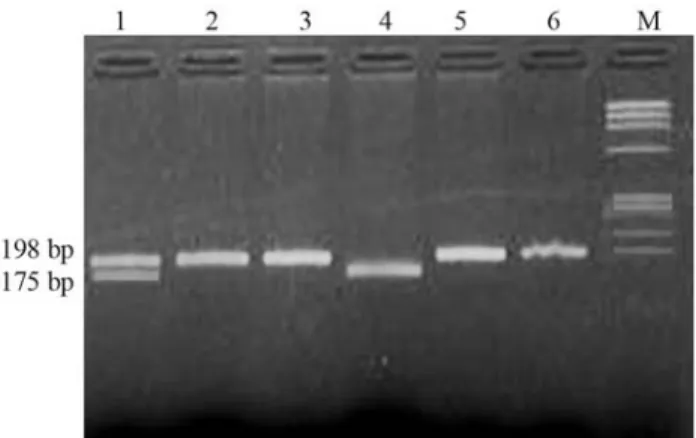
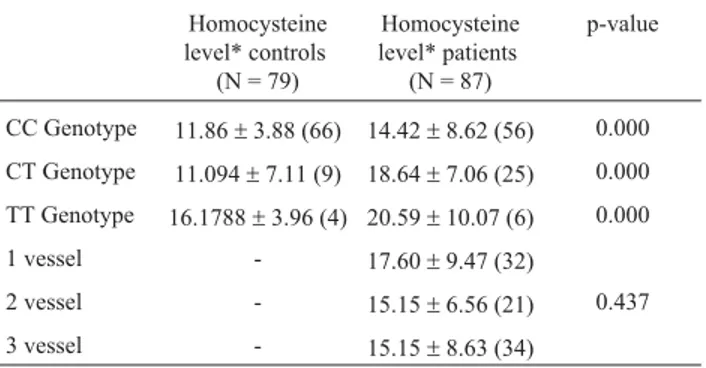
Association of homocysteine and methylene tetrahydrofolate reductase (MTHFR C677T) gene polymorphism with coronary artery disease (CAD) in the population of North India
Texto
Imagem

Documentos relacionados
Constatado os diferentes usos das terras e o predomínio de áreas destinadas a agricultura e urbano, a averiguação dessas influencia sobre a qualidade da
Il mettra au point, au fil des années, un véritable modèle d’intervention auprès des établissements scolaires, touchant au cours de campagnes de grande ampleur et de
polymorphisms, we evaluated the influence of C677T and A1298C polymorphisms in the methylenetetrahydrofolate reductase gene (MTHFR), of A2756G polymorphism in the methionine
tetrahydrofolate reductase gene C677T and A1298C polymorphisms, plasma homocysteine, folate, and vitamin B12 levels and the extent of coronary artery disease. Muniz MTC, Siqueira
ABSTRACT - Objective: To investigate the association between total plasma homocysteine concentration, C677T and A1298C polymorphisms in MTHFR gene and Alzheimer´s disease
Objective: To establish the degree of association between cardiovascular risk factors and the presence of coronary artery disease (CAD) in a group of patients undergoing
Objective: To determine plasma homocysteine levels and the incidence of methylenetetrahydrofolate reductase (MTHFR) gene C677T polymorphism in a group of subjects who
In a previous study, we have reported a significantly lower control of anger in patients with coronary artery disease (CAD), independently of the traditional risk factors,
