BrazJOtorhinolaryngol.2016;82(3):281---284
www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Audiologic
evaluations
of
children
with
mucopolysaccharidosis
夽
C
¸a˘
gıl
Gökdo˘
gan
a,∗,
¸enay
S
Altinyay
a,
Ozan
Gökdo˘
gan
b,
Hakan
Tutar
c,
Bülent
Gündüz
a, ˙Ilyas
Okur
d,
Leyla
Tümer
e,
Yusuf
Kemal
Kemalo˘
glu
caDepartmentofAudiology,GaziUniversityHospital,Ankara,Turkey bDepartmentofENT-HNS,MemorialHospital,Ankara,Turkey cDepartmentofENT-HNS,GaziUniversityHospital,Ankara,Turkey
dDepartmentofPediatricNutritionandMetabolism,GaziUniversityHospital,Ankara,Turkey eDepartmentofPediatricEndocrinology,GaziUniversityHospital,Ankara,Turkey
Received16December2014;accepted5May2015 Availableonline25September2015
KEYWORDS
Mucopolysaccharido-sis;
Hearingloss;
Audiologicevaluation
Abstract
Introduction:Mucopolysaccharidosisisahereditarylysosomalstoragedisease,whichdevelops duetoadeficiencyintheenzymesthatplayaroleinthemetabolismofglycosaminoglycans (GAG).Theincidenceofmucopolysaccharidosisis1/25,000,withautosomalrecessive inheri-tance(exceptforMPSII).Mucopolysaccharidosisoccursinsevendifferenttypes,eachwitha differentcongenitaldeficiencyoflysosomalenzymes.Inmucopolysaccharidosispatients,even thoughprogressionofclinicalfindingsisnotprominent,thediseaseadvancesandcausesdeath atearlyages.Facialdysmorphism,growthretardation,mentalretardation,andskeletalorjoint dysplasiaarethemostfrequentlyfoundsymptomsinthesepatients.
Objective: Thepurposeofourstudyistopresentthetypesofhearinglosstypesand tympano-metricfindingsofpatientswithmucopolysaccharidosisreferredtoourclinicwithsuspicionof hearingloss.
Methods:After otorhinolaryngological examination, 9 patients with different types of mucopolysaccharidosis, underwent to immittance and audiometric evaluations, performed accordingtotheirphysicalandmentalabilities,andages,inordertodeterminetheirhearing thresholds.
Results:Theaudiometricfindingsofthe9patientsfollowedwithmucopolysaccharidosiswere reportedseparatelyforeachcase.
夽 Pleasecitethisarticleas:Gökdo˘ganC¸,AltinyayS¸,Gökdo˘ganO,TutarH,GündüzB,Okur ˙I,etal.Audiologicevaluationsofchildrenwith
mucopolysaccharidosis.BrazJOtorhinolaryngol.2016;82:281---4. ∗Correspondingauthor.
E-mail:[email protected](C¸.Gökdo˘gan).
http://dx.doi.org/10.1016/j.bjorl.2015.05.007
1808-8694/©2015Associac¸˜aoBrasileirade OtorrinolaringologiaeCirurgiaC´ervico-Facial.Published byElsevierEditoraLtda.Allrights
282 Gökdo˘ganC¸etal.
Conclusion:Based onthehigh frequencyofhearing lossin mucopolysaccharidosispatients, earlyanddetailed audiologicalevaluationsarehighlydesirable.Therefore,regularand sys-tematicmultidisciplinaryevaluationsareveryimportant.
© 2015Associac¸˜ao Brasileira de Otorrinolaringologiae CirurgiaC´ervico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Mucopolissacaridose; Perdaauditiva; Avaliac¸ãoaudiológica
Avaliac¸ãoaudiológicaemcrianc¸ascommucopolissacaridose
Resumo
Introduc¸ão:Mucopolissacaridose (MPS) é uma doenc¸a hereditária de depósito lisossômico, decorrentedadeficiênciadasenzimasqueinfluenciamometabolismodosglicosaminoglicanos (GAGs).A incidênciade MPS é de1/25.000 habitantes, resultante deheranc¸a autossômica recessiva(excetonocasodeMPSII).MPS seapresentanaformadesetetiposdiferentese, emcadatipo,ocorreumadeficiênciacongênitadistintadeenzimaslisossômicas.Emboraem pacientescomMPSosachadosclínicosnãosejamgeralmenteobservados,adoenc¸aprogrideem seucursonaturalecostumalevaraóbitopacientesmuitojovens.Dismorfismofacial,retardo decrescimento,retardo mentaledisplasiaesquelética ouarticularsãoossinaisesintomas maisfrequentementeobservadosnessespacientes.
Objetivo:Afinalidadedopresenteestudofoiapresentarostiposdeperdaauditivaeosachados timpanométricosdepacientescomMPSencaminhadosparanossaclínicacomsuspeitadeperda auditiva.
Método: Emseguidaaoexameotorrinolaringológico,novepacientescomdiferentestiposde MPS,foramsubmetidosaavaliac¸õesimitanciométricasetestesaudiométricosdeacordocom suafaixaetáriaeficiênciafísicaemental,nointuitodeidentificarseuslimiaresauditivos.
Resultados: Os achados audiométricos dos nove pacientes acompanhados por MPS foram descritosseparadamenteparacadacaso.
Conclusão:Baseado naaltafrequência deperdaauditivaem pacientescomMPS, avaliac¸ão audiológicaprecoceedetalhadaéaltamentedesejável.Paratanto,éimportantequesejam realizadosavaliac¸õesmultidisciplinaresperiódicasesistemáticas.
©2015Associac¸˜aoBrasileira deOtorrinolaringologiaeCirurgiaC´ervico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Mucopolysaccharidosis(MPS)isahereditarylysosomal stor-age disease, which develops due to the deficiency in the enzymes that play a role in the metabolism of glycosaminoglycans (GAG). Progressive GAG accumulation causesadvancedgrowthretardation, skeletaldeformities, hearingloss,weakjointmovement,andfacialdysmorphism. Inaccordancewiththedeficiencyoftheknown11enzymes, MPS has seven sub-types (MPS I, MPS II, MPS III, MPS IV, MPSVI,MPSVII,MPSIX).AlthoughtheincidenceofMPSin accordancewithitssub-typesvaries,ageneralincidenceof 1/25,000hasbeenreported.1---3
InpatientswithMPS,hearinglossisobserveddueto var-ious reasons. Conductive hearing loss (CHL) may develop due to recurrent upper respiratory tract infections and serousotitismediaorbonechaindeformities.Sensorineural hearingloss(SHL)isthoughttobecausedduetothe accu-mulationofGAGinthecochlea,auditorynerve,andbrain stem.Inmanypatients,mixed-typehearingloss,alongwith thesymptomsofconductiveandsensorineuralhearingloss, canalsobeseen.InCHLrelatedtomiddleeareffusion,while theventilation tubeimplementation isfrequently usedas
treatment, hearing aidsareadvised in SHL.4---7 Early diag-nosisofhearinglossescarriesgreatimportanceintermsof early intervention in MPSpatients, aswell asin allother patients.8,9
The purpose of the present study was to present the hearing loss type, degree, and tympanometric findings of patientswithMPS,whoaredirectedtothisclinicwiththe suspicionofhearingloss.
Methods
Audiologicevaluationsofchildrenwithmucopolysaccharidosis 283
Table1 Degreeofhearingloss(dBHL).
Degreeofhearingloss Hearinglossrange(dBHL) Normal −10to15
Slight 16---25 Mild 26---40 Moderate 41---55 Moderatelysevere 56---70 Severe 71---90 Profound 90+
Table2 Tympanogramtypes(daPa).
Tympanogramtype Pressureintervals(daPa) TypeA +50to(−150)
TypeB −400
TypeC −150to(−399)
testswhichareappropriateforthepatients’ages,physical andmentalefficiencies,andboth airandboneconduction thresholdsweredeterminedat250,500,1000,2000,4000, 6000,and8000Hz.
The hearing loss levelswere determinedby taking the averageofpuretoneairconductionthresholds,determined at0.5,1,2,and4kHz,inaccordancewiththeintervalsgiven inTable1.
Hearlosswasclassifiedunderthreegroupsasconductive, mixed,andsensorineural.ForCHL,whilethebonehearing thresholdswerepresentaudiometrically(lessthan20dB),it hasbeenacceptedthat;theaverageair-bonegapin0.5,1, 2kHztobemorethan15dB;inmixedtypehearinglosses, bonehearingthresholdstobe20dBandoveraudiometrically andtheaverageair-bonegaptobemorethan15dBin0.5, 1,2kHz;insensorineuralhearingloss(SHL),thedifference betweentheairandboneconductionthresholdstobeless than15dBinaveragein0.5,1,2kHz.
In the tympanometrical evaluation, 225Hz probe tone signalswereused.Thetympanogramtypeswereevaluated inaccordancewiththevaluesgiveninTable2.
Statisticalanalysis
For the statistical analysis, SPSS version 16.0 (SPSS Inc., Chicago, IL, United States) was used. For the age aver-ageandstandarddeviation(SD),descriptivestatisticswere developed.
Results
TheageaverageofthetotalofninepatientswithMPS,four female (44.44%) and five male (55.55%), was determined as5.66±2.73.TherewerethreecasesofMPSVI(33.33%), threecasesofMPSI(33.33%),onecaseofMPSIII(11.11%), andtwocasesofMPSIV(22.22%)thatwerediagnosed.Cases MÖand EÖ aresiblings; ˙IK and ˙IK 2 are twins.The other fivepatientsarenotrelated.Thedegreeofhearingloss,its type,andtympanometricalfindings areshown in Table3. Thereweresixears withconductive hearingloss(33.33%) (HLoneear:slight;HLoneear:mild;HLtwoears:moderate, andHLtwoears:moderatelysevere); 12ears withmixed hearingloss(66.66%)(HLtwoears:mild;HLfourears: mod-erate,HLfiveears:severe,andHLoneear:profound)were determined.Therewere14earswithTypeBtympanogram (77.77%),threeearswithTypeCtympanogram(16.66%),and oneearwithTypeAtympanogram(5.55%).E.C¸.,B.E.B.,and MSEhadabilateralventilationtube(VT)inserted.Although theotherpatientswereadvised regardingtheVT applica-tionaswell, ithasnotbeen carriedoutupon thewishof theirfamilies.WiththeexceptionofMÖandBEB,although allpatientswereadvisedtousehearingaids,thefamilies didnot adoptthe useof these devicesand didnot come regularlyforfollow-ups.
Discussion
In cases with MPS (Table 4), the initiation of treatment in early stages carries great importance in terms of the prognosisofthedisease.However,duetothelate appear-ance of the symptoms, the definite diagnosis range is 3---4 years of age. In the follow-up of the stages of the treatmentsofpatients withMPS, theotolaryngologistand audiologists have a significant role in multidisciplinary teamwork.Recurrent serous otitismedia and hearingloss
Table3 AudiometricalfindingsofpatientswithMPS.
Patient Agea Diagnosis Tympanometricalfindings Typeofhearingloss Degreeofhearingloss
Right Left Right Left Right Left
MÖ 9 MPSVI TypeC TypeA Conductive Conductive Slight Mild
EÖ 4 MPSVI TypeC TypeC Mixed Mixed Moderate Moderate
˙IK 3 MPSI TypeB TypeB Mixed Mixed Severe Severe
˙IK2 3 MPSI TypeB TypeB Mixed Mixed Severe Severe
EC¸ 9 MPSVI TypeB TypeB Conductive Conductive Moderate Moderatelysevere
SD 8 MPSIV TypeB TypeB Mixed Mixed Moderate Mild
BEB 6 MPSI TypeB TypeB Conductive Conductive Moderate Moderatelysevere
MSE 7 MPSIV TypeB TypeB Mixed Mixed Moderate Moderate
YCE 2 MPSIII TypeB TypeB Mixed Mixed Severe Profound
284 Gökdo˘ganC¸etal.
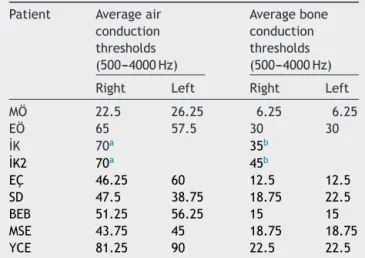
Table4 Air and boneconduction thresholdsof patients withMPS(dBHL).
Patient Averageair conduction thresholds (500---4000Hz)
Averagebone conduction thresholds (500---4000Hz) Right Left Right Left MÖ 22.5 26.25 6.25 6.25 EÖ 65 57.5 30 30 ˙IK 70a 35b
˙IK2 70a 45b
EC¸ 46.25 60 12.5 12.5
SD 47.5 38.75 18.75 22.5
BEB 51.25 56.25 15 15
MSE 43.75 45 18.75 18.75
YCE 81.25 90 22.5 22.5
aTheairconductionthresholdshavebeendeterminedinfree
field.
b The bone conductionthresholds have been determinedin
accordancewiththespeechrecognitionthresholds.
that develops in individuals within this disease group are the reasons why better, long-term follow-ups should be done.Hearinglosscanbeseeninvarioustypesanddegrees in MPS in general.10---13 Overall, conductive hearing losses due to chronic effusion and eustachian tube dysfunction areseenmore inpatients withMPS; the incidenceofSHL hasnotbeendeterminedveryclearly.10
Although conductiveand mixed-type hearing losswere observedinthecasesofthepresentstudy,SHLcompatible withliteraturehasnotbeendetermined.Inthestudies con-ducted,it wasstatedthattheincidenceof mixedhearing lossis more,andthat thisfactis relatedwithage.While conductivehearingloss isdeterminedinearlyagesandin patientswhoarediagnosedearlier,ithasbeenstatedthat mixedhearingloss can be observed,and that thisrate is between33%and71%asageincreases.Inthepresentcases, degreeofhearinglosswasdeterminedfromslighttosevere. This difference is considered to be due to GAG’s exces-sive accumulation in the cochlear ducts, stria vascularis, andcochlearnerve,whichpreventsthemfromfunctioning efficiently.14 Inthepresent cases,theincidenceofTypeB andCtympanogram wasdeterminedtobe high,in accor-dancewiththeliterature.AccordingtoYuLinetal.,while this rateis stated toreach 70%, the incidence of Type B tympanogramwasdeterminedas77.77%andtheincidence ofType C tympanogram wasdeterminedas 16.66%in the presentstudy,similarly. VTapplication isadvised tocases withsimilarclinicalfindingsindifferentclinicsaswell,just asinthe present study.However,a majority of thecases inthisstudy havehindered theirtreatments,duetotheir families’rejectionoftheVTapplication.Incasesforwhich hearingaidsareadvised,whilesocio-economicalinadequacy creates hardships in coming to follow-ups and obtaining theseaids,the factthatmanylivein differentcities pre-ventscontinuityinfollow-ups.
Conclusion
IncaseswithMPS,sincetheincidenceofhearinglossishigh, thehearinglossshouldbedeterminedinearlystages.After the diagnosis, the required treatments should be started promptlyandthusqualityoflifeshouldbeincreased. How-ever,itisconsideredthatthisisonlypossibleasaresultof regularandsystematicfollow-upsandwithmultidisciplinary studies.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.NeufeldEF,MuenzerJ.Themucopolysaccharidoses.In:Scriver CR,BeaudetAL,SlyWS,ValleD,ChildsB,KinzlerKW,etal., editors.The metabolicand molecularbasesofinherited dis-ease.8thed.NewYork:McGraw-Hill;2001.p.3421---52.
2.ChuangCK,LinSP. Neurochemicalchangesand therapeutical approachesinmucopolysaccharidoses.In:SurendranS,Aschner M,BhatnagarM,editors.Neurochemistryofmetabolicdiseases ---lysosomalstoragediseases,phenylketonuriaandCanavan dis-ease.Trivandrum,India:TransworldResearchNetwork;2007.p. 1---20.
3.TomatsuS,FujiiT,FukushiM,OgumaT,ShimadaT,MaedaM, etal.Newborn screeninganddiagnosisof mucopolysacchari-doses.MolGenetMetab.2013;110:42---53.
4.SchleierE, Streubel HG. Phoniatricaspects of childrenwith mucopolysaccharidosis.FoliaPhoniatr.1976;28:65---72.
5.Peck JE. Hearing loss in Hunter’s syndrome----mucopolysac-charidosisII.EarHear.1984;5:243---6.
6.Wold SM,DerkayCS, Darrow DH,Proud V.Roleof the pedi-atricotolaryngologistindiagnosisandmanagementofchildren with mucopolysaccharidoses. Int J Pediatr Otorhinolaryngol. 2010;74:27---31.
7.HendrikszCJ,Al-JawadM,BergerKI,HawleySM,LawrenceR, McArdleC,etal.Clinicaloverviewandtreatmentoptionsfor non-skeletalmanifestationsofmucopolysaccharidosistypeIVA. JInheritMetabDis.2013;36:309---22.
8.NapiontekU,KeilmannA.Hearingimpairmentinpatientswith mucopolysaccharidoses.ActaPaediatrSuppl.2006;451:114.
9.KeilmannA,NakaratT,BruceIA,MolterD,MalmG, Investiga-torsHOS.Hearinglossinpatientswithmucopolysaccharidosis II:datafromHOS----theHunterOutcomeSurvey.JInheritMetab Dis.2012;35:343---53.
10.SimmonsMA,BruceIA,PenneyS,WraithE,RotheraMP. Otorhi-nolaryngologicalmanifestationsofthemucopolysaccharidoses. IntJPediatrOtorhinolaryngol.2005;69:589---95.
11.Shinhar SY, Zablocki H, Madgy DN. Airway management in mucopolysaccharidestoragedisorders.ArchOtolaryngolHead NeckSurg.2004;130:233---7.
12.Bredenkamp JK, Smith ME, Dudley JP, Williams JC, Crum-ley RL, Crockett DM. Otolaryngologic manifestations of the mucopolysaccharidoses. Ann Otol Rhinol Laryngol. 1992;101:472---8.
13.Peck JE. Hearing loss in Hunter’s syndrome----mucopolysac-charidosisII.EarHear.1984;5:243---6.