www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Evaluation
of
cytokines
produced
by

-hemolytic
streptococcus
in
acute
pharyngotonsillitis
夽,夽夽
Sydney
Correia
Leão
a,∗,
Ivanna
Oliveira
Leal
b,
Hertaline
Menezes
do
Nascimento
Rocha
b,
Tania
Maria
de
Andrade
Rodrigues
baUniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
bPost-GraduatePrograminBiology(PROBP-UFS),UniversidadeFederaldeSergipe(UFS),SãoCristóvão,SE,Brazil
Received23April2014;accepted24August2014
Availableonline10June2015
KEYWORDS
Pharyngitis; Cytokines; Streptococcus
Abstract
Introduction:ThemostcommonpathogeninbacterialpharyngotonsillitisisgroupA-hemolytic streptococcus,althoughgroupsB,C,F,andGhavealsobeenassociatedwithpharyngotonsillitis. Objective:ToassessthelevelsofthecytokinesTNF-␣,IL-6,IL-4,andIL-10inbacterial pharyn-gotonsillitiscausedbygroupAandnon-A(groupsB,C,FandG)-hemolyticstreptococcus. Methods:Thestudywasconductedatapediatricemergencycareunit.Thesamplecomprised children(5---9yearsold)withacutebacterialpharyngotonsillitisdiagnosedbetweenDecember of2011andMayof2012.Theresearchinvolvedcollectionofbloodsamplesfromthepatients, enzyme-linkedimmunosorbentassaydetectionofTNF-␣,IL-6,IL-4,andIL-10,andcollectionof twooropharyngealswabsforbacterialisolation.Additionally,themedicalhistoryofthestudy participantswasalsocollected.
Results:Inthestudiedgroup(meanage:5.93years),higherpharyngotonsillitisincidencewas observedinthefemalegender(64.76%).Higherincidenceoftonsillarexudateswasobserved withgroupsAandC.Nostatisticallysignificantdifferencesincytokinelevelswereobserved amonggroups.However,thegroupAandthecontrolgroupshowedadifferenceintheIL-6level (p=0.0016).
Conclusions:TheGroupsAandCshowedhighercytokinelevelsthantheGroupsBandcontrol, suggestingsimilarimmunologicalpatterns.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:LeãoSC,LealIO,RochaHMN,RodriguesTMA.Evaluationofcytokinesproducedby-hemolyticstreptococcus inacutepharyngotonsillitis.BrazJOtorhinolaryngol.2015;81:402---7.
夽夽
Institution:MolecularAnatomyGroup,DepartmentofMorphology,UniversidadeFederaldeSergipe(UFS),SãoCristóvão,SE,Brazil. ∗Correspondingauthor.
E-mail:[email protected](S.C.Leão). http://dx.doi.org/10.1016/j.bjorl.2015.05.003
PALAVRAS-CHAVE
Faringite; Citosinas; Streptococcus
Avaliac¸ãodascitosinasproduzidasporestreptococos-hemolíticosem faringotonsilitesagudas
Resumo
Introduc¸ão: Opatógenomaiscomumenteassociadoàfaringotonsilitebacterianaéo estrepto-coco-hemolíticodogrupoA,adespeitodosgruposB,C,FeGteremtambémsidoassociados comafaringotonsilite.
Objetivo: DeterminarosníveisdascitosinasTNF-␣,IL-6,IL-4,eIL-10nafaringotonsilite bac-terianacausadapelosestreptococos-hemolíticosdogrupoAenão-A(gruposB,C,FeG). Método: Oestudo foi conduzidoem uma emergência pediátrica.A amostra estudada com-preendeucrianc¸as(entre5e9anos)comfaringotonsiliteagudabacterianadiagnosticadaentre dezembrode2011emaiode2012.Apesquisaenvolveuacoletadeamostrassanguíneasdos pacientes,adetecc¸ão,atravésdoELISA,deTNF-␣,IL-6,IL-4eIL-10,alémdacoletadedois swabsorofaríngeosparaisolamentobacteriano.Adicionalmentefoicoletadaahistóriamédica dosparticipantesdoestudo.
Resultados: Nogrupoestudado(idademédia:5,93anos),amaiorincidênciadefaringotonsilites foiobservadanogênerofeminino(64,76%).Foramdetectadasmaioresincidênciasdeexsudatos tonsilaresnosgruposAeC.Nãoforamobservadasdiferenc¸asestatisticamentesignificantesdos níveisdecitosinasentreosgrupos.PorémosgruposAeocontrolemostraramdiferenc¸anos níveisdeIL-6(p=0.0016).
Conclusões: OsgruposAeCmostrarammaioresníveisdecitosinasqueosgruposBeocontrole, sugerindomecanismosimunológicossimilares.
©2015Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Acutepharyngotonsillitis(PT) is one ofthe most common
conditions observed by pediatricians,
otorhinolaryngolo-gists,andprimarycarephysiciansintheirdailypractice.Itis estimatedthat>50%ofcasesofPTareofviralorigin;among
thebacterialcases,themostcommonpathogenisgroupA
-hemolytic streptococcus(GAS).1---3However,-hemolytic
streptococcigroupsB,C,F,andG(especiallyCandG)can alsocauseself-limitingPTwithnon-suppurativesequelae, suchasrheumaticfever.4,5
In the last50 years,the overall incidence of bacterial PT causedby groupsB,C, F,and Ghasincreased.A2011 studyontheprevalenceof-hemolyticstreptococcigroups CandFinpatientswithacutepharyngitisdemonstratedthat thesemicroorganismscausePTin6.2%ofallcasesofacute streptococcalinfections.6---8
In turn, groups C and G streptococci (GCS and GGS) have been describedaspyogenes-like, astheseorganisms shareimportantvirulencefactorssuchashemolysins, strep-tolysin O, extracellular enzymes, and Mproteins, similar toGAS.TheycanalsocauseexudativeisolatedPTin addi-tiontocellulitis,thusbecomingclinicallyindistinguishable fromGAS.PreviousstudiesdemonstratedthatGCScausesa strongimmunologicalresponse,ascanbeobservedfromthe increaseinantistreptolysinO(ASO)titerduring streptococ-calinfectionoftheoropharynx.9---11GBSalsoshowsvirulence
factors similar to the GAS, including hemolysins, encap-sulatedpolysaccharides,andC5apeptidase;hyaluronidase mayalsoappearinsomestrains.12
Considering the abovementioned data on the shared virulence factors and clinically similar PT development, especiallyamong groups A, C and G, this study aimed to assessthelevelsofTNF-␣,IL-6,IL-4,andIL-10cytokinesin patientswithPT,inordertodistinguishpharyngotonsillitis causedbyGASfromnon-GAS.
Methods
Thestudywascarriedoutatanemergencyunitofthecityof Aracaju.Thestudypopulationincludedchildren(5---9years old)withacutebacterialPTdiagnosedbetweenDecember 2011andMay2012.
Sample sizecalculation wasperformed considering the overall incidence of acute PT, which according to Simões et al. (2002) in a study carried out in Portugal, was 3440.3/105 for the age group of 5---9 years.6 The
popula-tionofchildren inthisage groupin thecity ofAracaju is 40,442inhabitants,accordingtothe2010Census(Brazilian InstituteofGeographyandStatistics---IBGE,2012). Apply-ingthe incidence reportedby the abovementioned study, usingthe formula for sample size calculation for a finite population --- chi-squared --- a sample of 50 children was attained.
Theinclusioncriteriawerethefollowing:
(1) Diagnostic hypothesis of bacterial PT demonstrated by at least two symptoms: sudden odynophagia, fever,headache,nausea,vomitingandabdominalpain, pharyngotonsillar inflammation, palatal petechiae, anteriorcervicaladenitis,andscarlatiniformrash. (2) Nohistoryofcardiovasculardisease.
(3) ResidentofthemunicipalityofAracaju.
PatientswithsuspectedviralPT,withthefollowing symp-toms:conjunctivitis,rhinitis,cough, diarrhea,hoarseness, mildulcerativestomatitis,andviralrashwereexcluded.13
Thestudywasdividedintotwophases:thefirstconsisted ofbloodsamplecollectionfrompatientswithadiagnostic hypothesis ofbacterial acutePT, toperform the enzyme-linked immunosorbent assay (ELISA) test for TNF-␣, IL-6, IL-4,andIL-10cytokines,pluscollectionoftwooropharynx swabs for bacterial isolation, seeded ona petri dish con-tainingbloodagar.Thesecondphaseconsistedofindividual inquiry,whichcontaineddataonsocioeconomicstatusand thechild’shealthhistory.
Microbiologicalphase
Themethodologyforthemicrobiologicalphaseofthestudy wasdescribedbasedonModulesIIIandVofClinical Micro-biologyManual for InfectionControl in HealthServicesby theBrazilianNational HealthSurveillanceAgency(Agência NacionaldeVigilância Sanitária[ANVISA]), concerningthe microbiologicallaboratoryproceduresandidentificationof medicallyimportantbacteria,respectively.14
The oropharyngeal swabs were collected following the techniquedescribedbyLevyetal.(2004)toobtainaculture specimenforStreptococcussp.isolation.Thetechnique fol-lowed the sequence described: the patient wasasked to open his/hermouth; usinga tongue depressorand sterile swabs,smearswereobtainedfromthetonsilsandposterior pharynx,seekingtocollectthematerialfromtheareas clos-esttothesitesofsuppurationandavoidingotheroralcavity sites.14
Forthe presumptiveidentification of colonies of beta-hemolytic streptococci, the specimens were seeded on a petri dish containing blood agar using aseptic techniques andincubatedfor24hinabacteriologicalincubator,using thecandle-jartechniqueat35◦±2◦C.Afterincubation,the
coloniesweretested withcatalasetoeliminate Microcco-cacea(staphylococci),whichgenerallygiveapositiveresult forcatalaseactivity,whereasstreptococci,ingeneral,yield anegativecatalasetest.Asevidentialtest,Gramstainwas performed in catalase-negative colonies, withsubsequent visualization of the morphological and color appear-ance of the specimens under optical microscopywith oil immersion.
Afterthemicroscopicconfirmationofstreptococci,a co-agglutinationtestusingPhadebact®StrepAD,F,andGTest
---BactusABTest®wasperformed.Thecoloniesof-hemolytic
groupAstreptococci(Streptococcuspyogenes)were identi-fiedusingbacitracinataconcentrationof0.04IU,withthe formationofaninhibitionzoneasaresultofsensitivity.
Serologicalphase
Blood samples (4mL) collected from each patient were maintained in serum separator tubes and centrifuged at 5000rpmfor 15min, withthe serumseparatedintothree aliquots of 500L and stored at −80◦C. The ELISA
tech-nique was performed for all cytokines according to the manufacturer’sinstructions (ELISAReady-SET-Go!® ---
EBIO-SCIENCE).Serumcytokineconcentrationsweremeasuredin pg/mL using standard curves previously described by the manufacturer:IL-4(2---200pg/mL);IL-6(2---200pg/mL); IL-10(2---300pg/mL);andTNF-␣(2---200pg/mL).
The C-reactive protein (CRP) measurement technique wasperformed according tothe manufacturer(Turbilátex kit---BIOTÉCNICA).Essentially,the methodconsistsof the agglutination of latex particles coated with human anti-CRPantibodybytheC-reactiveprotein(CRP)presentinthe sample.Theagglutinationcausesanincreaseinabsorbance proportionaltotheconcentrationofCRPinthesample,and bycomparisonwithaknownconcentrationofCRP calibra-tor,thecontentoftheCRPintheassayedsampleat540nm canbedetermined.
Statisticalanalysis
The data were stored in a database in a Microsoft Excel spreadsheet. Forcomparison of the studied cytokines,as wellassignsandsymptomsbetweengroups,thisstudyused ANOVA and the Kruskal---Wallis test with Bonferroni’s and Dunn’spost-tests,respectively, with95% confidence inter-val.Datawere analyzedusing GraphPad-Prisma5software (GraphPadSoftware---SanDiego,CA,UnitedStates).
Ethics
ThisresearchprotocolwasapprovedbytheResearchEthics CommitteeofUniversidadeFederaldeSergipe(CEP),under No.CAAE0098.0.107.000-11.
Results
The study population consisted of 74 patients (62 symp-tomatic and 12 controls) aged 5---9 years (mean age 5.93±1.69years).Regardinggender,69.76%ofthesample consistedoffemales(p=0.03).
Regardingmicrobiologicalfindings,itwasobservedthat
Table1 Comparisonoflevelsofcytokines(pg/mL)indifferentgroupsof-hemolyticstreptococcibyanalysisofvariance.
Lancefieldgroups IL-4 IL-10 TNF IL-6
GAS 10.40±5.48 19.40±10.16 76.00±138.40 24.13±12.22
GBA 7.66±0.52 28.32±14.43 10.85±17.41 12.01±11.22
GCS 11.97±5.56 30.98±22.49 120.81±128.42 30.41±25.98
Controls 10.45±3.01 12.8±11.6 8.88±7.52 0.91±0.68
p 0.377 0.10 0.076 0.061
Referencelevels:IL-4(0---38.7pg/mL);IL-6(0---5.9pg/mL);IL-10(1.5---9.1pg/mL);andTNF␣(0---20pg/mL).
Table 2 Comparison of C-reactive protein (CRP) levels
(mg/L) bygroups ofhemolyticstreptococci incomparison tothecontrolgroupusinganalysisofvariance.
Lancefieldgroups CRP
GAS 59.67±22.99
GBS 40.50±29.17
GCS 48.50±44.55
Controls 1.10±1.19
p 0.0007
Referencelevels:CRP(<3.0mg/L).
As for serum cytokines among the different groups of
beta-hemolyticstreptococci,itwasobservedthatIL-6levels (pg/mL)weresignificantlyhigheringroupAthanincontrols
(p=0.0016). Although it did not show significantly higher
levelswhencomparedtoothergroups,meanGCSwas
sig-nificantlyhigher (30.41±25.98pg/mL), evengreater than
that shown by GAS (24.13±12.22pg/mL). Mean levelsof
GBSwerehigherthancontrols,indicatingactiveinfection;
however,theselevelswere2-to2.5-foldlowerthanthose
shownbyGASandCGS,respectively(Table1).
A similar resultwas observed for the quantificationof TNF-␣,which did not significantly differbetween groups, although GAS and GCS showed higher levels than GBS, whichweresimilartothecontrolgroup.Thelevelsof anti-inflammatorycytokinesIL-4andIL-10werealsomeasured, butshowednostatisticallysignificantdifferencesbetween thegroups,includingthecontrolgroup(Table1).
DuetoasignificantincreaseinIL-6levelscausedbyGAS infections, CRP levelswere alsomeasured, which showed asignificantincrease inlevelsof -hemolyticstreptococci inrelationtothecontrolgroup(p=0.0007);however, sta-tisticallysignificantdifferenceswerenotobservedbetween thegroups,althoughthemeanlevelsintheGASgroupwere higher thanin the others, suggesting that GAS leads to a moreintenseinflammatoryresponse(Table2).
Discussion
Thedevelopmentandregulationofanautoimmuneresponse dependoncytokineproductionandrelease,thatcan deter-mine the differentiation of antigen-specific T cells in an appropriateeffector T-cell lineage.The immune response toinfectionisregulatedbythebalancebetweenthe mech-anisms inducingthe productionof Th1and Th2cytokines. ThecytokinesderivedfromTh1(IL-2andIFN-␥)inducean immuneresponsethroughacell-dependentpathway,while
cytokinesderived fromthe Th2 type(IL-4) suppress cell-mediatedresponsepathwayandinducehumoralresponse, whichinvolvesthereleaseofIL-4,IL-5,IL-6,andIL-10.15,16
In this study, the measurement of levels of IL-4, IL-6, IL-10,and TNF-␣cytokinesin childrenwithacute pharyn-gotonsillitiscausedbybeta-hemolyticstreptococcishowed highlevels ofpro-inflammatory cytokinesIL-6and TNF-␣. However,thelevelsof anti-inflammatory cytokines, espe-ciallyIL-4,weresimilartothosefoundinthecontrolgroup, suggestingachangeinimmuneresponsemediatedbyTh1.
Thelevelsofpro-inflammatorycytokinesintheGASand GCSgroupsshowedhighermeanvaluesthanthoseintheGBS andcontrol groups; similarly, themean anti-inflammatory cytokine levels were higher in GAS and GCS groups, sug-gestingsimilarimmunologicalmechanisms.Aimingtoassess thedegreeofhomeostasisbetweentheproductionof pro-inflammatorycytokinesandanti-inflammatoryfactors,the ratioofTNF-␣inrelationtoIL-4andIL-10anti-inflammatory cytokineswascalculated.Theproportionwashigherforthe infectioncausedbyGCS,suggestingatendencytowardmore acuteimmune andinflammatory responses,withachange toTh1pattern.16
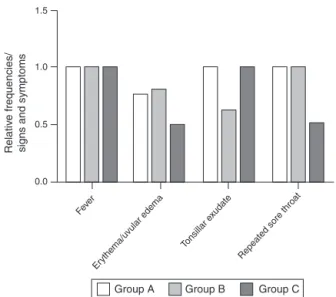
Cytokines levelsreflect the manifestation of signsand symptoms.More aggressivemanifestations were observed in patients with PT caused by GAS and GCS groups when comparedtothosecausedbyGBS,especiallyinrelationto tonsillarexudates(Fig.1).PTscausedbyGBSusuallyshow lowerlevelsofpro-inflammatorycytokineswhencompared tolevelsfoundinothergroups;thesedatasuggestaweaker immuneresponsetovirulencefactorsofthisgroup, reflect-ingmilderclinicalmanifestations15(Fig.1).
IL-6 levels in the serum of children with PT caused bybeta-hemolyticstreptococciincreasedbetweenthe dif-ferent groups when compared to the control group. IL-6 stimulates hepatocytes to produce high levels of acute-phaseproteinssuchasC-reactiveprotein(CRP)duringactive infectionoracuteinflammatoryprocess,givingitthestatus ofinflammatorymarker.17---19Inthisstudy,meanCRPlevels
inGAS werehigherthanintheother groups, suggestinga moreintenseinflammatoryresponse(Table2).
AlthoughGASandGCSsharevirulencefactorssuchasM protein,whichisconsideredthemainfactorresponsiblefor thevirulence and pathogenesis of acuterheumatic fever, GCSisnotrelatedtothisnon-suppurativecomplicationand can only be associated with acute glomerulonephritis.4,9
1.5
1.0
0.5
0.0
Group A Group B Group C
Feve r
Eryt
hema/uvular edema Tonsillar e xudate
Repeated sore throat
Relativ
e frequencies/
signs and symptoms
Figure 1 Distribution of relative frequencies of signs and
symptomsbetween different-hemolytic groups.Higher
rel-ativefrequency oftonsillarexudatesis observedingroups A
(GAS)andC(GCS).
specific circumstances, have the potential to initiate an autoimmune response, which could emulate a picture of acuterheumaticfever.20---22Thisfindingindicatestheclinical
importanceofthisbacteriumandalsothatitisappropriate toinvestigateandtreatPTcasescausedbyGCS,aswellas byGAS.
Conclusion
It can be concluded that PT caused by GAS, GBS, and GCS showed representative incidences and similar signs and symptoms. However, PT caused by GAS and GCS are more acute, as demonstrated by the immune response andthehighlevelsofpro-inflammatorycytokines, suggest-ingthatimmunologicalmechanismsaresimilarin thetwo groups.23,24 Thissimilarimmuneresponsein these
circum-stancescouldbeattributedtosharedvirulencefactors,such asMproteinandstreptolysinO.GBSidentifiedinthisstudy alsocausedPTinchildren,althoughitinducedless aggres-siveimmuneandclinicalresponsesthanGASandGCS.
Funding
This study was supported by CNPq (Conselho Nacional de Desenvolvimento Cientifico e Tecnologico,Brasília, DF, Brazil) and FAPITEC (Fundac¸ão de Apoio à Pesquisa e à Inovac¸ãoTecnológicadeSergipe,Aracaju,SE,Brazil).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.EjzenbergB.Acondutafrenteaopacientecomfaringiteaguda. JPediatr.2005;81:1---2.
2.ChowdhuryPK,MazumderPK,KhanNM,DasRK.Anti-biogramin acutepharyngitis:astudyof137childrencases.DinajpurMed ColJ.2008;1:40---4.
3.BarbosaPJB,MullerRE,LatadoAL,AchuttiAC,RamosAIO, Wek-slerC,etal.Diretrizesbrasileirasparadiagnóstico,tratamento eprevenc¸ãodafebrereumáticadaSociedadeBrasileirade Car-diologia,daSociedadeBrasileiradePediatriaedaSociedade Brasileira de Reumatologia. Arq Bras Cardiol. 2009;93: 1---18.
4.SihTM,ChinskiA, EavyR,GodinhoR.VIManualde otorrino-laringologiapediátricadaIAPO.SãoPaulo:GráficaeEditoraRR DonneleyLtda;2007.
5.Teixeira LM. Características das bactérias que causam IRA nas crianc¸as: considerac¸ões atuais para seu diagnóstico. Sec¸ãoII:aspectosetiológicos.In:BenguiguiY,Antu˜nanoFJL, Schmunis G, Yunes J, editors. Infecc¸ões respiratórias nas crianc¸as. Washington: Organizac¸ão Pan-Americana de Saúde; 1999.
6.SimõesJA,FalcãoIM,DiasCM.Incidênciadeamigdaliteaguda napopulac¸ãosobobservac¸ãopelaRedeMédicos-Sentinelano anode1998.RevPortClinGeral.2002;18:99---108.
7.SitkiewiczI,HryniewiczW.Pyogenicstreptococci---dangerof re-emergingpathogens.PolJMicrobiol.2010;59:219---26. 8.Al-CharrakhA,Al-KhafajiJKT,Al-RubayeRHS.Prevalenceof
-hemolyticgroupsCandFstreptococciinpatientswithacute pharyngitis.NAmJMedSci.2011;3:129---36.
9.ZaoutisT,AttiaM,GrossR,KleinJ.TheroleofgroupCandgroup Gstreptococciinacutepharyngitisinchildren.ClinMicrobiol Infect.2004;10:37---40.
10.ShahM,CentorRM,JenningsM.Severeacutepharyngitiscaused bygroupCStreptococcus.JGenInternMed.2007;22:272---4. 11.Johnson DR, Kurlan R, Leckman J, Kaplan EL. The human
immuneresponsetostreptococcalextracellularantigens: clin-ical,diagnostic,andpotentialpathogeneticimplications.Clin InfectDis.2010;50:481---90.
12.KilianM. Streptococcus and enterococcus: pharyngitis; scar-letfever;skin andsoft tissueinfections; streptococcaltoxic shocksyndrome;pneumonia; meningitis;urinary tract infec-tions;rheumaticfever;post-streptococcalglomerulonephritis. In:GreenwoodD,SlackRCB,BarerMR,IrvingWL,editors. Medi-calmicrobiology:aguidetomicrobialinfections;pathogenesis, immunity,laboratorydiagnosis,andcontrol.18thed.London: ChurchillLivingstoneElsevier;2012.p.183---98.
13.ShulmanST,BisnoAL,CleggHW,GerberMA,KaplanEL,LeeG, etal.Clinicalpracticeguidelineforthediagnosisand manage-mentofgroupAstreptococcalpharyngitis:2012updatebythe InfectiousDiseasesSocietyofAmerica.IDSAGuidelineforGAS Pharyngitis.ClinInfectDis.2012;55:e86---102.
14.Levy CE. Manual de microbiologia clínica para o controle de infecc¸ão em servic¸os de saúde. Brasília: EditoraAgência NacionaldeVigilânciaSanitária;2004.
15.WangB,DileepanT,BriscoeS,HylandKA,KangJ,KhorutsA, etal.InductionofTGF-1andTGF-1-dependentpredominant Th17differentiationbygroupAstreptococcalinfection. Proc NatlAcadSciUSA.2010;107:5937---42.
16.Greghi SLA. Avaliac¸ão quantitativa das citocinas IL-4, IL-6, IL-8, IL-10 e do TGF-, presentes na saliva de pacientes com periodontite, antes eapós a submissãoà psicoterapia: análisecomparativa compacientes controles.Bauru: Univer-sidade de São Paulo, Faculdade de Odontologia de Bauru; 2012.
17.PackardRS,LibbyP,Review:.Inflammationinatherosclerosis: fromvascularbiologytobiomarkerdiscoveryandrisk predic-tion.ClinChem.2008;54:124---38.
19.Libby P, Okamoto Y, Rocha VZ, Folco EF. Inflammation in atherosclerosis: transition from theory to practice. Circ J. 2010;74:213---20.
20.HaidanA,TalaySR,RohdeM,SriprakashKS,CurrieBJ,Chhatwal GS.Pharyngealcarriageofgroup CandgroupGstreptococci andacuterheumaticfeverinanAboriginalpopulation.Lancet. 2000;356:1167---9.
21.PaulWE.Fundamentalimmunology.6thed.Philadelphia: Lip-pincottWilliams&Wilkins;2008.
22.Coelho-CastelloAAM, TromboneAPF,RochaCD,Lorenzi JCC. Resposta imune às doenc¸as infecciosas. Medicina (Ribeirão Preto).2009;42:127---42.
23.KonemanEW,AllenSD,JandaWM,SchreckenbergerPC,Winn WC.Diagnósticomicrobiológico.5thed.RiodeJaneiro:MEDSI EditoraMédicaeCientíficaLtda;2001.