REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Comparative
evaluation
of
propofol
in
nanoemulsion
with
solutol
and
soy
lecithin
for
general
anesthesia
José
Carlos
Rittes
a,
Guilherme
Cagno
a,
Marcelo
Vaz
Perez
a,b,
Ligia
Andrade
da
Silva
Telles
Mathias
a,b,∗aIrmandadedaSantaCasadeMisericórdiadeSãoPaulo,SãoPaulo,SP,Brazil
bFaculdadedeCiênciasMédicas,SantaCasadeMisericórdiadeSãoPaulo,SãoPaulo,SP,Brazil
Received28May2012;accepted20March2013 Availableonline17April2015
KEYWORDS Propofol/ pharmacology; Propofol/
pharmacokinetics; Emulsions; Nanostructures;
Generalanesthesia
Abstract
Introduction:Thevehicleforpropofolin1and2%solutionsissoybeanoilemulsion10%,which maycausepainoninjection,instabilityofthesolutionandbacterialcontamination. Formula-tionshavebeenproposedaimingtochangethevehicleandreducetheseadversereactions. Objectives: Tocomparetheincidenceofpaincausedbytheinjectionofpropofol,witha hypoth-esisofreductionassociatedwithnanoemulsionandtheoccurrenceoflocalandsystemicadverse effectswithbothformulations.
Method: AfterapprovalbytheCEP,patientsundergoinggynecologicalprocedureswereincluded inthisprospectivestudy:control(n=25)andnanoemulsion(n=25)groups.Heartrate, non-invasivebloodpressureandperipheraloxygensaturationweremonitored.Demographicsand physicalcondition wereanalyzed;surgicaltimeandtotal volumeused ofpropofol;local or systemicadverseeffects;changesinvariablesmonitored.Avalueofp<0.05wasconsidered significant.
Results:Therewasnodifferencebetweengroupsregardingdemographicdata,surgicaltimes, totalvolumeofpropofolused,armwithdrawal,painduringinjectionandvariablesmonitored. There was astatisticallysignificant differenceinpain intensityatthe timeofinduction of anesthesia,withlesspainintensityinthenanoemulsiongroup.
Conclusions: Bothlipidandnanoemulsionformulationsofpropofolelicitedpainonintravenous injection;however,thenanoemulsionsolutionelicitedalessintensepain.Lipidand nanoemul-sionpropofolformulationsshowedneitherhemodynamicchangesnoradverseeffectsofclinical relevance.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](L.A.S.T.Mathias).
http://dx.doi.org/10.1016/j.bjane.2013.03.026
PALAVRAS-CHAVE Propofol/
farmacologia; Propofol/ farmacocinética; Emulsões; Nanoestruturas;
Anestesiageral
Avaliac¸ãocomparativadopropofolemnanoemulsãocomsolutolecomlecitinade
sojaparaanestesiageral
Resumo
Introduc¸ão:Oveículodopropofolemsoluc¸õesa1e2%éaemulsãodeóleodesojaa10%,que podeprovocardoràinjec¸ão,instabilidadedasoluc¸ãoecontaminac¸ãobacteriana.Formulac¸ões forampropostascomoobjetivodealteraroveículoereduziressasreac¸õesadversas. Objetivos: Comparara incidênciade doràinjec¸ão dopropofolcom ahipótese dereduc¸ão associadaànanoemulsãoeaocorrênciadeefeitosadversoslocaisesistêmicoscomasduas formulac¸ões.
Método: Apósaprovac¸ãopeloConselho deÉtica em Pesquisa,foramincluídos nesteestudo prospectivopacientessubmetidas aprocedimentoscirúrgicosginecológicos: gruposcontrole (n=25)enanoemulsão(n=25).Forammonitoradosfrequênciacardíaca,pressãoarterialnão invasiva esaturac¸ãoperiférica deoxigênio. Foramanalisados dadosdemográficos eestado físico;tempocirúrgicoevolumetotalusadodepropofol;efeitosadversoslocaisousistêmicos; alterac¸õesnasvariáveisdemonitoramento.Considerou-sesignificativovalordep<0,05. Resultados: Nãohouvediferenc¸aentreosgrupos emrelac¸ãoa:dadosdemográficos,tempos cirúrgicos,volumetotalusadodepropofol,retiradadobrac¸o,presenc¸adedorduranteainjec¸ão evariáveisdemonitoramento.Verificou-sediferenc¸aestatísticasignificativanaintensidadeda dornomomentodainduc¸ãodaanestesia,commenorintensidadenogruponanoemulsão. Conclusões:Ambasasformulac¸õesdepropofol,lipídicaeemnanoemulsão,elicitaramdorà injec¸ãovenosa,porémasoluc¸ãodenanoemulsãopromoveudoremmenorintensidade.O propo-follipídicoeopropofolemnanoemulsãonãoapresentaramalterac¸õeshemodinâmicaseefeitos adversosderelevânciaclínica.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Aftermanyyearsofresearchfornewintravenousdrugsfor
useinanesthesia, thepharmaceuticalindustryhasseenin
propofol(ICI35868)apotentialanestheticagent.Duringthe
studypreclinicalphase,theformulationwithCremophorEL,
commonly used in the pharmaceuticalindustry, has been
proposed.1Duetothefrequentoccurrenceof
hypersensitiv-ityreactionsandinjectionpain,CremophorELformulation wasabandonedandthesearchforaviableformulationwas initiated with the use of lipidemulsions. Lipid emulsions determineanincreaseinonsettime,decreaseinpotency, andincreasein awakeningtimerelativetotheinitial for-mulationin CremophorEL.2 Inan attempttoimprovethe
limitations ofpropofol lipidemulsion, injectionpain,and potentialbacterial growth, formulations have been made withgreater concentrationof propofol;less than 10%oil; phospholipidsmodificationswithintheemulsion(containing differentfattyacids)andemulsiondropletswithproteins.3
Nanoemulsionshavebeenassociatedwithimprovement informulation stability, whichincreases theuseful life of propofol,reducestheamountoffreepropofolandtherefore maydecreasetheincidenceofinjectionpain,inadditionto awideantimicrobialspectrum.4,5
In search for nanoemulsions withmore safetyfeatures and lower risk of anaphylaxis, polyethylene glycol-660-hidroxiesterato (Solutol® HS15 --- BASF, Ludwigshafen,
Germany)wasdeveloped,awater-solublenonionic solubi-lizerfor parenteralusewithlipophilicdrugsandvitamins.
It contains about 70% of lipophilic molecules and 30% of hydrophilicmolecules,soitisstableandhasbeenusedin parenteralsolutions.6,7
Thus, taking into consideration that propofol is the intravenousanestheticmostcommonlyusedingeneral anes-thesiaworldwide,itsusestillhaslimitationsduetoadverse effects, and there are few studies comparing conven-tionalpropofolwithpropofolnanoemulsion.Weconducteda comparativeevaluationbetweenpropofolformulations tra-ditionallyused(soylecithinandnanoemulsionwithsolutol) ingynecologicalprocedures.Theobjectiveofthisstudywas tocomparetheincidenceofpropofolinjectionpain,witha hypothesisofreductionassociatedwithnanoemulsion,and theoccurrence oflocalandsystemicadverse effectswith bothformulations.
Methods
After approval by the institutional Research Ethics Com-mittee,aprospective,open,randomizedandcomparative studywasinitiated,whichincluded50patientsundergoing gynecological procedures in theDepartment of Obstetrics andGynecology.
The sample size calculation was based on a previous study,8 which reported incidence of pain in about 80% of
patients whoreceivedpropofolinlipidformulation.9,10 To
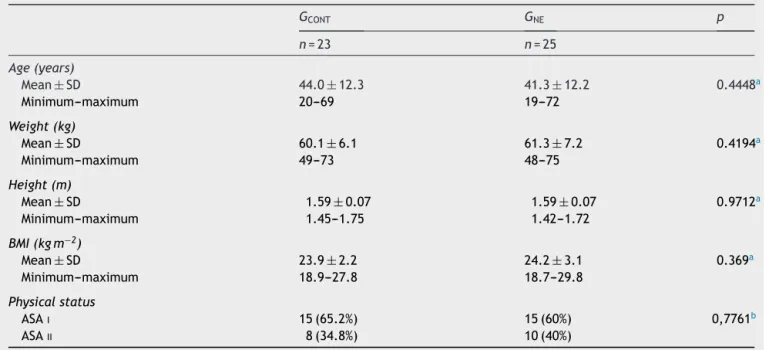
Table1 Studypopulationdemographicdata.
GCONT GNE p
n=23 n=25
Age(years)
Mean±SD 44.0±12.3 41.3±12.2 0.4448a
Minimum---maximum 20---69 19---72
Weight(kg)
Mean±SD 60.1±6.1 61.3±7.2 0.4194a
Minimum---maximum 49---73 48---75
Height(m)
Mean±SD 1.59±0.07 1.59±0.07 0.9712a
Minimum---maximum 1.45---1.75 1.42---1.72
BMI(kgm−2)
Mean±SD 23.9±2.2 24.2±3.1 0.369a
Minimum---maximum 18.9---27.8 18.7---29.8
Physicalstatus
ASAI 15(65.2%) 15(60%) 0,7761b
ASAII 8(34.8%) 10(40%)
GCONT,controlgroup;GNE,nanoemulsiongroup;BMI,bodymassindex;p,significanceofthestatisticaltestused. a Unpairedt-test.
b
2test.
powerof80%,andsignificancelevelof 5%.Itwasdecided touse50patientstocompensateforpossiblelosses.
Patients undergoing gynecological laparoscopic proce-dures and breast surgery, aged ≥18 years, ASA physical statusIandII(according totheAmericanSociety of Anes-thesiologistsclassification),BMI>18.5and<30.0kgm−2were
includedinthestudy.Exclusioncriteriawerepatientswith history of dyslipidemia and post-anesthesia nausea and vomiting,atopy,useofpsychoactivedrugs,andpregnancy.
Afterobtainingwritteninformedconsent,patientswere numberedanddistributed accordingtothe listofrandom numbers,at aratioof1:1,intotwogroups: controlgroup (Cont)with25patientswhoreceivedpropofolwithlecithin soy;nanoemulsiongroup(NE)with25patientswhoreceived propofolnanoemulsion.
Propofolconcentrationwas1%inboththeconventional soylecithinandnanoemulsion.
A blind study wasnotpossible becausethe drugs used inthestudyhaddifferentorganolepticproperties(propofol innanoemulsionistransparentandstableatroom tempera-ture,whilepropofolinsoybeanlecithinismilkyandrequires coldstorage).
Bothgroupsreceivedidenticalcareandattention,aswell asmonitoringandanesthetictechnique,exceptforthedrug used.Thepatientsreceivednopremedication.
Intheoperatingroom,venousaccesswasestablishedin preferred upper limb by a 20G Teflon device, and hydra-tionwasstartedwithlactatedRingersolution.Subsequently, patientsweremonitoredwithheartrate(HR), electrocar-diogram(ECG),noninvasivesystolicbloodpressure(SBP)and diastolicbloodpressure(DBP),peripheraloxygensaturation (SpO2),andbispectralindex(BIS).
Initial oxygenation was performed with 100% O2 via
face mask and at that time intravenous induction was initiated with sequential administration of the following
drugs:remifentanil,propofolorpropofolnanoemulsion,and atracurium.Thedosesusedforinductionofanesthesiawere lefttotheclinicalanesthesiologistdiscretion,without pro-tocol interference. The hemodynamic changes caused by formulations at doses commonly usedin clinical practice wererecorded.
Inductiontimewasconsideredfromtheendofdrug injec-tionuntilBISvaluesfallbelow60.
After tracheal intubation, patients were maintained on mechanical ventilation in semi-closed loop system, with 2Lmin−1 flow and ventilated with a mixture of
oxygen/nitrous oxide (50:50), with adjusted ventilatory parametersfromcurrent volume(CV)=8---10mLkg−1,
end-expiratory pressure of zero, and respiratory rate (RR) to maintain(PETCO2)between28and35mmHgwithSpO2above
95%.
Anesthesia wasmaintained withremifentanil,propofol orpropofol nanoemulsionmodified withan infusion pump speed,ifnecessary,tomaintainBISvaluesbetween40and 60.Aftertheendofanesthesia,thepatientsweretakento thepost-anesthesia care unitand dischargedto theward withAldrete-Kroulikmodifiedindex≥8.
Theanalyzedvariableswere:
- Age,weight,height,bodymassindex(BMI),andASA phys-icalstatus;
- Surgicaltimeandtotalvolumeusedofpropofoland propo-folnanoemulsion;
- Adverseeffectsattheinjectionsite:
• Injectionpain.
Twelvehoursafterthepuncture,thepatientwasasked ifshefeltpain duringinjection.Ifso, thedegree of pain wasevaluatedusingtheverbalscaleoffourterms(absent, mild,moderate,andsevere).
- Adverseeffects:
• Signsofinfectionatthepuncturesite;
• Nauseaandvomitingaftertheprocedure(assessedup todischargefrompost-anesthesiacareunit);
• Heartrate,systolicbloodpressure,diastolicblood pres-sure,andperipheraloxygensaturation(every10min); - Timeanddosesofinductionandmaintenance.
Statistical analysis wasperformed with the aid of the softwareSPSS(Statistical Packagefor Social Sciences) for Windows10.Student’st-testortheMann---Whitneytestwas used to compare quantitative variables between groups, accordingtosampledistribution.Ap-value<0.05was con-sideredstatisticallysignificant.
Results
Fromthe initial sample of 50 patients, 48 were included inthepresent study:23incontrolgroup(GCONT)and25in
nanoemulsiongroup(GNE).Twopatientswereexcludedfor
GCONTduetosurgicalcomplications.
Therewasnodifferencebetweengroupsregardingage, gender,weight,height,BMI,andASAvariables.Therewasno statisticallysignificantdifferencebetweengroups(p>0.05)
(Table 2). Surgical procedure times were similar in both
groups:3.02hforGCONTand2.50hforGNE(p=0.4893).
There was no significant difference between groups regarding arm withdrawal during the injection of propo-folandpresenceofpainduringinjection,buttherewasa statisticallysignificantdifferenceinpainseverity(p=0.01) (Table2).
The mean total volume used of propofol (GCONT) was
96.70±26.09mL and propofol nanoemulsion (GNE) was
82.93±37.77mL.Therewasnostatisticallysignificant dif-ferencebetweenthetwogroups(p=0.1521).
There was no significant difference in prevalence and severityofpainat theinjectionsite,assessed at12hours
Table2 Distributionofpatientsregardingarmwithdrawal duringpropofolinjection,presenceandseverityofpain dur-inginjection,assessedatthetimeofinductionofanesthesia.
GCONT GNE Test
Armwithdrawalduringinjection
No 17 73.9% 23 92% 2=2.82
Yes 6 26.1% 2 8% p=0.09
Painduringinjection
No 5 21.7% 12 48% 2=3.61
Yes 18 78.3% 13 52% p=0.07
Severityofpainduringinjection
Absent 5 21.7% 12 48% 2=6.56
Mild 6 26.1% 8 32% p=0.01
Moderate 7 30.4% 5 20%
Severe 5 21.7% 0 0%
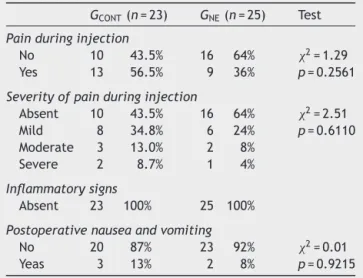
Table3 Evaluationofpainandotheradverseeventsinthe ward,12hafteranesthesia.
GCONT(n=23) GNE(n=25) Test
Painduringinjection
No 10 43.5% 16 64% 2=1.29
Yes 13 56.5% 9 36% p=0.2561
Severityofpainduringinjection
Absent 10 43.5% 16 64% 2=2.51
Mild 8 34.8% 6 24% p=0.6110
Moderate 3 13.0% 2 8%
Severe 2 8.7% 1 4%
Inflammatorysigns
Absent 23 100% 25 100%
Postoperativenauseaandvomiting
No 20 87% 23 92% 2=0.01
Yeas 3 13% 2 8% p=0.9215
aftervenipuncture,intheward(56.5%in GCONT and36.0%
in GNE). It was mild in both GCONT and GNE, 34% and
24.0%,respectively.Nopatientshowedsignsofinflammation
(Table3).
Fivepatients (3 in GCONT and 2 in GNE) had
postopera-tive nauseaand vomiting(2 --- p=0.9215) (Table3). Five patients(2inGCONTand3inGNE)hadsystemicadverseevents
(2---p=0.9215):twopatientsineachgrouphadmildskin rash and one patientin GNE had moderate bronchospasm
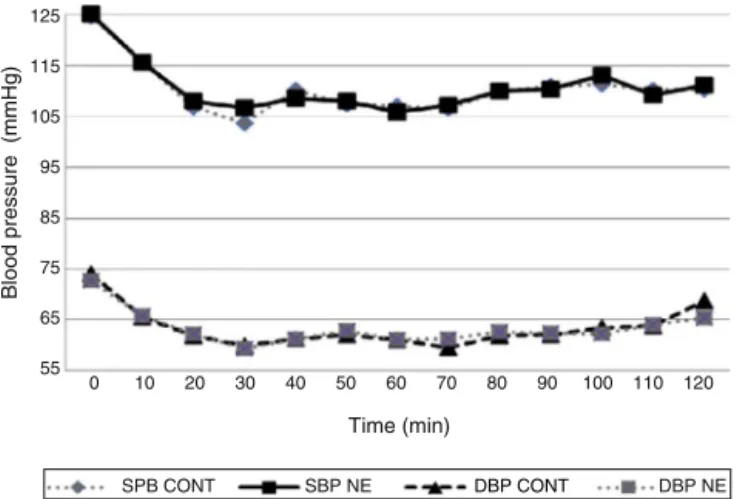
andwheezing.Therewasnosignificantdifferencebetween groupsregardingHR,SBP,DBP,andSpO2atallassessedtimes
(unpairedt-test---p>0.05)(Figs.1and2).
Discussion
Although the success of propofolis indisputable, an ideal formulationwhicheliminatestheadversereactionsresulting fromlipidformulationsisinvestigateduntilthepresentday. Therearefewstudiescomparingthepropofolnanoemulsion andclassicallipidformulations,7,8whichledtothepresent
studyinwhich48patientsundergoinggynecological proce-dures wereevaluatedin ordertoidentify specificclinical features, suchas propofolinjection painand presence of
Time (min)
Heart rate
60
0 10 20 30 40 50 60 70 80 90 100 110 120 65
70 75 80 85
HR CONT HR NE
Time (min)
Blood pressure (mmHg)
0 10 20 30 40 50 60 70 80 90 100 110 120 55
65 75 85 95 105 115 125
SPB CONT SBP NE DBP CONT DBP NE
Figure 2 Systolic anddiastolic bloodpressure evolution in bothgroups.
localandsystemicadverseevents associatedwiththeuse ofpropofolnanoemulsion.Theywerecomparedwiththose relatedtotheadministrationofpropofolinlipidemulsion (conventionalpropofol).
Although severalpreparations ofpropofolweretested, a preparation that reduces the incidence of pain after injection has not been found yet. Because it belongs to a group of phenols with chemical stability and low tox-icity, but with the potential to cause skin, endothelium, and mucous membranes irritation, it is expectedbut not desiredthatpropofolinjectioncausespain.Inthisstudy,the incidenceofpropofolinjectionpainassessedat the injec-tion timewas lower in nanoemulsion group (GNE) than in
control group, without statistical significance (GNE=56.0%
versusGCONT=78.3%).Regardingarmwithdrawalfrequency
during propofol injection, there was nostatistical differ-ence(GNE=8.0% versus GCONT=26.1%). Regarding injection
painseverity,mild,moderate,andseverepainweremore frequentin GCONT,p=0.01.However,inboth assessments,
painincidence andarm withdrawal frequency at propofol injection time, the differences were clinically significant and p-values (0.07 and 0.09) suggest that, if the sam-ple were larger, statistical difference would have been found.
In the same study, the incidence of propofol injection painassessed12hafterpuncturewaslowerinnanoemulsion groupthaninthecontrolgroup,without statistical signifi-cance(GNE=36.0%versusGCONT=56.5%),aswellasinjection
painseverity.
Onlytwostudies werefoundinthe literaturethatalso compared the classical soy lecithin versus nanoemulsion formulationsof propofolusedinthisstudy.7,8 Sudoetal.7
evaluatedtheincidenceofpaininmicereceiving intraperi-tonealinfusionof aceticacidandlipidvehicleofpropofol andnon-lipidnanoemulsion(sameasthatusedinthisstudy). Aceticacidandlipidvehicleofpropofolcausedpainafter intraperitonealinjection.However,therewasnopainafter theadministrationof propofolnanoemulsion.Inthestudy byRodriguesetal.8,withpatientsundergoingsedationfor
endoscopy, theincidence of propofolnanoemulsion injec-tionpain(sameformulationusedinthisresearch)waslower thanwiththeuseofconventionalpropofol,withstatistical significance(53.3%vs.82.7%).
Other studies with different formulations showed dif-ferent results, such as the research that found higher incidenceofpainwiththenon-lipidformulationofpropofol (Cleofol®;ThemisMedicare,India)thanwithpropofol
emul-sionwithmedium chain triglycerides(Propofol-Lipuro®, B
Braun, Germany).9 It is worth mentioning that the lipid
emulsion propofol used in this study was different from that used in the cited publication. Previous studies have found that formulations with medium chain triglycerides have lower freefraction of propofol and hence tendency toalowerincidenceofpain.10---14
Sim et al.,15 in a study that comparatively assessed
the level of plasma bradykinin after intravenous injec-tion of 0.9% saline solution, lipid emulsion propofol, propofol microemulsion, and polyethylene glycol-660-hidroxiestearato(Solutol®HS15),showedhigherlevelswith
theinjection of microemulsionand solutol not related to increasedincidenceofpain.Thus,theauthorsproposethat the onset of pain after propofol injection is not entirely relatedtothebradykininrelease.
The application of lidocaine, strategy widely used to reducepain oninjectionof propofol,has been discussed. Sim et al.15 reported that there was no change in free
propofolconcentrationduringtheaqueousphaseafter lido-caineaddition;whileYamakageetal.14reportedthatthere
wasachange of pH andstability ofthe solutionwiththe lidocaineaddition,suggesting that lidocaineadministered before propofol may inhibit transmission of pain through endothelialfreenerveendings.
Althoughtheassessmentof surgicaltimeandtotal vol-umeusedofpropofolhas notbeen partof theobjectives ofthisstudy,thesedatawereanalyzedandarepartofthe resultsbecausestatisticallysignificantdifferencesinanyof themorbothcouldcreateabiasininterpretingtheresults ofadverseevents.
Therewerenosignsofinflammationattheinjectionsite inanypatient,whichmayoccurin1---5%ofthecases.16
Ithasbeenwidelyreportedintheliteraturethat intra-venous administrationof propofolmay lead to decreased blood pressure with little change in heart rate and rhythm,17---21whichisconfirmedinthisstudythatfound
sim-ilarreductionofSBPandDBPvaluesinbothgroupsonlyat inductiontime,withposteriorstability,withminimum toler-ablevalues.Rodriguesetal.,8inhumans,andSudoetal.7in
mice,bothusedlipidornanoemulsionpropofolandreported reductionin systolicand diastolicarterial pressures, with no difference between the analyzed groups. Heart rate also decreased at the time of induction in both groups, with subsequent stabilization, without reaching critical levels.
Inthepresentstudy,fewcasesofnausea/vomitingwere observed after surgery (GNE=8.0% versus GCONT=13.0%),
with no statistical difference between the drugs used, which confirms the literature reporting that propofol has antiemetic property, by antidopaminergic activity, with depressant effectonthe chemoreceptortrigger zone and vagalnuclei, lower releaseof glutamate andaspartate in theolfactory cortex, anddecreased serotoninin thearea postrema.22
emulsion and propofol in nanoemulsion showed no hemodynamic changes and adverse effects of clinical relevance.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
The drugsused inthis study (propofolin soybeanlecithin andpropofolnanoemulsion)weredonatedbytheCristália®
ProdutosQuímicoseFarmacêuticos(Itapira,SP,Brazil).
References
1.GlenJB,DaviesGE,ThomsonDS,etal.Ananimalmodelforthe investigationofadverseresponsestoi.v.anestheticagentsand theirsolvents.BrJAnaesth.1979;51:819---27.
2.BakerMT,NaguibM.Propofol:thechallengesofformulation. Anesthesiology.2005;103:860---76.
3.ThompsonKA,GoodaleDB.Therecentdevelopmentofpropofol (Diprivan).IntensiveCareMed.2000;26Suppl.4:S400---4. 4.DateAA,NagarsenkerMS.Designandevaluationof
microemul-sions for improved parenteral delivery of propofol. AAPS PharmSciTech.2008;9:138---45.
5.SneydJR,Rigby-JonesAE.Newdrugsandtechnologies, intra-venous anaesthesia is on the move (again). Br J Anaesth. 2010;105:246---54.
6.Morey TE, Modell JH, ShekhawatD, et al. Anesthetic prop-erties of a propofol microemulsion in dogs. Anesth Analg. 2006;103:882---7.
7.SudoRT,BonfáL,TrachezMM,etal.Caracterizac¸ãoanestésica dananoemulsãonãolipídicadepropofol.RevBrasAnestesiol. 2010;60:475---83.
8.Rodrigues TA, AlexandrinoRA, KanczukME, et al. Avaliac¸ão comparativaentrepropofolcom doisveículosdiferentes:em nanoemulsãocomsolutolecomlecitinadesojaempacientes submetidosaprocedimentosendoscópicos.RevBrasAnestesiol. 2012;62:324---33.
9.DubeyPK, Kumar A. Pain on injectionof lipid-free propofol and propofolemulsioncontainingmedium-chain triglyceride: acomparativestudy.AnesthAnalg.2005;101:1060---2. 10.LarsenB,BeerhalterU,BiedlerA,etal.Lesspainoninjection
byanewformulationofpropofol?Acomparisonwithpropofol LCT.Anaesthesist.2001;50:842---5.
11.LarsenR,BeerhalterU,ErdkönigR,etal.Injectionpainfrom propofol-MCT-LCTinchildren.Acomparisonwithpropofol-LCT. Anaesthesist.2001;50:676---8.
12.RauJ,RoizenMF,DoenickeAW,etal.Propofolinanemulsion oflong-and medium-chaintriglycerides:theeffecton pain. AnesthAnalg.2001;93:382---4.
13.SunNC,WongAY,IrwinMG.Acomparisonofpainonintravenous injectionbetweentwopreparationsofpropofol.AnesthAnalg. 2005;101:675---8.
14.YamakageM,IwasakiS,SatohJ,etal.Changesinconcentrations offreepropofolbymodificationofthesolution.AnesthAnalg. 2005;101:385---8.
15.SimJY,LeeSH,ParkDY,etal.Painoninjectionwith microemul-sionpropofol.BrJClinPharmacol.2009;67:316---25.
16.PederneirasSG,DuarteDF,TeixeiraFilhoN,etal.Usodo propo-folemanestesiasdecurtadurac¸ão:estudocomparativocomo tiopental.RevBrasAnestesiol.1992;42:181---4.
17.Claeys MA, Gepts E, Camus F. Haemodynamic changes dur-inganaesthesia induced and maintained with propofol.Br J Anaesth.1983;60:3---9.
18.Grounds RM, Twigley AJ, Carli F, et al. The haemodynamic effectsofintravenousinduction.Comparisonoftheeffectsof thiopentoneandpropofol.Anaesthesia.1985;40:735---40. 19.Hug CC, McLeskey CH, Nahrwold NL, et al. Hemodynamic
effectsofpropofol---datafrom24,771patients.AnesthAnalg. 1993;76:S154.
20.El-BeheiryH,KimJ,MilneB,etal.Prophylaxisagainstthe sys-temichypotensioninducedbypropofolduringrapid-sequence intubation.CanJAnaesth.1995;42:875---8.
21.SatoM,TanakaM,UmeharaS,etal.Baroreflexcontrolofheart rateduringandafterpropofolinfusioninhumans.BrJAnaesth. 2005;94:577---81.