe body;position2, standingwiththeelbowsbentat90◦(simulatingholdingthe
anchors);andposition3,withtheelbowsbentat90◦holding
theanchors(Fig.2).Randomizationwasperformedto deter-minetheorderofthepositions.Therewasafiveminuterest periodbetweeneachposition.
Theanchorsystemisbasedonthedevelopmentofa non-rigid tool, which consists of flexible ropes attached to a weightontheextremitythattouchestheground; the vol-unteerholdstheropeintheoppositeextremity.8
Inthepositionwithanchorsusage,thevolunteerheldthe anchorstokeeptheflexiblecablesextendedandtheweight inconstantcontactwiththeground.
The variables of the LOS assessed were16 movement
latency(ML),averageinseconds(s)fromthevisual stimula-tiontothebeginningofthemovement;endpointexcursion (EPE), defined as the higher COP displacement in the first sustained movement in each direction, measured in displacementpercentageunderthepossiblemaximum dis-placement deemed to be 100%; and directional control of movement (DCM), defined as an individual’s ability to maintain the axis of movement parallel to the targeted axis,measuredasapercentagetocomparetheamountof intentionalmovement toward thetargetwiththe amount of corrective movement not directed toward the tar-get. This is calculated following the formula (intentional
movement−corrective movement/unintendedmovement) andisexpressedasapercentage(%).Ifallvoluntary move-mentisdirectedtothetargetinastraightline,theamount ofcorrectivemovementisequalto0andthescoreis100%; thedataobtainednearthisvalueareconsideredbetter.
Withthe aimof ensuringthe safety ofall assessments on the platform, the investigator in charge and an assis-tantstayed closetotheparticipanttopreventanyfalling episodesandobservedthemovementstrategiescarriedout bythevolunteersduringthetests.17
Samplesizecalculation
To calculatethesample size,GraphPadStatMatesoftware was used, and the variable of movement latency of the stability limit in the Balance Master® system was consid-eredaprimaryoutcome,whichresultedinsamplesize=17, power=0.9,and˛error=0.05.
Statisticalanalysis
Forthestatisticalanalysis,themeanvalueofeachvariable after conductingthreetrials in each movement excursion was considered. All data weresubjected toa descriptive analysisandnormalitytest(Shapiro---Wilk)usingSPSS® soft-ware,v.13.0.None ofthe datashownormaldistribution, so thestatistical inference was performed usingthe non-parametric test (Kruskal---Wallis)to comparethe different positions withand without the useof the anchor system. Thelevelofsignificancewasconsideredtobe95%basedon Tukey’sposthoctest.
Results
Table1 Anthropometriccharacteristicsoftheevaluated sample.
Variables Average±SD(n=30)
Age(years) 64.65±8.69
Bodymass(kg) 72.57±7.66
Height(m) 1.61±0.05
BMI(kg/m2) 28.14±3.65
BMI,bodymassindex.
The following datadescribetheLOS test, inwhich the positionswereselectedtorepresenttheanterior-posterior (1and5)andmedial-lateral(3and7)oscillations.
FortheML variable,theanteriordisplacementwas sig-nificantlylowerwiththeuseoftheanchorsystemcompared totheotherpositionsevaluated(Table2).
Thepointofmaximumexcursion(EPE)wasgreaterwhen usingtheanchorthaninposition1,whichdidnotuse the anchorandplacedthearmsalongthebodyontheleftlateral direction(Table3).
There wasgreater directional control(values closerto 100%)duringthedisplacementintheanteriorandposterior directions(p<0.05) with theuse of anchors comparedto otherpositions,whichmeansthatthevolunteerhadgreater motioncontrolwhendirectingtowardtheanteriorand pos-teriortargetsafterperformingfewercorrectivemovements duringtheroutine(Table4).
Discussion
The literature has shown that the better the postural balance, the better the functional capacity of subjects withchronicperipheralvestibulardisorders;converselythe greatertheimpairmentoffunctionalcapacity,thegreater theriskoffallsinthesesubjects.16
Peripheralvestibulopathycancreateachronic dysfunc-tion condition in which activities performed in a given environment can cause conflicting sensoryafferents, par-ticularly when they require greater postural control that affectsthestabilitylimitoftheindividual.
The LOS hasbeen evaluatedtoidentifydeficits of bal-anceinindividualswithchronicperipheralvestibulopathy.16
Studies haveevaluatedthe LOS bycomputerized posturo-graphytoassessthefunctionalstabilityofindividualswith vestibulardysfunction,which enablestheidentificationof possiblechangesintheellipticalareaandoscillationspeed ofthepressurecenter.18---20
In2010, asystematicreviewbyRiccietal.,whichwas related to VR in middle-aged and elderly adults, found thatinadditiontotheclassictestevaluationofstaticand dynamicbody balance,computedposturographywasused inmoststudies,particularlyintheLOStest ofthelatency of movement, maximum excursion point, and directional controlofthemovementvariables.20
Themeanageinthepresentstudypopulationwas64.6 years.According topublishedfindings,some authors indi-cate age as a possible factor for the loss of vestibular functionduetoelectrophysiologicalandstructuralchanges in the vestibular system, which can have important con-sequencesfor posturalcontrolasearly as40yearsofage
andcancausemultipleotoneurologicalsymptoms,suchas dizziness.21,22
In addition, the prevalence of female subjects in the presentstudyconfirmswhathasalreadybeendescribedin theliterature, thatdizziness ismore prevalentin women at a ratioof 2:1.An organic predispositionfor vestibular disorders may be related to an intrinsic hormonal varia-tionand/ormetabolicdisorders,andwomensufferthemost falls.23---25
Thepresentstudyobservedimmediatebenefitsofusing the anchor system in improving the LOS, particularly regardingtheincreaseoftheleftlateraldisplacementwith improved anterior and posterior directional control and loweranteriorlymovement latency,accordingtotheEPE, DCM,andMLvariables,respectively.
Thus,theanchorsystem’sfunctionasamediatorofthe hapticinformationbetweenthegroundandtheuser’sbody mightbebeneficialtoimprovebalanceperformance.9,26
Moreover,thissystemprovidesinformationaboutforce, motion,texture,andshape(acceleration,gravitational,and inertial)involvedinmechanicalperceptionofthe environ-mentthroughtheskinandkinestheticsystemefforts,such asthe touchof afinger withsome static toreduce body oscillation.26
The benefits of the anchor system werealso observed in the study of Freitas et al.11 in healthy elderly
individ-ualswhousedtheanchorsystem.Subjectsweredividedinto threegroups accordingtofrequency ofuseofthe anchor-ingsystem(0%,50%,and100%)inthestandingposition.The limitedperiodofsessionsat50%improvedposturalcontrol comparedtotheuseoftheanchorsystemforalongertime. Theauthorssuggestedthatthisresultwasduetothe hap-ticinformationbeingusedbythecentralnervoussystemas awaytorecalibratetheprocessofsensoryintegrationfor improvedposturalcontrol.15
Usingtheanchorsystem, thevolunteersin thepresent studywereabletomove theCOPmore inleftlateral dis-placement(EPE) compared to conditionswithout anchors andwiththearmalongthebody.
Thus, the anchor system can be an important tool in rehabilitationofbodybalanceprograms,becausea reduc-tioninthestabilitylimitinindividualswithposturalcontrol impairmentsmaycausedifficultywhenperformingreaching tasksintheorthostaticposition,suchaspickingupobjects, orevenwhentheindividualisimpactedby someexternal force.16Thesmallerthestabilitylimit,theworseisthe
abil-ityoftheindividualtomovewithoutchangingthesupport base, making him or her more susceptible toinjury from falls.17
Regarding the ML, the subjects in this study took less timetostartmovementintheanteriordirectionusingthe anchorsystemcomparedtoconditionswithoutanchorsand withthearmalongthebody.Thiscanberelatedtothefact thatwhenusingtheanchorsystem,theindividualmayfeel agreaterconfidencetomovetowardthetargets,usingthe hapticsystemasan adjuncttopostural controlsystem to keeptheCOPwithinthestabilitylimitwithoutchangingthe supportbase.
Table2 Meanandstandarddeviationofthevariablemovementlatency(ML)ofthestabilitylimit,inseconds.
Variables Position1 Position2 Position3 p-value
1×3 2×3
ML(1)seg 1.23±0.40 1.64±0.65 1.15±0.47 0.003a 0.003a
ML(3)seg 1.23±0.47 1.81±0.98 1.51±0.46 0.19 1.0
ML(5)seg 0.91±0.55 1.30±1.07 0.85±0.51 1.0 0.57
ML(7)seg 1.23±0.42 1.60±0.77 1.30±0.29 1.0 0.36
ML(1),anteriordisplacement;ML(3),rightlateraldisplacement;ML(5),posteriordisplacement;ML(7),leftlateraldisplacement. Position1,standingwiththearmsalongthebody;position2,standingwithelbowsbentat90◦(simulatingholdingtheanchors);and
position3,elbowsbentat90◦holdingtheanchors.1×3,position1vs.position3;2×3,position2vs.position3.
aSignificantdifference(p<0.05)accordingtotheKruskal---Wallistestofmultiplecomparisons.
Table3 Meanandstandarddeviationofthevariableendpointexcursion(EPE)ofthestabilitylimit,asapercentage.
Variables Position1 Position2 Position3 p-value
1×3 2×3
EPE(1)(%) 61.75±19.10 58.93±10.21 58.86±22.49 1.0 1.0
EPE(3)(%) 67.70±19.42 74.40±18.22 71.98±22.99 1.0 1.0
EPE(5)(%) 58.56±21.79 60.13±18.23 53.12±13.42 1.0 0.72
EPE(7)(%) 59.21±18.20 77.56±18.11 73.94±20.15 0.01a 1.0
EPE(1),anteriordisplacement;EPE(3),rightlateraldisplacement;EPE(5),posteriordisplacement;EPE(7),leftlateraldisplacement. Position1,standingwiththearmsalongthebody;position2,standingwiththeelbowsbentat90◦(simulatingholdingtheanchors);and
position3,elbowsbentat90◦holdingtheanchors.1×3,position1vs.position3;2×3,position2vs.position3.
aSignificantdifference(p<0.05)accordingtotheKruskal---Wallistestofmultiplecomparisons.
therefore performingthe COPdisplacement withas little correctionofmovementaspossible.
In2011,thestudybyIzquierdoetal.subjectedelderly patientswithchronicperipheralvestibulardiseasetoa reha-bilitationprogramofbodybalancebasedoncomputerized dynamicposturography,notinganimprovementof13.8%in theDCMvariableof thestabilitylimit aftertwoweeksof training.18 This was similar to the finding of the present
study,in which the anchor system showed an immediate improvementof10.06%indirectionalmovementcontrol.
Theimmediatepositiveeffectobtainedusingtheanchor systeminsubjectswithvestibulardisorderwhodidnotshow improvement after conventional VR suggests that it is a toolthatcanbeusedasatherapeuticstrategyforbalance improvementthroughrecalibrationofthesensorysystems, mainlysomatosensory.
As this is a relatively new way of exploring haptic informationtoimproveposturalcontrolinindividualswith chronic peripheralvestibulopathy,thephysiological mech-anism and ways in which the anchorsystem can improve posturalcontrol intheseindividualshave notbeen exten-sivelyexploredintheliterature.
However,ifwecomparetheuseofanchorswith biofeed-back modalities as a method of training for improved posturalcontrol,wecanfollowthetheoryofHorak,which suggeststhat sensoryinformationprovidedfrequently can be understood by thepostural control system asan addi-tionalsensorysystemandmaybeusedorfurtherexplored tothedetrimentofanothersystemthatisatadisadvantage orinaccurate.25
Thisstudyis relevantindemonstratingthattheanchor systemcanimprovethestabilitylimitoftheindividualwith
Table4 Mean and standarddeviation ofthe variable directional controlof movement (DCM) ofthe stability limit, as a percentage.
Variables Position1 Position2 Position3 p-value
1×3 2×3
DCM(1)(%) 84.02±8.45 83.56±5.33 88.85±4.08 0.03a 1.0
DCM(3)(%) 86.63±4.81 81.38±4.61 80.15±7.53 1.0 1.0
DCM(5)(%) 68.82±22.81 63.34±20.71 78.88±7.99 0.001a 0.01a
DCM(7)(%) 78.21±14.06 85.36±3.81 87.12±4.82 0.01 1.0
DCM(1),anteriordisplacement;DCM(3),rightlateraldisplacement;DCM(5),posteriordisplacement;DCM(7),leftlateraldisplacement. Position1,standingwiththearmsalongthebody;position2,standingwiththeelbowsbentat90◦(simulatingholdingtheanchors);and
position3,elbowsbentat90◦holdingtheanchors.1×3,position1vs.position3;2×3,position2vs.position3.
chronicvestibulardysfunction,whichcan assistinposture controland canbe usedinexercise protocolsfor balance rehabilitation.
Conclusion
Theanchorsystem,byusinghapticinformationforpostural control,providedanimmediateimprovementinthestability limit inindividuals withchronic peripheral vestibulopathy whohadnotrespondedtoVR.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
The authors would like toacknowledge the financial sup-portoftheSupportFoundationtheEducationandAssistance ResearchHospitaldasClinicasofmedicineofRibeirãoPreto, UniversityofSãoPaulo(FAEPA)careissue.Supportofteam Prof.PhDCamilaGiacomoCarneiroBarrosof Otorhinolaryn-gologyOutpatientClinicoftheDepartmentofOphtalmology, OtorhinolaryngologyandHeadandNeck Surgery,Schoolof Medicine,UniversityofSãoPaulo(FMRP-USP),inthecityof RibeirãoPreto,stateofSãoPaulo,Brazil.
References
1.TinettiME,WilliamsCS,GillTM.Health,functional,and psycho-logicaloutcomesamongolderpersonswithchronicdizziness.J AmGeriatrSoc.2000;48:417---21.
2.Gananc¸aMM,CaovillaHH,Gananc¸aFF,DonáBrancoF,Paulino CA.Comotrataravertigem.RevBrasMed.2008;65:6---14. 3.GazzolaJM,Gananc¸a FF, ArataniMC,Perracini MR, Gananc¸a
MM.Clinicalevaluationofelderlypeoplewithchronicvestibular disorder.BrazJOtorhinolaryngol.2006;72:515---22.
4.GünendiZ,SepiciDinc¸elA,Erdo˘ganZ,AknarO,YanpalS,Gö˘güs¸ F,etal.Doesexerciseaffecttheantioxidantsysteminpatients withankylosingspondylitis.ClinRheumatol.2010;19:1143---7. 5.HerdmanSJ.Reabilitac¸ãovestibular.2nded.SãoPaulo:Manole;
2002.
6.GanancaFF, GazzolaJM, GanancaCF, Caovilla HH, Gananca MM,CruzOL. Elderlyfallsassociatedwithbenignparoxysmal positionalvertigo.BrazJOtorhinolaryngol.2010;76:113---20. 7.Gananc¸aFF,Gananc¸aCF.Reabilitac¸ãovestibular:princípiose
técnicas.In:Gananc¸aMM,MunhozLSM,CaovillaHH,SilvaMLG, editors.Estratégiasterapêuticasemotoneurologia.SãoPaulo: Atheneu;2001.p.33---54.
8.Mauerberg-DecastroE.Developingananchorsystemtoenhance posturalcontrol.MotorControl.2004;8:339---58.
9.Mauerberg-deCastro E, Calve T, Viveiros FF, Polanszyck SD, CozzaniMV.Umtutorialsobrepercepc¸ãohápticanocontrole postural:ilustrandoum sistema âncoraesuas aplicac¸ões na reabilitac¸ãoenaatividadefísica adaptada.Revista Sobama. 2003;8:7---20.
10.Handa PH, Kuhn MB, Cunha F, Dorigueto RS, Gananc¸a FF. Quality oflife inpatients withbenignparoxysmal positional vertigo and/or Ménière’s disease. Braz J Otorhinolaryngol. 2005;71:776---83.
11.FreitasMD,Mauerberg-DecastroE,MoraesR.Intermittentuse ofananchorsystemimprovesposturalcontrolinhealthyolder adults.GaitPosture.2013;38:433---7.
12.Martin M, Shinberg M, Kuchibhatla M, Ray L, Carollo JJ, Schenkman ML. Gait initiation in community-dwelling adults withParkinson’sdisease: comparisonwitholderand younger adultswithoutthedisease.PhysTher.2002;82:566---77. 13.NewtonRA.Validityofthemulti-directionalreachtest:a
prac-ticalmeasureforlimitsofstabilityinolderadults.JGerontol ABiolMedSci.2001;56:248---52.
14.Rossi-IzquierdoM,Santos-PérezS,Soto-VarelaA. Whatisthe mosteffectivevestibularrehabilitationtechnique inpatients withunilateralperipheralvestibulardisorders?EurArch Otorhi-nolaryngol.2011;268:1569---74.
15.DeCastroSM,PerraciniMR,Gananc¸aFF.DynamicGaitIndex ---Brazilianversion.BrazJOtorhinolaryngol.2006;72:817---25. 16.MenesesSRF,BurkeTN,MarquesAP.Balance,posturalcontrol
and musclestrengthinosteoporoticelderly womenwithand withoutfalls.FisioterapiaePesquisa.2012;19:26---31. 17.RahalMA[dissertation]Comparac¸ãodoequilíbrioentreidosos
saudáveis praticantes e não praticantes de Tai Chi Chuan. São Paulo: Universidade de São Paulo, Faculdade de Medi-cina; 2009. Available from: http://www.teses.usp.br/teses/ disponiveis/5/5140/tde-09122009-164929/[cited24.06.13]. 18.GhiringhelliR,Gananc¸aCF.Posturographywithvirtualreality
stimuliinnormalyoungadultswithnobalancecomplaints.J SocBrasFonoaudiol.2011;23:264---70.
19.YamamotoMEI,GanancaCF.Posturographywithvirtualreality stimuliindifferentvestibulardysfunctions.JSocBras Fonoau-diol.2012;17:54---60.
20.RicciNA,ArataniMC,DonáF,MacedoC,CaovillaHH,Gananc¸a FF. A systematic review about the effects of the vestibular rehabilitationinmiddle-ageandolderadults.RevBrasFisioter. 2010;14:361---71.
21.WhitneySL.Managementoftheelderlypersonwithvestibular dysfunction. In:Herdman S,editor. Vestibular rehabilitation, vol.10.UnitedStatesofAmerica:ContemporaryPerspectives Rehabilitation;2000.p.510---33.
22.Caovilla HH, Gananc¸a MM, Munhoz MSL,Silva MLG,Gananc¸a FF.Presbivertigem,presbiataxia,presbizumbidoepresbiacusia. In: SilvaMLG, Munhoz MSL,Gananc¸a MM, Caovilla HH, edit-ors.Quadrosclínicosotoneurológicosmaiscomuns.SãoPaulo: Atheneu;2000.p.153---8.
23.Gananc¸aMM,MunhozMSL,CaovillaHH,SilvaMLG,Gananc¸aFF, Perracini MR,et al. Conceitosealgoritmos terapêuticos.In: Gananc¸aMM,MunhozMSL,CaovillaHH,SilvaMLG,editors. Con-dutasnavertigem.SãoPaulo:GrupoEditoralMoreiraJr;2004. p.55---112.
24.HorakFB,ShupertC.Func¸ãodosistemavestibularnocontrole postural.In:Herdman SJ,editor.Reabilitac¸ãovestibular.São Paulo:EditoraManole;2002.p.25---51.
25.HorakFB. Posturalcompensation forvestibularloss.AnnNY AcadSci.2009;1164:76---81.