REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
MISCELLANEOUS
Good
clinical
practice
guide
for
opioids
in
pain
management:
the
three
Ts
---
titration
(trial),
tweaking
(tailoring),
transition
(tapering)
Flaminia
Coluzzi
a,
Robert
Taylor
Jr.
b,
Joseph
V.
Pergolizzi
Jr.
c,d,e,
Consalvo
Mattia
a,
Robert
B.
Raffa
f,∗aDepartmentofMedical,SurgicalSciencesandBiotechnologies,SAPIENZAUniversityofRome,Rome,Italy bNEMAResearchInc.,Naples,USA
cJohnsHopkinsUniversity,Baltimore,USA
dDepartmentofPharmacology,TempleUniversitySchoolofMedicine,Philadelphia,USA eGeorgetownUniversitySchoolofMedicine,Washington,USA
fDepartmentofPharmaceuticalSciences,TempleUniversitySchoolofPharmacy,Philadelphia,USA
Received28June2014;accepted3September2014 Availableonline28November2014
KEYWORDS
Painmanagement; Opioid;
Titration; Tailoring; Tapering
Abstract
Backgroundandobjectives: Achievinggoodclinicalpracticeintheuseofopioidsaspartofa comprehensivepainmanagementregimencanfacesignificantchallenges.Despiteguidelines fromgovernmentalandpain society/organizationsources,therearestillsignificanthurdles. Areviewofsomebasictenetsofopioidanalgesiabasedoncurrentpublishedknowledgeand experiencesaboutthisimportanthealthcareimperativeiswarranted.
Content: Consistentwithguidelines,theliteraturesupportsusingthelowesttotalopioiddose thatprovidesadequatepaincontrolwiththefewestadverseeffects.Titration(ortrial)during opioidinitiationisawayofstartinglowandgoingslow(andassessingtheappropriatenessofa specificopioidandformulation).Recognizingthatmultiplefactorscontributetoanindividual’s personalexperienceofpain,thephysical,psychological,social,cultural,spiritual, pharmacoge-nomic,andbehavioralfactorsoftheindividualpatientshouldbetakenintoaccount(tweaking, ortailoring).Finally,forthosepatientsforwhomtransition(tapering)fromopioidisdesired, doingsotoorapidlycanhavenegativeconsequencesandminimizationofproblemsduringthis stepcanbeachievedbypropertapering.
Conclusion:Weconcludethatasimultaneouslyaggressive,yetconservative,approachis advo-cated intheliterature inwhich opioid therapyis dividedinto three keysteps (the3T’s): titration(or trial),tweaking(ortailoring),andtransition(ortapering).Establishmentofthe 3 T’s along with the application of other appropriate good medical practice and clinical
∗Correspondingauthor.
E-mail:[email protected](R.B.Raffa). http://dx.doi.org/10.1016/j.bjane.2014.09.005
experience/judgment, including non-pharmacologic approaches, can assist healthcare providersintheefforttoachieveoptimalmanagementofpain.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
PALAVRAS-CHAVE
Tratamentodador; Opioide;
Titulac¸ão; Ajuste;
Reduc¸ãogradual
Orientac¸ãoparaboapráticaclínicaparaopioidesnotratamentodador:ostrês ‘‘Ts’’---titulac¸ão(teste),ajustes(individualizac¸ão),transic¸ão(reduc¸ãogradual)
Resumo
Justificativaeobjetivos: Arealizac¸ãodeumaboapráticaclínicacomousodeopioidescomo partedeum regimeabrangentedetratamentodadorpodeenfrentardesafiossignificativos. Apesar das diretrizes provenientes de sociedades/organizac¸ões não governamentais para o manejo dador,ainda existemobstáculossignificativos.A revisão de algunsprincípios bási-cosdaanalgesiacomopioidecombasenaexperiênciaeconhecimentodaspublicac¸õesatuais sobreessecuidadoimportantedasaúdeéjustificável.
Conteúdo: Deacordocomasdiretrizes,aliteraturaapoiaousodadosetotalmaisbaixade opi-oidesquefornec¸aocontroleadequadodadorcommenosefeitosadversos.Atitulac¸ão(teste) aoiniciaraadministrac¸ãodeumopioideéumamaneiradecomec¸arcomumaconcentrac¸ão baixa e irdevagar (avaliando aadequac¸ão dafórmula específica de um opioide). Oajuste (individualizac¸ão)éreconhecerquevários fatorescontribuemparaaexperiênciapessoalda dordeumindivíduo,taiscomofatoresfísicos,psicológicos,sociais,culturais,espirituais, far-macogenômicosecomportamentais.Finalmente,paraaquelespacientesnosquaisatransic¸ão (reduc¸ãogradual)doopioideédesejada,fazeressatransic¸ãomuitorapidamentepodemter consequênciasnegativas,eépossívelminimizarosproblemasduranteessaetapaatravésde umareduc¸ãogradual.
Conclusão:Concluímos que uma abordagem simultânea, agressiva, porém conservadora é defendidanaliteraturaemqueaterapiacomopioidesédivididaemtrêsetapasprincipais(os 3‘‘Ts’’---eminglês:titration,tailoring,tapering):titulac¸ão(teste),ajuste(individualizac¸ão) etransic¸ão(reduc¸ãogradual).EstabelecerostrêsTs,juntamentecomaaplicac¸ãodeoutraboa prática médica eexperiência/julgamentoclínico,incluindo abordagensnãofarmacológicas, podemajudarosprofissionaisdesaúdenoesforc¸oparaalcanc¸arotratamentoidealdador. ©2014SociedadeBrasileira deAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Currentestimatesindicatethatasmanyas100million Amer-icans are suffering from a chronic pain condition1 and a
prevalence of 10---50% throughout European countries.2---4
Inadequatepaintreatmentcanhavesevereconsequencesat boththeindividualandsocietallevels.Forindividuals, sim-pledailyactivitiescanbedifficultanddisruptionsinone’s routinecanfurtherleadtomooddisorderssuchas depres-sion,anxiety,and stress.5 Takentogether,theseproblems
can decrease a patient’s quality of life. Forsociety, pain patientsplaceaburdenoneconomic productivityandthe healthcaresystem.6
Inadditiontonon-pharmacologicoptions,thereare sev-eral pharmacologic options for the treatment of pain, as promulgatedbytheWHO(WorldHealthOrganization)pain ‘ladder’ and modifications.7 They include NSAIDs
(nons-teroidal anti-inflammatory drugs), acetaminophen, weak andstrongopioids,musclerelaxants, anticonvulsants,and antidepressants.Mostoftheseareadequatetotreatmildto
moderatepainintheshortterm.Formoderate-to-moderate severepain,strongopioidsaregenerallyconsideredthefirst choice.Opioidshavebecomeincreasinglypopularin treat-ing moderate to moderately severe; ‘‘around the clock’’ pain conditions. Their efficacy for short-term pain relief hasbeen documentedin many randomizedclinical trials; theirlong-termbenefit/riskratiofornon-cancerpainisstill underdebate.8---11 The United States FDA promotes a Risk
EvaluationandMitigationStrategy(REMS).
of pain and use of analgesics, especially combinations of analgesics,totreatvarioustypesofpain.
Inadequateopioidtherapycangenerallybetracedback to errors during a few key stages of opioid treatment (titration/trial/initiation, tailoring/maintenance, taper-ing/rotation). Specific step-by-step protocols for each of thesestages require experienceand educationsince pain treatmentishighlyindividualizedanddynamic.Guidelines fromvariousgovernmentalandpainsocieties/organizations are available to follow, but currently there is no univer-sal opioid guideline.10---18 In order to facilitate the design
andimplementationofrationalandappropriateopioid reg-imens,itishelpfultodifferentiatethebasicstepsofopioid therapy.Inthisreviewweseektopresentcurrentpublished knowledgeandexperiencesregardingthreeimportantsteps ofopioidtreatment:titration(ortrial),tailoring,and taper-ing(The3T’s).
Titration
(trial/initiation)
The initiation phase of opioid therapy is a critical step towardachieving thegreatestbenefit while obtainingthe support,trust,andcomplianceofthepatient.Theultimate goalis to beable toprovide thefastest painrelief with-outcausinganemergenceofadverseeffects.However,the initiationofopioidsis notthesamefor everypatientand differentregimens may need to beimplemented (trial of firstopioid selectionfollowed,ifnecessary,byalternative selection),basedonthetypeofpainandpatient.19
Typeofpain
Itisbestifthehealthcareprovidercandeterminethetype of pain the patient is experiencing (e.g., low-back pain, osteoarthritis,fibromylagia)anddeterminewhetheropioid therapyisappropriate.Forexample,certainpainconditions suchasfibromyalgiadonot alwaysadequately respondto opioids20andthusmightcurrentlynotbethefirstchoicefor
thispaincondition.Long-termuseofopioidsforcertainpain conditions,e.g.,low-backpainandOA(osteoarthritis)are stillunderdebate.Theeffectivenessofopioidsinthese non-cancerconditions,aswellasthepotentialformisuse,abuse, andsideeffectsremainmajorissues.21However,short-term
reliefhasbeen documentedfor manypaintypes including diabetic neuropathy, peripheral neuropathy, postherpetic neuralgia,phantomlimbpain,spinalcordinjurywithpain belowthelevelofinjury,lumbarradiculopathy,OA, rheuma-toidarthritis,low-backpain,andneckpain.14Inthecourse
ofcancer,paincanstartoutasmostlynociceptive,but tran-sition(duetoperipheralandcentralsensitization)occursto include hyperalgesia and a neuropathic component (e.g., allodynia).
Typeofpatientandopioidchoice
Thechoiceofanopioidshouldbecarefullyconsidered.For example, opioid-naïve patients runa higher risk of expe-riencingadverse effects andoverdose.Elderlypatients or patientswithanumberofco-morbiditiesmaybenefitfrom theshorthalflifeofimmediatereleaseopioidsbecauseof the reduced probability of overdose.22 Guidelines by the
Canadiangovernmenthavedescribedtheuseofcodeineor tramadolasfirst-lineopioidsfor mildtomoderate chronic pain due to their reduced potential for misuse, overdose and addiction.14 Ifpain is not effectively controlled with
theseopioids,orifadverseeffectsareexperienced,theuse ofopioidssuchasmorphine,oxycodone,orhydromorphone aredescribed.Other‘atypical’opioids,suchastapentadol or buprenorphine,could be considered.23,24 Guidelines by
theDepartmentofVeteranAffairsandtheBritishPain Soci-ety suggest that nosingle opioid is superior over others, thechoiceshouldbemade basedonlocalexperienceand expertiseandthatselectingthecorrectopioidonthefirst attemptisdifficult,sothatseveralroundsofrotationmay benecessary.12,15
Opioidformulation
Itis criticalthat thetemporalsettingof painbematched withtheappropriaterelease-timingoftheopioid: immedi-ate release for initial titration; rapid onsetbreakthrough pain; and extended-release or transdermal patches for around-the-clockanalgesia.14Ingeneral,patientsshouldbe
placedonsustained/extendedreleaseformulationsifthey benefitfromaconsistentpharmacokineticprofile.However, patientswillresponddifferentlytothetypeandformulation ofanopioidandthusitisuptothehealthcareproviderand patienttounderstandthatseveralroundsofopioidrotation might beneededinordertofindthemostefficacious and safeoption.25
Starting-dose
There is no universal agreement on the starting-doses of individual opioids. The various initiation doses recom-mendedinseveralguidelinesarepresentedinTable1.14,15
Titrationprocedure---generalrulesandguidelines
With any type of opioid therapy, the end goal is to use the lowest opioid dose that provides an adequate level of pain control and a tolerable side effect profile. Some providerstaketheapproach‘startlowandstartslow’and thisapproachseemsreasonable.Oneofthemajorreasons forslowlyandincrementallyincreasinganopioiddoseisto minimizeadverseeffects.Patients,especiallythosewhoare opioid-naive,requiretimetoadjusttotheopioideffects.In addition,itwillbeeasierfor providerstofindtheoptimal dosethatprovidestheright balancebetweenbenefitsand risk.Other reasonsfor slowtitrationinclude:patientmay experiencechangesthatalterpainperceptionafteropioid initiation; and the underlying pain condition may worsen (e.g.,cancerprogression).
Titration:howmuchandwhentoincrease
Table1 Initialstartingdoseforvariousopioids.
Canadian guidelinesa
Departmentof veteranaffairsa
Agencymedical directorsgroup (opioidnaïve)
Americansociety ofinterventional painphysicians (opioidnaïve)
Americansociety ofinterventional painphysicians (opioid experienced)
Codeine 15---30mgevery6h 30mgq4---6h 15mgbidortid CRcodeine 50mgevery12h
CRtramadol 100---150mgevery 24h
Notrecommended
IRmorphine 5---10mg4---6h (max40)
10---30mgq4---6h 10mgq4h Notrecommended 10mg,2---3×
CRmorphine 10---20mg(max40) 15mgq8---12or 30mgq24h
15mgq12h Notrecommended 15---30mg,2×
daily IRoxycodone 5mg4---6h(max
30)
5mgq6h 5mgq4---6h 5---10mg,2---3×
daily
5---10mg,3---4×
daily CRoxycodone 10mg(max
30mg/d)
10mgq12h 10mgq12h Notrecommended 10mgfor12h
IRhydromorphone 1---2mg4---6h(max 8mg/d)
2mgq4---6h 2mgq4---6h 2mgbidortid 2---4mg,2---3×
daily
CRhydromorphone 3mg(max9mg/d) Notrecommended 5---10mg,2×daily
Hydrocodone 5---10mgq4---6h 5---10mgq4---6h 5---10mg,2---3×
daily
5---10mg, 3---4×daily
IRoxymorphone 10---20mgq4---6h 5---10mgq4---6h 5mgbidortid 5---10mg,2---3×
daily IRtapentadol 50mgq4---6h
Tramadol 25mgdaily 50mgbidortid 50mg,3---4×daily
CRoxymorphone 5mgq12h 10mgq12h Notrecommended 10mgq12h Transdermalfentanyl 25mcg/hq72h Notrecommended 12.5---25mcgq72h
Newopioidformulations,recentlyintroducedontheUSand/orEUmarket,arenotyetincludedincurrentguidelines.However,according topublishedRCTs,therecommendedstartingdosesare10/5mgBID(q12h)forER(extended-release)oxycodone/naloxoneand50mg BID(q12h)forERtapentadol.CR,controlledrelease;IR,immediaterelease.
a Nodistinctionbetweenopioidnaïvevs.opioidexperienced.
Particularcareindosingmustbegivenintheelderly, espe-ciallyfrailelderly, lowtolerantopioidpatients,andthose experiencingsideeffects.Carefulmonitoringshouldalways accompany every titrateddose. Providers shouldalsopay particularattentiontothedevelopmentofadverseeffects.
Titration:whentostop
Optimal dose is generally considered achieved when a patient has experienced a ≥30% reduction in pain relief (e.g.,2 pointsonan 11-pointnumerical ratingscale) and no serious,or tolerable, side effects or complications on the dose.16,26,27 However, all of these are meant to
pro-videgeneral guidanceonlyand theactual regimenshould becustomizedtoeachpatient.
Key points to consider when determining if titration needstocontinue:
• Lackofefficacy.
• Sideeffectshavebecomeintolerable.
If efficacy is not achieved, the patient should be re-evaluatedoropioid rotationor formulationchange should beconsidered.
Tweaking
(tailoring/maintenance)
Painassessment
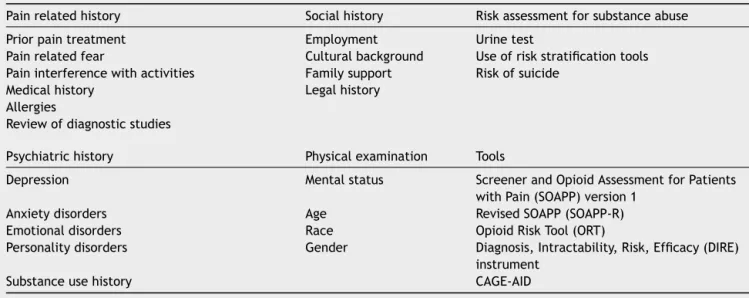
Pain assessment is not only determining a patient’s pain intensityscore.Therearemanyfactorsthatcancontribute toan individual’schronicpainexperience,including phys-ical,psychological,social,cultural,spiritual, genetic,and behavioralfactors.Allofthesefactorsshouldbeassessed inorderfor optimalmanagementtooccur. Manytools are availabletoassessthesefactorsanditisuptothe health-care providers and the patient to determine which ones theyprefertouseat initiationandthroughout treatment. Inaddition,itisimportant fortheprovider tounderstand theassessmenttoolinorderforthephysiciantoaccurately gaugetheimpactofeachindividualfactor.Alistofcommon assessmentsandtoolsthatshouldbeconsideredisincluded inTable2.
Typeofpatient
Table2 Typesofassessmentandtoolsfordeterminingappropriatenessofopioidtherapy.13---15,22,48---54
Painrelatedhistory Socialhistory Riskassessmentforsubstanceabuse
Priorpaintreatment Employment Urinetest
Painrelatedfear Culturalbackground Useofriskstratificationtools Paininterferencewithactivities Familysupport Riskofsuicide
Medicalhistory Legalhistory Allergies
Reviewofdiagnosticstudies
Psychiatrichistory Physicalexamination Tools
Depression Mentalstatus ScreenerandOpioidAssessmentforPatients withPain(SOAPP)version1
Anxietydisorders Age RevisedSOAPP(SOAPP-R) Emotionaldisorders Race OpioidRiskTool(ORT)
Personalitydisorders Gender Diagnosis,Intractability,Risk,Efficacy(DIRE) instrument
Substanceusehistory CAGE-AID
of drugs. The general approach includes: the use of the least-invasiverouteofmedication,thechoiceof sustained-release formulations, the introduction of one agent at a time, at the lowest effective dose, according to the rule ‘start low, go slow’,and a strict monitoring of effi-cacyandsafety.Accordingtothe2009AmericanGeriatrics Society (AGS) guidelineson pharmacologicaltreatment of persistentpaininolderadults,acetaminophenremainsthe first-line recommendation among the non-opioid class.28
NSAIDs pose a risk for causing adverse events within older adult populations. Their use should be limited, particularly in patients with reduced creatinine clear-ance, gastropathy, cardiovascular disease, or congestive heart failure. If needed, a topical formulation should be preferred.AmongoralNSAIDs,naproxenmayhavea compar-ativelylowerriskofcardiovascularevents.29 Intheelderly,
NSAIDs and cyclooxygenase-2 (COX-2)-selective inhibitors should only be used in rare instances.30 Both require
co-administration of an agent for gastrointestinal protec-tion, such as a proton pump inhibitor, if the therapy is extended.
Opioidsarenotexcludedfromuseforolderadults. Opi-oiduseinpatients>65yearshasbeenshowntohavesimilar efficacytothatinyoungeradults.Infact,thereisacurrent trendof under-utilization of opioidsin this patient popu-lationdue tothe high incidence of injuries (falls and hip fractures),particularlywithcodeinecombinations31plusan
increasedriskofcognitiveimpairment.32Opioidshavebeen
recentlyrecognizedasariskfactorforthedevelopmentof osteoporosis,thereforeitisreasonabletosuspectthatthe increasedincidence of fractures observed in opioid users couldberelatedtoreduced bonemass density secondary totheeffectsofopioidsontheendocrinologicalsystem.33
Physiological changes suchas lower serum-binding, lower strokevolume,anddecreased renalfunctionmight playa roleinthealteredpharmacokineticsandpharmacodynamic effectsof opioidsin this patientpopulation. The adverse eventprofilevariesgreatlybetweenopioids.Formost opi-oidsexceptbuprenorphine,thehalf-livesofactivedrugand metabolitesareincreasedintheelderly.Special considera-tionmightbegivenregardingeffectsonrespiration.Inthis
regard,buprenorphinemightbeatop-linechoiceforopioid treatmentintheelderly.34
Co-morbidities
Patients withimpaired liver and/or renal function areat increasedrisk of accumulation ofparent drugor metabo-lites, which canlead totoxicity. However,not allopioids behave the same in renallyimpaired individuals andthus it is up to the prescriber to have adequate knowledge on what opioid and what dose to use in the varying levels of renal impairment. Guidelines developed by the European Palliative ResearchCollaborative stratisfied opi-oids,basedoncurrentliterature,intogroups oftoxicity.35
prescribedatlowerdosesinpatientswithsevereliver dis-ease, with extended dosing intervals when multiple daily dosesareneeded.36
Dysphagia (difficulty swallowing) is common among elderlypeopleandamongcancerpatients.Swallowing prob-lems can cause several clinical problems that complicate administration of oral solid medications. Moreover, some drugs, includingopioids, canworsen swallowingproblems byinducingxerostomia(drymouth)andbydecreasinglower esophagealsphincter(LES)pressure.Forpatientswhohave difficulty swallowingand require opioid analgesics, trans-dermalformulationsmightbeconsidered.37
Genetics
An increasing literature demonstrates that individual vul-nerabilities to specific pain types and mechanisms --- and variationinresponsetopainmedication---mightbepartially explained or predicted by the patient’s genetics.38 There
aremany pharmacogeneticfactors that cancontribute to the efficacy and adverse effects of analgesics, especially theopioids: polymorphismsin genesencodingforproteins controllingtheenzymaticmetabolismofdrugs(e.g.,CYP2D6 andcodeine),thetransportofdrugsoutoftheirtargetorgan (e.g.,P-glycoproteinandfentanyl)andthetargetreceptor (e.g.,mu-opioidreceptorandmorphine).39
More than half of all current prescription drugs are metabolized by the cytochrome P450 (CYP) enzymes (specificallyCYP2D6andCYP3A4).Therefore,drugs metab-olized by this pathway (phase I metabolism), which includes many opioids, suchasoxycodone, codeine, dihy-drocodeine, hydrocodone, and tramadol, are associated with an increased possibility for drug---drug interactions. CYP450inhibitorscanleadtoexcessivelyhighserum concen-trationsoftheparentdrug.Thismayincreasetheincidence of side effects if the parent drug is active (e.g., oxy-codone),oritmaydecreaseefficacyifitisaprodrug(e.g., codeine). Conversely, CYP450 inducers can lead to lower thanexpectedserumconcentrationsoftheparentdrug.This canleadtoareducedeffectiftheparentdrugisactiveor anenhancedeffectifitisaprodrug.Moreover,mutationsin theCYP2D6gene,whichoccurinapproximately1%to7%of theCaucasianpopulation,caneither decreaseorincrease enzymeactivity,leadingtoalterationsinopioidanalgesia.40
Thefuturepromiseofpharmacogeneticsisanindividually tailored,rationaldrugregimenthatmaximizesefficacyand minimizes adverse events. Pharmacogenetic testing could be the alternative to one-size-fits-all prescribing of pain medication.However,pharmacogenetictestingisnotwidely appliedincurrentclinicalpracticeanddrugswhichdonot undergo significant metabolism by CYP enzymes, such as tapentadol,morphine,andoxymorphone,hydromorphone, canbeanalternative.41
Gender
Overthepast20years,anincreasingnumberofstudieshave suggestedsexdifferencesinresponsetopainandanalgesics. In general, it has been suggested that the prevalence of most commonforms ofpain ishigher amongwomen than men, and that women report greater pain after invasive
proceduresthandomen.Comparedwithmen,ithasbeen suggestedthatwomendisplayenhancedsensitivitytomost formofexperimentallyinducedpain.42Ithasbeensuggested
thatwomenhave greater opioidreceptor analgesia. Simi-larly,someevidencesuggeststhatserotonergicagentsmay bemoreefficaciousinalleviatingchronicpaininwomen,43
whichseemsreasonable giventhathormonaland neurobi-ologicalfactorscan directly affect nociceptiveresponses. However,womenhavebeentraditionallyunder-represented inclinicaltrials.Currently,theevidenceonsexdifferences inpainresponseisthoughtnottobestrongenoughtoallow translation of the experimental work to clinical decision-making.44
Transition
(tapering)
Current literature support for, or advice about, how to discontinueanopioidisgenerallylacking.Aswiththe titra-tionstep,performingthissteptoorapidlycanhavesevere consequencessuchasexperiencingopioidwithdrawal symp-toms. These are generally not life threatening and may includeagitation,anxiety,muscleaches,insomnia, sweat-ing,abdominalcramping,diarrhea,nauseaandvomiting.
Individualizedprocess
Theprovidershouldrecognizethevariousreasonsfor discon-tinuingopioidtherapy andthenconstructaplanofaction that is individualized to the patient. As a general guide-line,patientremovaloffanopioidshouldoccurunderthe followingcircumstances:
• Intolerableadverseeffects. • Non-adherencebythepatient.
• Misusebythepatient. • Lackofanalgesiceffect. • Patientrequest.
Tapering:generalguidelinesandgoals
Therearenotmuchdataonthistopicandguidelinesvary substantially.15,16Someexpertsrecommendthatthelongera
patienthasbeenonopioids,theslowerthetapering.Since therange is quite large, physicianexperience,as well as appropriatemonitoring,shouldalwaysbetheguide.
Ithasbeenrecommendedthataspecialistbeinvolvedin thetaperingofcertainpatients,suchas:15
• Those thatareat high risk of aberrantbehaviors(e.g., parasuicidal acts, dealing/selling medications, or those withsevereimpulsecontroldisorders).
• Thosewithcomplicatedwithdrawalsymptoms.
• Thosebeingtapered duetoconcernabout development ofaddiction.
Opioidformulationconsiderations
and diarrhea, musculoskeletal symptoms, insomnia, anxi-ety,andirritability.Occurrenceofsymptomswillbedriven by the specific opioid, the speed of taper and patient co-morbidities.Someopioidsmightbeeasiertotaperthan others.45 Appropriateteststhatcouldbeadministered
dur-ingtheprocesstomonitorthepatientincludetheclinical opiatewithdrawalscale (COWS)andthesubjectiveopiate withdrawalscale.46,47Thesescalescanprovidethephysician
withtheknowledgeofwhethertheplannedtaperingprocess needs adjustment. During the tapering process, adjuvant agentsshouldbeconsideredformanagementofsymptomsof withdrawal.Inaddition,patientsshouldreceive psychoso-cialsupportifneededduringtheprocess.
Conclusion
Pain is a highly individualized process and no one single pharmacologicornon-pharmacologicapproachcompletely removespainin100%ofpatients100%ofthetimewithout anysideeffects.Thisiswhymultipleoptionsareneededand whytheoptionsmustbeoptimizedtotheindividualpatient. Thisisparticularlyimportantwhenconsideringopioid ther-apy,sinceproperopioid,regimen,andpatientselectionare paramount.ThethreeT’softitration(trial),tailoring,and taperingareuseful conceptsandguidesfor rational,safe, and appropriateopioid prescribingwhich should result in improvedoutcomesandopioidoptimization.
Conflicts
of
interest
Dr.PergolizziisaconsultantandspeakerforJanssen Phar-maceuticals, Endo Pharmaceuticals, Purdue Pharma, and InSys.Dr.Raffaisaspeaker,consultant,and/orbasicscience investigatorforseveralpharmaceuticalcompaniesinvolved inanalgesicsresearchbutreceivesnoroyalty(cashor oth-erwise)fromthesaleofanyproduct.
References
1.Institute of medicine (US) committee on advancing pain research C, and education. Relieving pain in America: a blueprint for transforming prevention, care, education and research 2012/05/04 edition. Washington, DC: National AcademiesPress;2011.
2.BreivikH,CollettB,VentafriddaV,etal.Surveyofchronicpain inEurope:prevalence,impactondailylife,andtreatment.Eur JPain.2006;10:287---333.
3.Reid KJ, Harker J, Bala MM, et al. Epidemiology of chronic non-cancer pain in Europe:narrative review of prevalence, pain treatments and pain impact. Curr Med Res Opin. 2011;27:449---62.
4.RustoenT,WahlAK,HanestadBR,etal.Prevalenceand charac-teristicsofchronicpaininthegeneralNorwegianpopulation. EurJPain.2004;8:555---65.
5.David Michaelson and Company. Voices of chronic pain: a nationalstudyconductedforAmericanPainFoundation;2006. 6.StewartWF,RicciJA,CheeE,etal.Lostproductivetimeand costduetocommonpainconditionsintheUSworkforce.JAMA. 2003;290:2443---54.
7.RaffaRB,PergolizziJVJr.Amodernanalgesicspain‘pyramid’. JClinPharmTher.2014;39:4---6.
8.Martell BA, O’Connor PG, Kerns RD, et al. Systematic review: opioidtreatment for chronic backpain: prevalence,
efficacy, and association with addiction. Ann Intern Med. 2007;146:116---27.
9.Deshpande A, Furlan A, Mailis-Gagnon A, et al. Opioids for chronic low-back pain. Cochrane Database Syst Rev. 2007:CD004959.
10.TrescotAM,HelmS,HansenH,etal.Opioidsinthe manage-mentofchronicnon-cancerpain:anupdateofAmericanSociety oftheInterventionalPainPhysicians’(ASIPP)Guidelines.Pain Phys.2008;11:S5---62.
11.Manchikanti L, Abdi S, Atluri S, et al. American society of interventionalpain physicians (ASIPP) guidelines for respon-sibleopioidprescribing inchronic non-cancerpain: Part2 ---Guidance.PainPhys.2012;15:S67S116.
12.TheBritishPainSociety.Opioidsforpersistentpain:good prac-tice.London:TheBritishPainSociety;2010.
13.AmericanPainSociety.Guidelinefortheuseofchronicopioid therapyinchronicnoncancerpain.EvidRev.2009.
14.KahanM,Mailis-GagnonA,WilsonL,etal.Canadianguideline forsafeandeffectiveuseofopioidsforchronicnoncancerpain: clinicalsummaryforfamilyphysicians.Part1:General popula-tion.CanFamPhys.2011;57:1257---66.
15.TheManagement ofOpioidTherapy for ChronicPainWorking Group.In: Affairs, D.O.V., (Ed.),Clinicalpractice guideline: managementofopioidtherapyfor chronicpain, Washington, DC;2010.
16.AgencyMedicalDirectorsGroup.Interagencyguidelineon opi-oiddosingfor chronicnon-cancerpain:aneducationalaidto improvecareandsafetywithopioidtherapy;2010.
17.Ambrosio F, FincoG, Mattia C, et al. SIAARTI recommenda-tionsfor chronic noncancer pain. MinerAnestesiol.2006;72: 859---80.
18.ColuzziF,PappagalloM.Opioidtherapyforchronicnoncancer pain:practiceguidelinesforinitiationandmaintenanceof ther-apy.MinerAnestesiol.2005;71:425---33.
19.MercadanteS.Opioidtitrationincancerpain:acriticalreview. EurJPain.2007;11:823---30.
20.Ngian GS, GuymerEK, Littlejohn GO.The use of opioids in fibromyalgia.IntJRheumDis.2011;14:6---11.
21.Noble M,Treadwell JR, Tregear SJ, et al. Long-term opioid managementfor chronic noncancerpain. CochraneDatabase SystRev.2010:CD006605.
22.ChouR.2009ClinicalGuidelinesfromtheAmericanPain Soci-etyand the AmericanAcademy ofPain Medicine on theuse ofchronicopioidtherapyinchronicnoncancerpain:whatare thekey messages for clinicalpractice? Pol Arch MedWewn. 2009;119:469---77.
23.Riemsma R, Forbes C, Harker J, et al. Systematic review of tapentadol in chronic severe pain. Curr Med Res Opin. 2011;27:1907---30.
24.WolffRF,AuneD,TruyersC,etal.Systematicreviewof effi-cacyandsafetyofbuprenorphineversusfentanylormorphine inpatientswithchronicmoderatetoseverepain.CurrMedRes Opin.2012;28:833---45.
25.Quang-CantagrelND,WallaceMS,MagnusonSK.Opioid substi-tutiontoimprovetheeffectivenessofchronicnoncancerpain control:achartreview.AnesthAnalg.2000;90:933---7. 26.FarrarJT,YoungJPJr,LaMoreauxL,etal.Clinicalimportance
ofchangesinchronicpainintensitymeasuredonan11-point numericalpainratingscale.Pain.2001;94:149---58.
27.DunnKM,SaundersKW,RutterCM,etal.Opioidprescriptions forchronicpainandoverdose:acohortstudy.AnnInternMed. 2010;152:85---92.
28.Pharmacologicalmanagementofpersistent paininolder per-sons.JAmGeriatrSoc.2009;57:1331---46.
30.Gloth FM. Pharmacological management of persistent pain in older persons: focus on opioids and nonopioids. J Pain. 2011;12:S14---20.
31.BuckeridgeD,Huang A,HanleyJ, et al.Risk ofinjury asso-ciated with opioid use in older adults. J Am Geriatr Soc. 2010;58:1664---70.
32.SaundersKW,DunnKM,MerrillJO,etal.Relationshipofopioid useanddosagelevelstofracturesinolderchronicpainpatients. JGenInternMed.2010;25:310---5.
33.MattiaC,DiBussoloE,ColuzziF.Non-analgesiceffectsof opi-oids:theinteractionofopioidswithboneandjoints.CurrPharm Des.2012;18:6005---9.
34.PergolizziJ,BogerRH,BuddK,etal.Opioidsandthe manage-mentofchronicseverepainintheelderly:consensusstatement ofanInternational Expert Panel withfocus onthe six clini-callymostoftenusedWorldHealthOrganizationStepIIIopioids (buprenorphine,fentanyl, hydromorphone, methadone, mor-phine,oxycodone).PainPract.2008;8:287---313.
35.KingS,ForbesK,HanksGW,etal.Asystematicreviewofthe useofopioid medicationfor those withmoderateto severe cancerpainandrenalimpairment:aEuropeanPalliativeCare ResearchCollaborativeopioidguidelinesproject.PalliatMed. 2011;25:525---52.
36.HannaM.Theeffectsofliverimpairmentonopioidsusedto relievepainincancerpatients.PalliatMed.2011;25:604---5. 37.MuijsersRB, Wagstaff AJ. Transdermal fentanyl: an updated
review of its pharmacological properties and therapeutic efficacy in chronic cancer pain control. Drugs. 2001;61: 2289---307.
38.SkorpenF,LaugsandEA,KlepstadP,etal.Variableresponseto opioidtreatment:anygeneticpredictorswithin sight?Palliat Med.2008;22:310---27.
39.DroneyJ,Riley J.Recentadvancesin theuseofopioidsfor cancerpain.JPainRes.2009;2:135---55.
40.OverholserBR,Foster DR. Opioidpharmacokinetic drug-drug interactions.AmJManageCare.2011;17Suppl.11:S276---87. 41.Afilalo M, Stegmann JU, Upmalis D. Tapentadol immediate
release:anewtreatmentoptionforacutepainmanagement.J PainRes.2010;3:1---9.
42.FillingimRB,KingCD,Ribeiro-DasilvaMC,etal.Sex,gender, andpain:areviewofrecentclinicalandexperimentalfindings. JPain.2009;10:447---85.
43.GreenspanJD,CraftRM,LeRescheL,etal.Studyingsex and genderdifferencesinpainandanalgesia:aconsensusreport. Pain.2007;132Suppl.1:S26---45.
44.HurleyRW,AdamsMC.Sex,gender,andpain:anoverviewofa complexfield.AnesthAnalg.2008;107:309---17.
45.Hale M,Upmalis D,OkamotoA, et al. Tolerability of tapen-tadolimmediate releaseinpatientswithlowerbackpainor osteoarthritisofthehiporkneeover90days:arandomized, double-blindstudy.CurrMedResOpin.2009;25:1095---104. 46.Wesson DR, Ling W. The Clinical Opiate Withdrawal Scale
(COWS).JPsychoactDrugs.2003;35:253---9.
47.HandelsmanL,CochraneKJ,AronsonMJ,etal.Twonew rat-ing scales for opiate withdrawal. Am J DrugAlcohol Abuse. 1987;13:293---308.
48.ChouR,FanciulloGJ,FinePG,etal.Clinicalguidelinesforthe useofchronicopioidtherapyinchronicnoncancerpain.JPain. 2009;10:113---30.
49.Butler SF, Budman SH, Fernandez K, et al. Validation of a screener and opioid assessment measure for patients with chronicpain.Pain.2004;112:65---75.
50.ButlerSF,FernandezK,BenoitC,etal.Validationoftherevised ScreenerandOpioidAssessmentforPatientswithPain (SOAPP-R).JPain.2008;9:360---72.
51.Webster LR, Webster RM. Predicting aberrant behaviors in opioid-treated patients: preliminary validation ofthe Opioid RiskTool.PainMed.2005;6:432---42.
52.BelgradeMJ,SchamberCD,LindgrenBR.TheDIREscore: pre-dictingoutcomesofopioidprescribingforchronicpain.JPain. 2006;7:671---81.
53.CouwenberghC,VanDerGaagRJ,KoeterM,etal.Screening forsubstanceabuseamongadolescentsvalidityofthe CAGE-AIDinyouthmentalhealth care.SubstUse Misuse.2009;44: 823---34.