www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Arteriovenous
malformation
of
the
external
ear:
a
clinical
assessment
with
a
scoping
review
of
the
literature
夽
Shin
Hye
Kim
a,b,
Seung
Hoon
Han
b,
Yoonjae
Song
b,
Chang
Sik
Park
c,
Jae-Jin
Song
b,∗aKoreaUniversityMedicalCenter,KoreaUniversityCollegeofMedicine,DepartmentofOtorhinolaryngology-HeadandNeck
Surgery,Seoul,RepublicofKorea
bSeoulNationalUniversityBundangHospital,SeoulNationalUniversityCollegeofMedicine,Departmentof
Otorhinolaryngology-HeadandNeckSurgery,Seongnam,RepublicofKorea
cSeoulNationalUniversityBundangHospital,SeoulNationalUniversityCollegeofMedicine,DepartmentofPlasticSurgery,
Seongnam,RepublicofKorea
Received20May2016;accepted20September2016 Availableonline17October2016
KEYWORDS Ear;
Tinnitus; Arteriovenous malformations; Embolization, therapeutic; Surgicalprocedures, operative
Abstract
Introduction:AuricularArteriovenousMalformationoftheexternalearisararelyencountered disease;inparticular,arteriovenousmalformationarisingfromtheauricle,withspontaneous bleeding,hasseldombeenreported.
Objective: Inthecurrentstudy,wereportanunusualcaseoflate-onsetauriculararteriovenous malformationoriginatingfromtheposteriorauriculararterythatwasconfirmedbycomputed tomographic angiography.The case was successfully managed by pre-surgical intravascular embolizationfollowedbytotallesionexcision.Promptedbythiscase,wealsopresentascoping reviewoftheliterature.
Methods:Acaseofa60year-oldmanwithrightauriculararteriovenousmalformationtreatedin ourtertiarycarecenter,and52patientswithauriculararteriovenousmalformationdescribedin 10casereportsandaretrospectivereviewarepresented.Auriculararteriovenousmalformation canmanifestasswellingoftheear,pulsatiletinnitus,pain,and/orbleeding.Onphysical exami-nation,apulsatileswellingand/oratendermassisevident.Whenarteriovenousmalformationis suspected,thelesionsshouldbevisualizedusingimagingmodalitiesthatoptimallydetect vascu-larlesions,andmanagedviaembolization,massexcision,orauricularresection.Effectiveness ofthevariousdiagnosticmethodsusedandthetreatmentoutcomeswereanalyzed.
夽 Pleasecitethisarticleas:KimSH,HanSH,SongY,ParkCS,SongJ-J.Arteriovenousmalformationoftheexternalear:aclinicalassessment
withascopingreviewoftheliterature.BrazJOtorhinolaryngol.2017;83:683---90.
∗Correspondingauthor.
E-mail:[email protected](J.Song).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.09.004
Results:Various imaging modalities including Doppler sonography, computed tomographic angiography,magneticresonanceangiography,and/ortransfemoralcerebralangiographywere usedtodiagnose38casesreportedintheliterature.Inanother15cases,noimagingwas per-formed;treatmentwasdeterminedsolelybyphysicalexaminationandauscultation.Ofthetotal of53cases,12werenottreated(theirsymptomsweremerelyobserved)whereas20underwent therapeuticembolization.Intotal,32patients,including1patientwhowasnottreatedand10 withpersistentoraggravatedarteriovenousmalformationafterpreviousembolization, under-went massexcisionorauricularresectiondependingon theextent ofthe lesion.Nomajor postoperativecomplication wasrecorded.Thepostoperativefollow-upduration variedfrom 1monthto19years,andonlyonecaseofunresectable,residualcervicofacialarteriovenous malformationwasrecorded.
Conclusion:Auriculararteriovenousmalformationisararelyencountereddisease,butshould besuspectedifapatientpresentswithaswollenearandpulsatiletinnitus.Appropriateimaging isessentialfordiagnosisandevaluationoftheextentofdisease.Asembolizationaffordsonly relativelypoorcontrol,totalsurgicalremovalofthevascularmassisrecommended.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http://
creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE Orelha;
Zumbido; Malformac¸ões arteriovenosas; Embolizac¸ão, terapêutica; Procedimentos cirúrgicos, operatórios
Malformac¸ãoarteriovenosadaorelhaexterna:avaliac¸ãoclínicacomrevisão abrangentedaliteratura
Resumo
Introduc¸ão:Malformac¸ãoArteriovenosaAuriculardaorelhaexternaéumadoenc¸araramente observada,emparticular,naregiãodaaurícula,comhemorragiaespontânea,temsido infre-quentementerelatada.
Objetivo:No presente estudo, relatamos um caso incomum de malformac¸ão arteriovenosa auricular de início tardio originária da artéria auricular posterior confirmada por angioto-mografiacomputadorizada.Ocasofoicontroladocomsucessoporembolizac¸ãoendovascular pré-cirúrgicaseguidaporexcisãocompletadalesão.Alémdisso, nóstambémapresentamos umarevisãoabrangentedaliteratura.
Método: Umhomemde 60 anosde idade commalformac¸ãoarteriovenosa auriculardireita tratado em nossocentrode atendimentoterciárioe52 pacientescommalformac¸ão arteri-ovenosaauriculardescritosem10relatosdecasoseumestudoderevisãosãoapresentados. Amalformac¸ãoarteriovenosaauricularpodemanifestar-secomoinchac¸odaorelha,zumbido pulsátil,dore/ousangramento.Aoexamefísico,umedemapulsátile/ouumamassasensívelé evidente.Quandohásuspeitademalformac¸ãoarteriovenosa,aslesõesdevemservisualizadas usandomodalidadesdeimagemquedetectamdemaneiraidealaslesõesvasculares,etratadas pormeiodeembolizac¸ão,excisãototaldalesão,ouressecc¸ãoauricular.Aeficáciadosvários métodosdediagnósticoutilizadoseosdesfechosdotratamentoforamanalisados.
Resultados: Várias modalidades de imagem, incluindo ultrassonografia Doppler, angiotomo-grafia computadorizada, angiografia por ressonância magnética e/ou angiografia cerebral transfemoralforamusadaspara diagnosticar38 casosrelatados naliteratura.Em outros15 casos,nenhumaimagemfoirealizada;otratamentofoideterminadounicamentepeloexame físicoeausculta.Dototalde53 casos,12 nãoforamtratados(osseussintomasforam ape-nasobservados),enquantoque20foramsubmetidosaembolizac¸ãoterapêutica.Nototal,32 doentes,incluindoumpacientequenãofoitratadoe10commalformac¸ãoarteriovenosa per-sistenteouagravadaapósaembolizac¸ão anterior,foramsubmetidos aexcisãocompletada lesãoouressecc¸ãoauricular,dependendodaextensãodalesão.Nenhumacomplicac¸ão pós-operatóriaimportantefoiregistrada.Otempodeseguimentopós-operatóriovarioude1mês a19anos,eapenasumcasodemalformac¸ãoarteriovenosacervicofacialirressecável,residual foiregistrado.
Conclusão:A malformac¸ão arteriovenosa auricular é uma doenc¸a raramente encontrada, mas deve ser suspeitada se um paciente apresentar orelha inchada e zumbido pulsátil. A imagemapropriadaéessencialparaodiagnósticoeavaliac¸ãodaextensãodadoenc¸a.Comoa embolizac¸ãoproporcionaapenasumcontrolerelativamenteprecário,aremoc¸ãocirúrgicatotal dalesãovascularérecomendada.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http://
Introduction
An Arteriovenous Malformation (AVM)is an abnormal con-nectionbetweenoneormorearteriesandveins,bypassing thecapillarysystem.1Inmostcases,theAVMarisesfromthe
intracranialarea,butoccasionallyoriginatesfrom extracra-nialvessels.2Inaretrospectivereviewof81patientswith
AVMofthehead-and-neck,themostcommonsitewasthe cheek(31%),followedbyanear(16%).3TheAVMisalmost
alwayspresentatbirth,butmanifestslaterinlife.
Here,wereportanunusualcaseoflate-onsetauricular AVMoriginatingfromtheposteriorauricularartery.Also,a scopingreviewoftheliteratureallowsustodiscusstheroles playedbyimaginginthediagnosisandmanagementofAVM.
Materials
and
methods
Searchcriteria
We adhered tothe PRISMA(Preferred ReportingItems for SystematicReviewsandMeta-Analyses)guidelinewhen per-forming PubMed (http://www.ncbi.nlm.nih.gov/pubmed/) searchestoidentifyallstudiesonAVMoftheexternalear.4
Thekeywordsusedwere‘‘arteriovenousmalformation’’and ‘‘ear’’,andthesearchwaslimitedtoarticlesintheEnglish language.AVMsoriginatingfromtheexternalauditorycanal, orthepre-orretro-auricularareas,wereexcluded.
Ourcaseandliteraturereview
Wetreateda60year-oldmanwithright-sideauricularAVM. The study wasapproved bythe institutionalreview board of the Clinical Research Institute at our center (B-1601-329-002).Theliteraturereviewidentifiedatotalof52AVM patientsdescribedin11reports(10casereportsand1 retro-spectivereview).The10casereportsdealtwith11casesof auricularAVMandthesinglereviewanalyzed41cases.The chiefcomplaints,durationofsymptoms,eventsthat aggra-vatedthe AVMs,and historyof spontaneousAVM bleeding wereanalyzed.
Diagnosticprocessanddifferentialdiagnosis
The laterality, location, and extent of AVM were inves-tigated. Various diagnostic imaging modalities including DopplerSonography(DS),TemporalBoneComputed Tomo-graphic Angiography(TBCTA),Magnetic Resonance Angiog-raphy (MRA), and/or Transfemoral Cerebral Angiography (TFCA)wereemployedinindividualcases,andthefindings ofthekeydiagnosticmodalitieswerereviewed.Inpatients who underwentdiagnostic angiography, the main arteries andfeedervesselsaresummarized.
Managementoptionsandtreatmentoutcomes
The AVM management options included observation, embolization, mass excision, or auricularresection. After the treatment, the clinical condition was described as controlled, improved, persistent, or aggravated. We also exploredtheapplicationofreconstructiveproceduressuch
as Skin-Thickness Split Grafting (STSG) and total auricu-larreconstruction. Postoperative complications, follow-up durations,andfinalstatuswerereviewed.
Results
Ourexperiencewithlate-onsetAVM
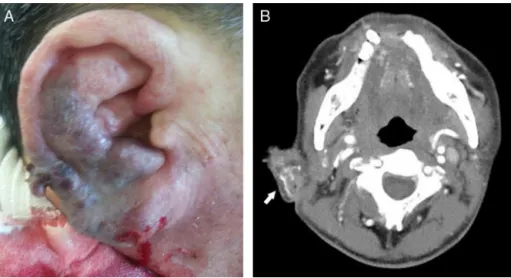
A60year-oldmanvisitedtheemergencydepartmentwith massivespontaneousbleedingfromtherightear.Hehada historyofrecurrentswellingof theright auricle,and pul-satiletinnitus.Threeyearsprior,thepatienthadvisitedour outpatientclinicwithrecurrentauricularswelling,andwas diagnosedwithanotohematomabecauseofthe cauliflower-likeappearanceoftheauricle.
On physical examination, the right auricle exhibited excessiveswellinganddiscoloration(Fig.1A).Thetympanic membraneandexternalauditorycanalwerenormal.TBCTA revealedenlargementoftherighthelix,andanentangled vascular lesion (Fig. 1B). We suspected an auricular AVM andperformedtransarterial embolizationusingTFCA.The principalAVM-feeding arteryoriginatedfromtheposterior auricularartery, andwe completely embolized theartery withglue(Fig.2A).Afterembolization,bleedingwas con-trolled,butischemicnecrosisoftheauricularskindeveloped (Fig.2BandC).Twoweekslater,thenecroticskinboundary becamedistinct(Fig.3A),andwethus plannedtotalmass excision.
Under local anesthesia, the skin wasincised along the verticalplane of the right auricle andthe AVM mass was totallyexcised (Fig. 3B). The adjacent necrotic skin was excisedand primaryclosure wasperformed (Fig.3C).The patientrecovered withoutanycomplications.At6months postoperatively, the auricle was well-healed without any evidenceofrecurrence.
DemographicsandsymptomsofAVMpatients
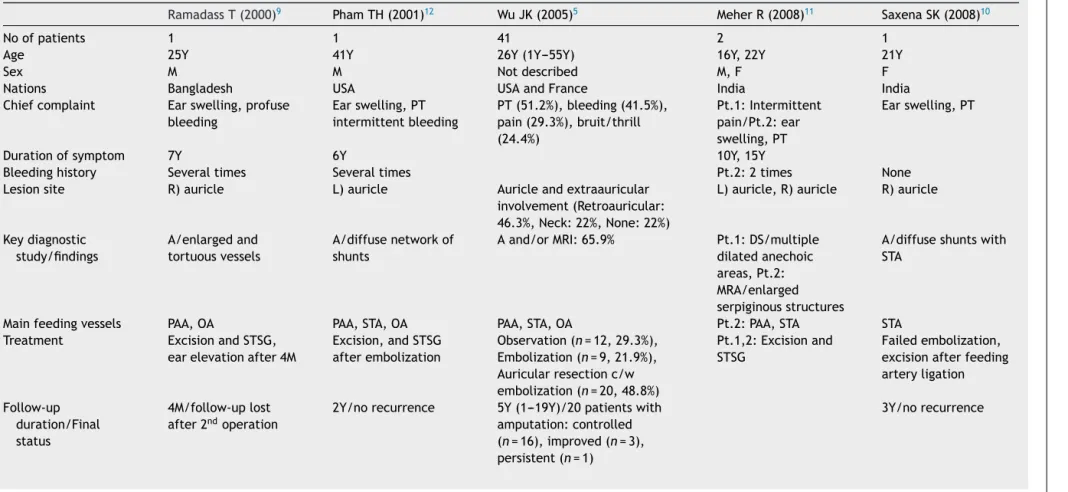
Table1summarizes the findingsof 12studies on53cases ofauricularAVM.1,5,6 Of 11case reports, 7 weremenand
4werewomen,withamedianageof21(15---45)years.In theretrospective review of 41 cases, themale-to-female patientratio was not mentioned, and the mean age was 26(1---55)years.Chiefcomplaintswereswellingoftheear, pulsatile tinnitus,intermittent pain, hearing loss, and/or profusespontaneousbleeding.Abouttwo-thirdsofpatients reported that their symptoms had commenced at a very youngage.SevenpatientsreportedthattheirAVMsbecame aggravatedduringpuberty,and6hadhistoriesoftrauma.
Diagnosis
Table1showskeydiagnosticstudyandtheirfindings.In38 ofthe53cases,DS,TBCTA,MRA,and/orTFCAweresilent in terms of diagnosis. No imaging was performed in the other15cases;treatment wasdeterminedsolelyby phys-icalexamination and auscultation.5,7 On angiography, the
Figure1 Grossfindings andtemporalbonecomputedtomographic angiographyfindings ontheearofa60year-old man,as recordedintheemergencyroom:(A)thepatientpresentedwithaswollenearandspontaneousmassivebleeding;(B)temporal bonecomputedtomographicangiographyrevealedaright-side,auricularvasculartangledlesion(whitearrow).
Figure2 Preoperative therapeutic embolizationusing transfemoralcerebral angiographyandgross earfindings 3days after embolization:(A)transfemoralcerebralangiographyrevealedlargetortuousvesselsandinnumerablesmallvessels.Theprincipal feedervesselofthearteriovenousmalformationoriginatedfromtheposteriorauricularartery(blackarrow),andwascompletely occludedwithglue;(B)and(C)afterembolization,thebleedingstopped,butischemicnecrosisoftheskinprogressed.
Managementandtreatmentoutcomes
The flowchartof Fig.4 shows thetreatment optionsand outcomes.Twelveof53patientswereinitiallyfollowed-up withoutanytreatment.Ofthese,AVMspersistedin10,and became aggravatedin 2. Of the latter 2, one underwent auricular resection but the other rejected an operation. Twenty patients underwent therapeutic embolization. Of these,theAVMsimprovedin3, butbecameaggravatedin 17. Of thelatter 17, 10 underwentAVM mass excision or auricularresection.
Atotal of21 patients underwentAVMmass excision or auricularresectionasinitialtreatment. Ofthesepatients, plus afurther 11 whounderwent excision or resection as salvagemanagement,22(69%)werecontrolledand9(28%) improved,andonlyonehadapersistentunresectableAVMin theadjacentregion.Inthese32patients,woundclosurewas performed bysimple linearclosure (n=18);STSG(n=10);
immediatereconstructionusingsalvagedauricular cartilagi-nous framework covered by temporoparietal flap (n=1), expanded local flap (n=1), advancementflap (n=1), and freeflap(n=1).Onepatientunderwentatwo-staged oper-ation:auricularresectionandSTSGinitiallyandearlobule creationandearelevationsecondarily.8Nomajor
postopera-tive complicationwasnoted,except fortransient tinnitus in onepatientandskin necrosisat thesite ofwound clo-sure in two.7 The postoperativefollow-up durationvaried
from1month to19years,andonlyonecase hadresidual cervicofacialAVM.7
Discussion
Figure3 Grossearfindingsat2weeksafterembolizationandtotalexcisionofthearteriovenousmalformation.(A)Twoweeks aftertransarterialembolization,theboundaryofthenecroticskinlesionbecamedistinct.(B)Thenecroticskinandthemassof thearteriovenousmalformationwasexcisedunderlocalanesthesia.Thedimensionsofthemasswere4.8cm×1.2cm×1.2cm.(C) Theauriclewasclosedunderminimaltension.
Stage III (destruction) is characterized by pain, ulcera-tion, and bleeding; whereas stage IV (decompensation) featurescardiacfailure.3,9 Thepresentingsignsand
symp-tomscorrelatewiththestageofAVM.AlthoughmanyAVMs are asymptomatic, they may alternatively trigger severe pain and/or bleeding. The most common symptoms are pulsation(51.2%),bleeding(41.5%),andpain(29.3%).7
Hear-ing canalso deteriorate,presumably because thebruit is audible.10---13Thereare2typesofAVMwithregardtotheflow
rate: fast-flowing andslow-flowing.14 Most of fast-flowing
regions arearteriovenous fistulas whereasslow-flow AVMs areproduced by venous, capillary, or lymphatic lesions.14
This flow rate-based classification may be of impor-tance as different treatment options are needed for the 2types.
Enlargement of an AVM may be triggered by trauma, infection,orhormonalinfluences.15 Inthereviewpaperof
41AVMpatients,expansionoccurredduringchildhoodin7, adolescencein14,pregnancyin10,andadulthoodin10.7
Some AVMs may remain quiescent until adolescence and, evenintoadulthood.Ourpatientwasratherolderthanthose ofotherreports.Moreover,wehadearliermisdiagnosedthe lesionasanotohematoma.AVMissimilartocauliflowerear inthatbothdiseasesmaypresentwithaswollendeformed auricle.Assimpledrainagebasedonamisdiagnosisof oto-hematomamaytrigger massivebleedinginacase ofAVM, differentialdiagnosisofAVMfromanotohematomais impor-tant.
In twocase reports, surgical intervention wasplanned undersuspicionofAVMintheabsenceofimagingdata.2
How-ever,imagingmodalitiesarerequiredforaccuratediagnosis ofthevascularlesionandconfirmationoftheextent.MRA orTFCA revealed totalauricularinvolvement in 24(89%), although56.1%of27patientswerethoughttoexhibitonly partialinvolvement upon physical examination.7 Although
conventional TFCA is invasive, the technique is useful to identify the principal feeding vessel and an appropri-ate embolization portal.15 TFCA-guided embolization is a
53 cases with auricular AVM
12 cases: Observation
10 cases: Persistent
2 cases: Aggravated
20 cases: Embolization
17 cases: Aggravated or persistent 32 cases:
Mass excision or auricular resection
1 case: Persistent
22 (controlled) 9 (improved)
10 cases
21 cases 3 (improved)
1 case
Ki
m
SH
et
al.
Table1 Summaryofcasesshowingarteriovenousmalformationoftheexternalearfrompreviousreportedliteraturesandthisstudy.
RamadassT(2000)9 PhamTH(2001)12 WuJK(2005)5 MeherR(2008)11 SaxenaSK(2008)10
Noofpatients 1 1 41 2 1
Age 25Y 41Y 26Y(1Y---55Y) 16Y,22Y 21Y
Sex M M Notdescribed M,F F
Nations Bangladesh USA USAandFrance India India
Chiefcomplaint Earswelling,profuse bleeding
Earswelling,PT intermittentbleeding
PT(51.2%),bleeding(41.5%), pain(29.3%),bruit/thrill (24.4%)
Pt.1:Intermittent pain/Pt.2:ear swelling,PT
Earswelling,PT
Durationofsymptom 7Y 6Y 10Y,15Y
Bleedinghistory Severaltimes Severaltimes Pt.2:2times None
Lesionsite R)auricle L)auricle Auricleandextraauricular involvement(Retroauricular: 46.3%,Neck:22%,None:22%)
L)auricle,R)auricle R)auricle
Keydiagnostic study/findings
A/enlargedand tortuousvessels
A/diffusenetworkof shunts
Aand/orMRI:65.9% Pt.1:DS/multiple dilatedanechoic areas,Pt.2: MRA/enlarged serpiginousstructures
A/diffuseshuntswith STA
Mainfeedingvessels PAA,OA PAA,STA,OA PAA,STA,OA Pt.2:PAA,STA STA Treatment ExcisionandSTSG,
earelevationafter4M
Excision,andSTSG afterembolization
Observation(n=12,29.3%), Embolization(n=9,21.9%), Auricularresectionc/w embolization(n=20,48.8%)
Pt.1,2:Excisionand STSG
Failedembolization, excisionafterfeeding arteryligation
Follow-up duration/Final status
4M/follow-uplost after2ndoperation
2Y/norecurrence 5Y(1---19Y)/20patientswith amputation:controlled (n=16),improved(n=3), persistent(n=1)
malformation
of
the
external
ear
689
Table1 (Continued)
WooHJ(2008)13 WhittyLA(2009)8 PrasadKC(2011)14 GoelA(2011)15 MeenaBK(2013)1 DixitSG(2013)6 KimSH(thisstudy)
Noofpatients 1 1 1 1 1 1 1
Age 20Y 15Y 45Y 22Y 21Y 21Y 60YA
Sex M M M F F M M
Nations Korea USA India India India India Korea
Chiefcomplaint PT Earswelling, intermittentpain
Earswelling Earswelling,PT Earswelling,PT Earswelling Earswelling, massivebleeding, PT
Durationofsymptom 7M 2Y 2-3Y 4Y 1Y Sincebirth 3Y
Bleedinghistory None 2times 2times None
Lesionsite L)auricle L)auricle R)auricle L)auricle R)auricle
Keydiagnostic study/findings
MRI/abnormalsignal voidingintensityof themass
Auscultation/audible bruit
A/AVMmassand PAAaneurysm
DS DS,CTA/enlarged serpiginous structures
MRA/abnormal tortuousvessel
CTA/innervascular tangledlesion
Mainfeedingvessels PAA,STA PAA PAA,STA PAA PAA
Treatment Failedembolization, excision
Excision Vesselligationand massexcision
ExcisionandSTSG Excision Embolization underexternal approach
Excisionafter embolization
Follow-up duration/final status
2Y/norecurrence 1M/norecurrence 2Y/norecurrence 3M/norecurrence
useful initial therapeutic step, but surgical excision is requiredinmostcasestoavoidrecurrence.
Treatment isunnecessary (especiallyin children)ifthe AVM is small and asymptomatic. In an untreated group of 12 patients, 2 of stage I and 7 of stage II remained stable.3,7 If the AVM is symptomatic, complete excision
(preceded by embolization) is the treatment of choice.6
Ligation of the arterial vessels alone or partial excision should be avoided, because a new collateral circula-tion will form,triggering further enlargement.15,16 In our
scoping review, 17 of 20 patients who underwent initial embolizationexhibitedaggravatedor persistentAVMs.Wu etal. reported that the mean lag timebetween the last embolizationandultimateresectionwas5.6years(range: 2---8 years).5 Based on these results, embolization is best
employedonly toreduceblood lossandfacilitate surgical extirpation.
Conclusion
Our case was initially misdiagnosed as an otohematoma becauseofthecauliflower-likeauricle,andthepatient pre-sented3 yearslater withmassivebleeding. To accurately diagnose anAVM, meticulousphysical examination includ-ingpalpation and auscultation and imaging areessential. In most cases of auricular AVM, optimal treatment is a combinationofsuper-selectiveembolizationandcomplete surgicalexcision.
Funding
ThisworkwassupportedbyagrantfromtheKoreaHealth Technology R&D Project through the Korea Health Indus-try Development Institute (KHIDI), fundedby the Ministry of Health & Welfare, Republic of Korea (grant number HI14C2264).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Meher R, Varshney S, Pant HC. Arteriovenous malformation relatedtothepinna.HongKongMedJ.2008;14:157---9.
2.RaghuM,DeR,HigginsN,AxonP.Spontaneousarteriovenous malformationoftheexternalauditorymeatus.JLaryngolOtol. 2004;118:912---3.
3.Kohout MP, HansenM, Pribaz JJ,Mulliken JB. Arteriovenous malformationsoftheheadandneck:naturalhistoryand man-agement.PlastReconstrSurg.1998;102:643---54.
4.MoherD,LiberatiA,TetzlaffJ,AltmanDG,GroupP.Preferred reportingitemsforsystematicreviewsandmeta-analyses:the PRISMAstatement.IntJSurg.2010;8:336---41.
5.WhittyLA,MurrayJD,NullWE,ElwoodET,JonesGE.An arte-riovenous malformationof theexternal ear in the pediatric population:acasereportandreviewoftheliterature.CanJ PlastSurg.2009;17:e45---7.
6.PhamTH, WongBJ,Allison G. Alargearteriovenous malfor-mationoftheexternalear inanadult:reportofa caseand approachtomanagement.Laryngoscope.2001;111:1390---4. 7.WuJK,BisdorffA,GelbertF,EnjolrasO,BurrowsPE,Mulliken
JB.Auriculararteriovenousmalformation:evaluation, manage-ment,andoutcome.PlastReconstrSurg.2005;115:985---95. 8.RamadassT,SridharK,KrishnanG,SekharPM,Narayanan N.
Arteriovenousmalformationwithauricularhypertrophy.Indian JOtolaryngolHeadNeckSurg.2000;52:307---9.
9.SecciaA,SalgarelloM,FaralloE,FalappaPG.Combined radio-logicalandsurgicaltreatmentofarteriovenousmalformations oftheheadandneck.AnnPlastSurg.1999;43:359---66. 10.SongJJ,AnGS,ChoiI,DeRidderD,KimSY,ChoiHS,etal.
Objec-tificationanddifferentialdiagnosisofvascularpulsatiletinnitus bytranscanalsoundrecordingandspectrotemporalanalysis:a preliminarystudy.OtolNeurotol.2016;37:613---20.
11.Kim SH, An GS, Choi I, Koo JW, Lee K, Song JJ. Pre-treatment objective diagnosis and post-treatment outcome evaluation in patients with vascular pulsatile tinnitus using transcanalrecordingandspectro-temporalanalysis.PLoSOne. 2016;11:e0157722.
12.KimCS,KimSY,ChoiH,KooJW,YooSY,AnGS,etal. Transmas-toidreshapingofthesigmoidsinus:preliminarystudyofanovel surgicalmethodtoquietpulsatiletinnitusofanunrecognized vascularorigin.JNeurosurg.2016;152:441---9.
13.SongJJ,KimYJ, KimSY, AnYS,Kim K,Lee SY,et al. Sinus wallresurfacingforpatientswithtemporalbonevenoussinus diverticulum and ipsilateral pulsatile tinnitus. Neurosurgery. 2015;77:709---17.
14.GuptaR, AgrawalA. Arteriovenousmalformationofexternal ear and temporalregion: a casereport. Int J Res MedSci. 2015;3:3427---9.
15.SaxenaSK,GopalakrishnanS,MegalamaniSB,KannanS, Shan-mugapriyaJ.Arteriovenousmalformationoftheexternalear. IndianJOtolaryngolHeadNeckSurg.2008;60:177---8.