www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Open
fitting:
performance
verification
of
receiver
in
the
ear
and
receiver
in
the
aid
夽
,
夽夽
Maria
Fernanda
Capoani
Garcia
Mondelli
a,∗,
Tatiana
Manfrini
Garcia
b,
Fabiana
Midori
Tokuhara
Hashimoto
b,
Andressa
Vital
Rocha
baFaculdadedeOdontologiadeBauru,UniversidadedeSãoPaulo(FOB/USP),Bauru,SP,Brazil
bPhonoaudiology,FaculdadedeOdontologiadeBauru,UniversidadedeSãoPaulo(FOB/USP),Bauru,SP,Brazil
Received2January2014;accepted6April2014 Availableonline7September2014
KEYWORDS Hearingaids; Hearingloss; Speechperception; Noise
Abstract
Objective:Toverifythereceiverintheearandreceiverintheaidadaptationsbymeasuring
insituthespeechperceptionandusers’levelofsatisfaction.
Methods:The study was approved by the research ethics committee (Process: 027/2011). Twentysubjectsolderthan18 yearswithaudiologicaldiagnosisofmildandmoderate bilat-eraldescendingsensorineuralhearinglosswereevaluated.Thesubjectsweredividedintotwo groups,whereG1(group1)wasfittedwithopen-fithearingaidswiththebuilt-inreceiverunit (receiverintheear)andG2(group2)wasfittedwithopen-fithearingaidswithRITE.Aprobe microphonemeasurementwasperformedtocheckthegainandoutputprovidedbythe ampli-ficationandforassessmentofspeechperceptionwithHearinginNoiseTestwithandwithout hearingaids. Afteraperiodofsixweeksofusewithoutinterruption, thesubjectsreturned forfollow-upandansweredtheSatisfactionwithAmplificationinDailyLifequestionnaire,and wereagainsubjectedtoHearinginNoiseTest.
Results:Bothgroupspresentedbettertestresultsfor speechrecognitioninthepresenceof noise.
Conclusion:Groups1and2weresatisfiedwiththeuseofhearingaidsandimprovedspeech recognitioninsilentandnoisysituationswithhearingaids.
© 2014Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:MondelliMF,GarciaTM,HashimotoFM,RochaAV.Openfitting:performanceverificationofreceiverintheear
(RITE)andreceiverintheaid(RITA).BrazJOtorhinolaryngol.2015;81:270---5.
夽夽Institution:FaculdadedeOdontologiadeBauru(FOB/USP),Bauru,SãoPaulo,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](M.F.C.G.Mondelli). http://dx.doi.org/10.1016/j.bjorl.2014.08.013
PALAVRAS-CHAVE Auxiliaresdeaudic¸ão; Perdaauditiva; Percepc¸ãodafala; Ruído
Adaptac¸ãoaberta:verificac¸ãododesempenhoRITEeRITA
Resumo
Objetivo: Estudo clínico prospectivo para verificar as adaptac¸ões RITE e RITA por meio da mensurac¸ãoinsitudapercepc¸ãodafalaesatisfac¸ãodosusuários.
Método: Estudo aprovado peloCEP (Processo no 027/2011). Foram avaliados 20 indivíduos
maioresde18anoscomdiagnósticoaudiológicodeperdaauditivasensorioneuraldescendente bilateraldegrausleveemoderado.Osindivíduosforamdivididosemdoisgrupos,ondeoG1 (grupo1)foiadaptadocomAASIopen-fitcomreceptornopróprioaparelho(RITA)eoG2(grupo 2)foiadaptadocomAASIopen-fitcomreceptornocanal(RITE).Foirealizadaamedidacom microfone-sondaparaverificac¸ãodoganhoesaídadoAASIeavaliac¸ãodapercepc¸ãodafalacom
HearinginNoiseTest(HINT),semecomAASI.Apósumperíododeseissemanasdeusosem interrupc¸ões,oindividuoretornou paraacompanhamentoerespondeuaoquestionárioSADL (SatisfactionwithAmplificationinDailyLifeScale)erealizouoHINT.
Resultados: Osgruposapresentarammelhoresresultadosnotestedereconhecimentodafala compresenc¸aderuído.
Conclusão:Osgrupos1e2apresentaramsatisfac¸ãocomousodoAASIemelhorano reconhec-imentodefalanassituac¸õesdesilêncioeruídocomousodeAASI.
©2014Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Much has been discussed regarding the hearing aid (HA) adaptationinsubjectswithslopinghearingloss.1The
occlu-sioneffectisoneof theirmajorcomplaintsasdue tothe configurationoftheloss,whichisreportedasautophonia.
Consideringthetechnologicalevolutioninthe develop-mentofHAandtheparticularconfigurationofthehearing loss in these cases, open fit-specific mini behind-the-ear (BTE) devices provide benefits to these individuals. This model uses a shaft and a flexible adapter, and has an uniquecharacteristicof amplificationinmedium andhigh frequencies.2,3
These devices areknown asreceiver in the ear(RITE) whenthereceiverisusedintotheearcanalandconnected to the HA through a thin tube. Since the receiver is not locatedwithintheretroauriculardevice(BTE),thistypeof HAisparticularlysmallandmayhaveadvantagesregarding soundqualityandcomfort.Receiverintheaid(RITA)devices featurethereceiverintheHAitself.
Bothfittingandverificationshouldbeperceivedasa pro-cesswithamainobjective:theoptimumadaptationofthe individualtotheamplificationcharacteristics.Researchers4
havedevelopedaguidewherebytheverificationprocessby probemicrophonemeasurement ispart ofthe procedures foraproperHAfitting.Theprobemicrophonemeasurement isthepreferredmethodforverificationofHAinsitu.5
Probemicrophonemeasurementscanbeusedfor check-ingadjustmentsmadeintheHAandtoassesstheefficacyof specialcircuitssuchasnoisereducers,feedbackreducers, directionalmicrophones,andopen-fittingHA.6---8
The main aim of the adaptation of HA is to improve speech intelligibility, thus facilitating the communication process; hence the importance of testing the individual’s speechperception.9Withthisinvestigation,itispossibleto
obtainthethresholdofspeechrecognitionwithandwithout competitivenoisethroughtheHearinginNoiseTest(HINT),10
whichconsistsofaseriesof12listsof20sentenceswiththe sameextension, phoneticdistribution, and degree of dif-ficulty,which werenormatized so astopresent a natural aspectandreliability.
During the process of counseling hearing-impaired patients,thethreeprocessesof motivationrelatedtothe useofHAshould beconsidered:acceptance,benefit,and satisfaction.11 The success of the adaptation process of
amplificationdepends,amongotherfactors,onthe individ-ual’ssatisfactionwiththeresultsoftheuseofHA.12
Satisfactionistheoutcomemeasureofauditory rehabili-tationthatrepresentsthemostcomprehensivecombination of factors needed for the final result, since the variable ofinterestis thepointof viewoftheindividual,and itis not related only to the performance of HA,13 but rather
dependsexclusivelyontheperceptionsandattitudesofthe individual.14
The measurement of satisfaction with the use of HA in daily life has also been studied using the Satisfaction WithAmplificationinDailyLife(SADL)questionnaire.13This
tool wasdesigned toassess the satisfaction of HA users, quantifyingitthroughascoring processof foursubscales: positiveeffects, costs andservices, negativefactors,and self-image.15,16
Inthefieldofphonoaudiology,studiesthatcritically con-tributeto the process of HA fitting in centers accredited bythenationalpoliticsofhearinghealthcarearelacking.17
Thepresentstudyprioritizedtheevaluationofopen-fitting devicesusingobjectiveandsubjectivetoolsandfavoringthe optionsofRITEorRITA.
Methods
This was a prospective clinical study, conducted after approval by the Research Ethics Committee, process No. 027/2011.Allparticipantswereinformedaboutthe objec-tives and methodology of the proposed study, agreed to theproceduresnecessaryforconductingtheresearch,and signedaninformedconsent.
Forsamplecomposition,thefollowingeligibilitycriteria wereestablished: subjectsolder than 18years with audi-ologicaldiagnosis ofbilateralsensorineuralhearinglossat highfrequencies,ofmildtomoderatedegree,andwithno priorexperiencewithamplification.
Subjects with unilateral hearing loss or with previous experiencewiththeuse of HA;whodid notcontinue the processofadaptation;orwhodidnotagreetoparticipate inthestudywereexcluded.
The sample consistedof 20subjects, randomlydivided intotwogroups:group1(G1),usersofopen-fitHA adapta-tionwithRITE,and group2 (G2),userswithconventional open-fitHAadaptation(RITA).Bothgroupsconsistedoften subjectswithsimilarauditory characteristicsand commu-nicativeneeds.
The degree of hearing loss was classified using the audiometric thresholds at 500, 1000, 2000, and 4000Hz, rated as mild (average 26---40dB NH), moderate (average 41---60dB NH), severe (average of 61---80dB NH), and pro-found (average above 81dB NH), according to the World HealthOrganizationcriteria.18
The participants were bilaterally fitted with a Claris-Oticon HA device, with the same criteria of prescriptive method(NAL-NL1),whichhasasunderlyinglogicthe loud-ness equalization, i.e., the formula assumes that speech intelligibilitywillbe maximizedwhenall frequencybands areperceivedbytheuserashavingthesameloudness.
Attheconsultationfortheadaptationprocedure,aprobe microphonemeasurementofthegainandoutputprovided bytheamplificationwasperformed,inadditiontoan eval-uation of speech perception with and without HA. The procedurelastedapproximately90mininthisfirstphaseof thestudy.
Probemicrophonemeasurement
Probe microphone measurements were performed in a sound-proofroomwithadequatesize.Thepatientwas pos-itionedonemeterawayfromtheloudspeakerat0◦azimuth,
usingAffinity2.0(Interacustics)equipment.
Theinformationrelatedtospecifiedacoustic character-isticswith respect to the tubing type and olive size was inserted.Thefollowingmeasurementswereperformed:real earunaidedresponse(REUR),open-fitcalibration;realear occludedresponse(REOR),toverifyanypossibleocclusion oftheexternalauditorymeatus(EAM)bytheolive;andreal earaidedresponse(REAR).
The resonance response with the use of amplification (REAR)wasobtainedwithspeechnoisestimuliat50dBSPL, 65dBSPL,and80dBSPLintensities.
The values of REAR,at frequencies of 250, 500, 1000, 2000, 3000, 4000, and 6000Hz for input levels of 50, 65,and 80dB SPL,werecompared withtheNAL-NL1rule
targetsforweak,medium,andstrongsounds,respectively. The obtained responses were considered equivalentwhen thedifferencebetweenthetargettorealearinsertiongain (REIG) andthe realvalue obtained in ear didnot exceed 10dB.19
HearingInNoiseTest(HINT)
TheassessmentofspeechperceptionwasheldbytheHINT, adaptedforBrazilianPortuguese,20 underfourconditions:
- Sentences presented in silence: the HINT sentences adapted to Brazilian Portuguese were recorded at the HouseEarInstitute(LosAngeles,USA)byaBrazilian pro-fessionalactor.
- Speechwithfrontnoise(FN):20sentencesderivedfrom afrontallypositionedsoundbox(0◦)andpresented
simul-taneouslywithnoiseatafixedintensityof65dBNHinthe samefrontalbox(0◦).Acomposite-typenoisemaskerwas
used.
- Speechwithnoisetotheright(RN):20sentencesderived fromafrontallypositionedbox(0◦)withnoisepresented
atafixedintensityof65dBNHinaboxtotheright(90◦).
Acomposite-typenoisemaskerwasused.
- Speechwithnoisetotheleft(LN):20sentencesderived fromafrontallypositionedbox(0◦),withnoisepresented
atafixedintensityof65dBNHinaboxtotheleft(90◦).
Acomposite-typenoisemaskerwasused.
TheevaluationwasperformedwithoutHA,withHA,and six weeks after the adaptation. The acoustically-treated room andthe space allowed for theproper placement of theparticipant,examiner,andequipment.
After calibration of the system, the participant was instructed to remainin the same position throughout the test, ensuringthattheintensity that wouldreachtheear wouldbethesameasindicatedonthecomputerscreen.
Foreachcondition,alistof20sentenceswaspresented, andthelistwaschosenrandomlybytheHINTPROsoftware. Theparticipantswereinstructedverbally,accordingtothe guidelinescontainedintheHINToperatingmanual.
The sentence was considered correct by the examiner when all essential words were repeatedcorrectly. In this case,theexaminerpressedthe‘Yes’buttononthesoftware screen.When‘Yes’wasselectedafterthefirstpresentation, thesecondsentencewaspresented4dBbelowtheintensity ofthefirstsentence.
Forthetestconductedinsilence,thespeechlevelwas initiallysetat60dB.Therewasvariationinintensity accord-ing tothe responses of the participant--- if he/shefailed tocorrectlyrepeatthesentence,thelevelofpresentation wouldbeprogressivelyincreasedby4dB,untilthe partici-pantcouldrepeatthesentencecorrectly.
Thescoringforthetestconductedinsilence,definedas thethreshold ofrecognition of50% ofthesentences, was expressedindBNH.
signal-to-noise ratio after application of a list of 20 sentences,wasexpressedindB.Thus,thelowerthe signal-to-noise ratio, the better the speech perception of the participantinthiscondition.
Afteraperiodofsixweeksofuninterrupteduse,the par-ticipantreturnedtotheclinicforfollow-up.Atthisstage, he/she answered the SADL questionnaire administeredby theresearcher, in ordertoverifythe satisfactionlevelof theindividualwiththeuseofamplification.Uninterrupted useofHAwasdefinedastheuseforlongerthan8h/day.
The second stage of the study, with the realization of HINTand application of SADL questionnaire, lastedfor approximately1h.
SatisfactionwithAmplificationinDailyLife
Scale---SADL
TheSADLquestionnaireisaninstrumentdesignedtoassess users’satisfactionwithHA.Thisquestionnairecontains 15 questionsdivided intofoursubscales: positiveeffects (six itemsassociated withacousticand psychologicalbenefit), servicesandcosts(threeitemsassociatedwithprofessional competence,productpriceandnumberofrepairs),negative factors(threeitemsrelatedtoenvironmentalnoise ampli-fication,presence offeedback andtheuse oftelephone), andself-image(threeitemsrelatedtoestheticfactorsand tothestigmaofusingHA).13
Considering the 15 items of SADL, in 11 the score attributed by the participants coincided with the scoring scale,andintheotherfouritems(questions2,4,7,and13) therewasaninverserelationshipbetweenthescoreandthe scale(i.e.,inthesequestionsthescore1receives7points, expressinggreater satisfaction).The higherthe numerical results obtained by averaging the responses of each sub-scale,thegreatertheindividual’ssatisfaction.Questions1, 3,5,6,9,and10arerelatedtopositiveeffectsofthe sub-scale;questions2,7,and11arerelatedtonegativefactors ofthe subscale;questions4,8,and13 arerelatedtothe subscale‘self-image’;andquestions12,14,and15referto thesubscale‘servicesandcosts’.14
Results
The results of the probe microphonemeasurements were defined asexpected (target) responses, and asresponses obtainedofsoundpressurelevelwiththeuseof amplifica-tion(REAR),intheintensityof50,65,and80dBSPL.
Forgroups 1and2,amaximumdifferenceof10dBwas observedbetweentheexpectedresultsandthoseobtained inthewholefrequencyrangeinthethreeinput levels.No discrepanciesbetweentheresultsobtainedatall frequen-ciesforthewholesamplewerenoted,andnoresponsewas obtained exceedingthe expectedanswers,respecting the establishedprescriptionrules.
Regarding theresults of HINT,Figs.1 and2 depict the dataobtainedinpatientswithRITEandRITAfittings, respec-tively.TheresultsfromSADLquestionnairearedescribedin
Fig.3.
ConsideringtheresultsofHINTbetweengroups1and2, analysisofvariance(ANOVA)revealedastatistically signif-icantdifference(p=0.01)betweenthefactor‘withoutHA’
60
50
40
30
Response/dB
20
10
0
–10
Silence F.N. N.R. N.L.
Noise position
RITE pre-RITE post-RITE post-6wk.
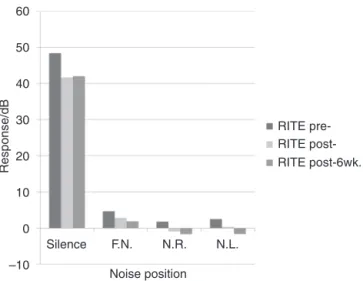
Figure1 Responsesingroup1obtainedwiththeapplication ofthehearinginnoisetest(HINT)atthreetimes:without hear-ingaid(HA),withHA,andsixweeksafterthefitting(n=10).
and‘with HA’ in a silence condition. Evaluating such sig-nificance,theTukeytestrevealednosignificantdifference betweenthegroupsofRITEandRITAHAusers.
As for the results in the presence of noise, there was no significant difference between RITA and RITE users, regardingtothetimeofuseofHAandtonoisepositioning.
Fig.1indicatesthat,inthenoisepositions‘infront’,‘tothe right’,and‘totheleft’,group1patientsshowed improve-ment in speechperception, according tothe time of use ofHA.
InFig.2,thegroupofRITAusersshowedbetterresultsin speechperceptiontestinthepresenceofnoisetotheleft andtotheright,withalongeruseoftheHAtest.
When the degree of satisfaction of participants from both groups wascompared using ANOVA for two criteria, nostatistically significant difference wasobserved in any subscale.
60
50
40
30
Response/dB
20
10
0
–10
Silence F.N. N.R. N.L.
Noise position
RITE pre-RITE post-RITE post-6wk.
8.00
5.90 5.92 5.886.22
7.006.70
5.42 4.80
5.605.88
RITE RITA 7.00
6.00
5.00
Scor
ing
4.00
3.00
2.00
1.00
0.00
Global Positive Effect
Service and cost
Negative factors
Subescalas
Self-image
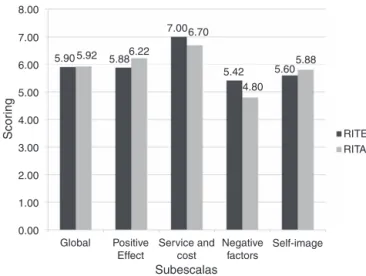
Figure3 Meanscoreofsatisfactionlevelofreceiverinthe ear(RITE)andreceiverintheaid(RITA)hearingaidusersinthe foursubscalesoftheSatisfactionwithAmplificationinDailyLife (SADL)questionnaire(n=20).
Discussion
The probe microphone measures consist of an objective andaccuratetechniquetocheckwhethertheperformance of the HAin the ear of the user is equivalent toa given curve(orasetofcurves)of gainor outputperprescribed frequency. These measures are considered to be a good practiceinthefittingprocedureofthesedevices.4,5,8,19,22,23
In this study, these measurements were performed, sug-gesting that the adequacy of HA settings to the target canprovidebetterspeechrecognitionand,inconsequence, greaterusers’satisfactionwiththedevice.Thegroupshad theirHAadjustedaccordingtoprescriptivemethods,andall participantsreachedthetarget,beingconsidereda differ-enceof10dB.19
Regardingthespeechrecognitiontests,itisknownthat theycanbeusedtopredictthedifficultiesthatpeoplewill haveincertainenvironmentswhenusingHA.Furthermore, thesetestsfacilitatethespeechtherapist’sdecision-making processregarding the need for specific training or use of otherdevices.19
Thespeechtestsinnoiseconditionsweredevelopedinan attempttohampertheidentificationofaspeechsignaland tosimulatereal-lifesituationsexperiencedbypatients.24In
addition,theinformationobtainedfromspeechperception in noise tests can be usedto accomplish the therapeutic planningforagivenpatient.25
Inthisstudy,theresultsofHINTobtainedbyanalysisof variance(Figs.1and2)indicatedastatisticallysignificant difference(p=0.01)betweentheresponseswithand with-outHAinconditionofsilence.TheTukeytest revealedno significantdifferencebetweenthegroupsofRITEandRITA HAusers.ThisresultdemonstratesthatHAprovidesa sig-nificantimprovementinspeechrecognitioninconditionof silenceforbothgroupsofsubjects;however,whenthis vari-ablewascomparedaftersixweeks,therewasnosignificant difference.
Regardingtheresultsinthepresenceofnoise,therewas no significant difference between RITE and RITA users in
relation to the timeof use of HA andthe noise position.
Fig.1 shows thatin front,right, andleft positionsof the noise,subjectsingroup1(RITEusers)showedimprovement in speech perception regarding the timeof HAfitting. In
Fig.2,thegroupofRITAusers,aftersixweeksusingtheHA device,showedimprovementinthespeechperceptiontest withpresenceofnoiseinfrontandrightpositions.
For both groups, when the situation without HA and aftersix weeksof adaptationwascompared,asignificant improvementinspeechperceptioninpresenceofnoisewas observed.Inastudyofopen-fitusers,itwasfoundthatthe effectofacclimatizationthatoccurswithHAusersresults inimprovementinthespeechrecognitionskills,andhence inthecommunicationandusersatisfaction.26
Theuseofsoundamplificationcanimprovethespeech recognitionovertime,afteraperiodofsixto12weeksof amplification.27 Thus, acclimatizationreferstotheperiod
followingtheHAfitting,whenaprogressiveimprovementof listeningskillsandspeechrecognitionoccurs,asaresultof thenewcluesofspeechavailableforamplificationusers.28
ConsideringthatasuccessfulHAfittinginvolvesmultiple aspects,thebenefits ofacclimatizationcannot belimited onlytotheimprovementinspeechrecognition,butalsoto matters involving allaspects ofthe user’ communication, andthatprovidesalevelofsatisfaction,thankstohis/her newconditionoflistener.29
Regardingthe satisfactionwith theuse of HA (Fig.3), the results of the SADL questionnaire subscales (positive effect,serviceandcost,negativefactors,andself-image) werehigherthantheresultsinthenormalization,withlower values13forbothgroups.Onlythesubscale‘self-image’for
RITE amplificationusers confirmed the normative data. A high level of satisfaction in the subscale‘positive effect’ wasnotedfor thegroups ---aresultsimilartodatafroma nationalsurvey.30
Ingeneral,theparticipantsweresatisfiedinallsubscales withtheuseofHA,regardlessofthelocationofthereceiver. Nosignificantrelationshipbetweenthedegreeof satisfac-tionofthe participantswasfound, whentheresponses of thegroupsinthequestionnaireasawholewerecompared. The data obtained are consistent with a study emphasizingthattheexperiencewiththeaudiological ser-vice/support influences on the satisfaction with HA use; subjects whoreported their satisfactionwiththe support receivedalsotendedtoreportgreatersatisfactionwiththe device.31
In a study of 25 adult open-fit users, the Abbreviate Profile of Hearing Aid Benefit (APHAB) questionnaire was applied to measure the individual benefit with the dif-ferentpositions of the receiver,with nosignificant result betweenRITEandRITA.However,greaterusersatisfaction wasobservedwithRITE,duetotheappearance,comfort, retention,andspeechintelligibility.32Thestudyinquestion
observedsimilardataforbothadaptations(RITEandRITA); however,theresponsesweresignificantlybetter,compared totheabsenceofamplification.
Conclusion
Individualswithslopinghearinglossusinganopen-fitsystem showed improvement in auditory performance, according toobjectiveandsubjectivemeasurements,consideringthe high-levelsatisfactionwiththeuseofamplificationandthe improvementinspeechrecognitionin situationsofsilence andnoise.Therewasnodifferenceinperformancebetween RITEandRITAusers.
Funding
ThisstudywassupportedbyFundac¸ãodeAmparoàPesquisa doEstadodeSãoPaulo(FAPESP).Processn.2011/01454-0.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.KukF,BaekgaardL.HearingaidselectionandBTEs: choosing amongvarious‘open-ear’and‘receiver-in-canal’options.Hear Rev.2008;12:36---42.
2.OttoWC.Evaluationofanopen-canalhearingaid by experi-encedusers.HearJ.2005;58:26---32.
3.MacKenzie DJ. Open-canal fittings: a special issue. Hear J. 2006;59:50---6.
4.ValenteM,AbramsH,BensonD,ChisolmT,CitronD,Hampton D,etal.Guidelinesfortheaudiologicalmanagementofadult hearingimpairment.AudiolToday.2006;18:1---44.
5.American Academy of Audiology. Guidelines for the audio-logic management of adult hearing impairment. AAA; 2008. p. 44. Available at: http://www.audiology.org/resources/ documentlibrary/Documents/haguidelines
6.KrishnamurtiS,AndersonL.Digitalnoisereductionprocessingin hearingaids:howmuchandwhere?HearRev.2008.Availableat: http://www.hearingreview.com/issues/articles/2008-0304. asp
7.HallenbeckSA.Considerationsinperformingrealearmeasures withopenfithearinginstruments.AudiolOnline.2008. Avail-able at: http://www.audiologyonline.com/askexpert/display question.asp?questionid=539
8.MuellerHG.Probe-micmeasurements:hearingaidfitting’smost neglectedelement.HearJ.2005;58:21---30.
9.DillonH.Assessingtheoutcomesofhearingrehabilitation.In: Hearingaids.NewYork:Thieme;2001.p.349---69.
10.NilsonM,SoliSD,Sullivan JA.Developmentofthehearingin noisetestforthemeasurementofspeechreceptionthresholds inquietinnoise.JAcoustSocAm.1994;95:1085---99.
11.SandlinRE.Soundfieldassessment: hearingaidsand related issues.In:SandlinRE,editor.Hearingaidamplification: techni-calandclinicalconsiderations.2nded.SanDiego,CA:Singular PublishingGroup;2000.p.343---68.
12.ÁvilaVD.Impactodaprotetizac¸ãoauditivanaqualidadedevida doIdoso.In:Trabalhodeconclusãodecurso(Graduac¸ão)--- Uni-versidadeFederaldeMinasGerais.BeloHorizonte:Faculdade deMedicina,CursodeFonoaudiologia;2008.
13.CoxRM,AlexanderGC.Measuringsatisfactionwith Amplifica-tioninDailyLife:theSADLScale.EarHear.1999;20:306---20.
14.MondelliMFCG, MagalhãesFF,LaurisJRP. Adaptac¸ãocultural doquestionárioSADL(SatisfactionwithAmplificationinDaily Life)deparaoportuguêsbrasileiro.BrazJOtorhinolaryngol. 2011;77:563---72.
15.Hosford-DunnH,HalpernJ.Clinicalapplicationofthe satisfac-tionwithAmplificationinDailyLife scaleinprivatepractice I:statistical,contentandfactorialvalidity.JAmAcadAudiol. 2000;11:523---39.
16.Hosford-DunnH, Halpern J. Clinicalapplication ofthe SADL scaleinprivatepracticeII:predictivevalidityoffitting varia-bles.JAmAcadAudiol.2001;12:15---36.
17.BRASIL. Ministério da Saúde. Política Nacional de Atenc¸ão à Saúde Auditiva, portaria GM/MS n. 2.073 de 28/09/2004. www.saude.gov.br
18.WHO---WorldHealthOrganization.Gradesofhearing impair-ment;2012.Availableat:http://www.who.int/pbd/deafness/ hearingimpairmentgrades/en/index.html[accessed6.2.13;1 screen].
19.Dillon H, Keidser G. Is probe-mic measurement of HA gain-frequencyresponsebestpractice?HearJ.2003;56:28---30. 20.BevilacquaMC,BanharaMR,CostaEA,VignolyAB,Alvarenga
KF.TheBrazilianPortuguesehearinginnoisetest.IntJAudiol. 2008;47:364---5.
21.WeissD,DempseyJJ.Performanceofbilingualspeakersonthe EnglishandSpanishversionsoftheHearinginNoiseTest(HINT). JAmAcadAudiol.2008;19:5---17.
22.YanzJL,PisaJFD,OlsonL.IntegratedREM:real-ear measure-mentfromahearingaid.HearRev.2007.Availableat:http:// www.hearingreview.com/issues/articles/2007-0504.asp[cited 9.12.10].
23.El examen del audıfono digital. Auditio: Rev Electron Audiol. 2002;1:25---9. Available at: http://www.auditio.com/ revista/pdf/vol1/2/010203.pdf[cited9.11.10].
24.KukF.Considerationsinmodernmultichannelnonlinearhearing aids.In:ValenteM,editor.Hearingaids:standards,options,and limitations.2nded.NewYork:Thieme;2002.p.178---213. 25.MatasCG,IórioMCM.Verificac¸ãoevalidac¸ãodo processode
selec¸ão e adaptac¸ão de próteses auditivas. In: Almeida K, IórioMCM,editors.Prótesesauditivas:fundamentosteóricose aplicac¸õesclínicas.2nded.SãoPaulo:Lovise;2003.p.305---23. 26.PicoliniMM,BlascaWQ,CamposK,MondelliMFCG.Adaptac¸ão aberta:avaliac¸ãodasatisfac¸ãodosusuários deum centrode altacomplexidade.RevCEFAC.2011;13:676---84.
27.AlmeidaK.Avaliac¸ãodosresultadosdaintervenc¸ão.In:Almeida K,Iório MCM,editors.Prótesesauditivas: fundamentos teóri-coseaplicac¸õesclínicas.2nd ed.SãoPaulo:Lovise;2003.p. 357---79.
28.Munro KJ, Lutman ME. The effect of speech presentation levelonmeasurementofauditoryacclimatizationtoamplified speech.JAcoustSocAm.2003;114:484---95.
29.HumesLE,WilsonDL,BarlowNH,GarnerC.Changesin hearing-aidbenefitfollowing1or2yearsofhearing-aidsusebyolder adults.JSpeechLangHearRes.2002;45:772---82.
30.Magalhães FF, Mondelli MFCG. Avaliac¸ão da satisfac¸ão dos usuáriosdeaparelhodeamplificac¸ãosonoraindividual---revisão sistemática.RevCEFAC.2011;13:552---8.
31.DillonH,BirtlesG,LovegroveR.Measuringtheoutcomesofa nationalrehabilitationprogram:normativedatafortheclient orientedscaleofimprovement(COSI)andthehearingaiduser’s questionnaire(HAUQ).JAmAcadAudiol.1999;10:67---79. 32.AlworthLN,PlylerPN,ReberMB,JohnstonePM.Theeffects