REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Use
of
remifentanil
to
reduce
propofol
injection
pain
and
the
required
propofol
dose
in
upper
digestive
tract
endoscopy
diagnostic
tests
Gustavo
Nadal
Uliana
a,b,e,∗,
Elizabeth
Milla
Tambara
c,d,e,
Giorgio
Alfredo
Pedroso
Baretta
eaGraduatePrograminSurgery,UniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil bDepartmentofAnesthesiology,HospitaisVita,Curitiba,PR,Brazil
cDisciplineofAnesthesiology,EscoladeMedicina,PontifíciaUniversidadeCatólicadoParaná(PUC-PR),Curitiba,PR,Brazil dDepartmentofAnesthesiology,HospitalSantaCasadeCuritiba,Curitiba,PR,Brazil
eSurgery,UniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil
Received24November2014;accepted23December2014 Availableonline9October2015
KEYWORDS
Sedation;
UpperGIdiagnostic test;
Propofol; Remifentanil
Abstract
Backgroundandobjectives: Theintroductionofpropofol(2,6-diisopropylphenol)asasedative agenthastransformedtheareaofsedationforendoscopicprocedures.However,amajor draw-backofsedationwiththeuseofpropofolisitshighincidenceofinjectionpain.Themostwidely usedtechniqueinreducingpropofolinjectionpainisthroughtheassociationofotherdrugs. Theaimofthisstudywastoevaluatetheeffectofremifentanil-propofolcombinationonthe incidenceofpropofolinjectionpainanditsinfluenceonthetotaldoseofpropofolrequiredfor sedationinupperdigestivetractendoscopy(UDE)diagnostictests.
Method: Onehundredandfivepatientsundergoingupperdigestivetractendoscopywere eval-uatedandrandomly dividedinto3groups of35patients each. The ControlGroupreceived propofol alone;Study-group1 receivedremifentanilatafixeddoseof0.2mg/kg combined withpropofol;Study-group2receivedremifentanilatafixeddoseof0.3mg/kgcombinedwith propofol.Theincidenceofpropofolinjectionpainandthetotaldoseofpropofolrequiredfor thetestwereevaluated.Thesamplewasverysimilarregardingage,weight,height,sex,and physicalstatus.Statisticalanalysiswas performedaccordingtothenature oftheevaluated data.Student’st-testwasusedtocomparethemeanofage,weight,height(cm),anddose (mg/kg)variablesbetweengroups.The2testwasusedtocomparesex,physicalstatus,and
propofolinjectionpainbetweengroups.Thesignificancelevelwas˛<0.05.
Results:Therewassignificantstatisticaldifferencebetweenthestudygroupsandthecontrol groupregardingtheparametersofpropofolinjectionpainandtotaldoseofpropofol(mg/kg)
∗Correspondingauthor.
E-mails:[email protected],[email protected](G.N.Uliana). http://dx.doi.org/10.1016/j.bjane.2014.12.001
used.However,therewerenostatisticaldifferencesbetweenthetwostudygroupsforthese parameters.
Conclusion:Weconcludethattheuseofremifentanilatdosesof0.2mg/kgand0.3mg/kgwas effectiveforreducingboththepropofolinjectionpainandthetotaldoseofpropofolused. ©2015SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.Allrights reserved.
PALAVRAS-CHAVE
Sedac¸ão;
Endoscopiadigestória altadiagnóstica; Propofol; Remifentanil
Usodoremifentanilparareduc¸ãodadoràinjec¸ãodepropofoleadosenecessáriade propofolemexamesdeendoscopiadigestóriaaltadiagnóstica
Resumo
Justificativaeobjetivos: Aintroduc¸ãodopropofol(2,6-di-isopropilfenol)comoagentesedativo temtransformadoaáreadasedac¸ãoparaprocedimentosendoscópicos.Entretanto,umgrande inconvenientedasedac¸ãocomousodopropofolésuaaltaincidênciadedoràinjec¸ão.Atécnica maisusadanareduc¸ãodadoràinjec¸ãodopropofoltemsidoaassociac¸ãocomoutrosfármacos. Oobjetivodesteestudofoiavaliararepercussãodaassociac¸ãodoremifentanilcomopropofol naincidênciadedoràinjec¸ãodepropofoleainfluêncianadosetotaldepropofolnecessária parasedac¸ãoemendoscopiadigestóriaalta(EDA)diagnóstica.
Método: Foramavaliados105pacientes,submetidosàEDAdiagnósticaedivididos aleatoria-menteemtrêsgruposde35.OGrupoControlefoisedadoapenascompropofol.OGrupode Estudo1foisedadocomremifentanilemdosefixa de0,2g/kgassociadoao propofol.Eo
GrupodeEstudo2foisedadocomremifentanilemdosefixade0,3g/kgassociadoao
propo-fol.Foramavaliadasaincidênciadedoràinjec¸ãodepropofoleadosedepropofolnecessária para oexame. A amostrasemostrou bastante similar em relac¸ãoàsvariáveis idade,peso, altura,sexoeestadofísico.Deacordocomanaturezadosdadosestudados,procedeu-seao tratamentoestatísticojulgadoadequado.Usou-seotestetparacomparac¸ão,entreosgrupos analisados,dasmédiasdasvariáveisidade,peso,altura(cm)edose(mg/kg).Foiusadooteste
2paracomparac¸ão,entreosgruposanalisados,dasvariáveissexo,estadofísicoedoràinjec¸ão
depropofol.Oníveldesignificânciaadotadofoi␣<0,05.
Resultado:Houvediferenc¸aestatísticasignificativaentreosgruposdeestudoeogrupocontrole tanto noparâmetrodoràinjec¸ãodepropofolquanto noparâmetrodosedepropofol usada (mg/kg). Entretanto,não houvediferenc¸asestatísticas entreosdoisgrupos deestudo para essesparâmetros.
Conclusão:Ousodoremifentanilnasdosesde0,2g/kgede0,3g/kgmostrou-seefetivo
tantosobreoparâmetroreduc¸ãodadoràinjec¸ãodepropofolquantosobreoparâmetrodose depropofolusada.
©2015SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Inmanycountries,sedationhasbecomeroutineinpatients undergoingcolonoscopyanddiagnosticupperdigestivetract endoscopy(UDE).1AccordingtoasurveyfromtheAmerican
CollegeofGastroenterologists,sedationisusedinover98% ofcolonoscopyexamsandUEintheUnitedStates.2Theterm
sedationisusedfordepressionofanindividual’slevelof con-sciousness.Sedationisusedtopromoteanxiolysis,amnesia, and,insomeinstances,analgesia.3
The introduction ofpropofol (2,6-diisopropylphenol) as a sedative agent has transformed the area of sedation for endoscopic procedures.3 Much of propofol’s
popular-ity between physicians and patients is related to its
pharmacokinetic and pharmacodynamic properties, which givesthedrugaquickstartandendofitseffectsand pro-videsthepatientasenseofwell-being.3Inmanyrespects,
propofol is an ideal agent for short procedures in outpa-tients.However,becauseofitspharmacologicalprofile,one ofitsrecommendationsis tobeusedonlybyprofessionals trainedintheadministrationofgeneralanesthesia.4Amajor
drawbackofsedationusingpropofolisitshighincidenceof injection pain.5,6 The presence of propofolinjection pain
rangesfrom28%7to90%8ofcases.
Macarioetal.9questionedamongAmerican
among 33 clinical outcomes, when taking into account frequency and clinical significance together. Many stud-ies have been conducted seeking to minimize or resolve this problem.10 Even after changing the original
formula-tionofpropofol,thecremophorthinner,whichwaslinked to anaphylactic reaction,11 to a lipid emulsion, the pain
remained.Thisshowsthatitisduetothedrugitself,notthe formulac¸ão.12 Thatis tosaythattheuseoflipidemulsion
almostabolishedthepainassociatedwithdiazepamand eto-midate injection.13---15 Optional propofolformulations with
changes in the composition of the lipid emulsion, differ-entfractionsofmedium-andlong-chaintriglycerides,and use of different preservatives, such as ethylenediamine-tetraacetic acid(EDTA) andsodiummetabisulfite, did not eliminate the injection pain.16 However, it has been
sug-gestedthatincreasedlipidsolventcontentmayreducethe concentration of free propofol in the aqueous phase and its contact with free nerve endings, which could reduce propofolinjectionpainduring.17---22 Recommendationssuch
as using large-caliber veins help reduce propofol injec-tion pain. However, the most widely used technique to reduce propofol injection pain has been the combination ofother drugs suchaslidocaine,23---25 ephedrine,24
magne-siumsulfate,26thiopental,25ketamine,27 acetaminophen,28
andtramadol,29 amongothers.
Opioids arethedrugsmostcommonlyusedin combina-tionwithpropofolfor anesthesia. Itsuse inthe reduction ofpropofolinjectionpainiswidespreadandhasprovedto be effective in most clinical studies,30,31 although it was
provedineffectiveinthestudybyBasaranogluetal.32 Itis
knownthatintravenousanesthetics,suchashypnotics, opi-oids, andbenzodiazepines, combine synergistically during anesthesia.33 Thesedrugsareassociatedinorderto
poten-tiatethe effectsof the interactionbetweenpropofol and opioids34; thus, the desired effects can beachieved with
lowerdosesofdrugs.Inveryshortoutpatientprocedures, suchasendoscopicexaminationsorlumbarpuncturein pedi-atricpatients,35theassociationofremifentanilandpropofol
enablesextremelyfastrecoverywithshortduration pharma-codynamiceffects.
The aim of this study was to evaluate the effects of remifentanil associated withpropofol in the incidenceof propofolinjectionpainand,concomitantly,theinfluenceof theremifentanilassociation onpropofoldose requiredfor sedationindiagnosticUDE.
Method
The study wasconducted after approval by the Research EthicsCommitteeoftheinstitution,andallpatients were informedabout the projectand signed theinformed con-sent.
A total of 105 patients of both genders, physical sta-tus ASA I or II, undergoing diagnostic UDE was selected. Exclusion criteria were patients aged under 18 and over 65,pregnantwomenwithahistoryof allergytoany com-ponent of the study drugs, in whom it was necessary, in addition to the diagnostic test, any kind of therapy dur-ing the procedure, and any patient with physical status ASA>II.
Thepatientswererandomlydividedintothreegroupsby drawinglots:
Control Group (n=35), received sedation with propofol alonefordiagnosticUDE.
Study Group 1 (n=35), received sedation with remifen-tanil at fixed dose of 0.2g/kg combined withpropofol
fordiagnosticUDE.
StudyGroup2(n=35),receivesedationwithremifentanil atfixeddoseof0.3g/kgcombinedwithpropofolfor
diag-nosticUDE.
Patientswhomettheinclusioncriteriaweremonitored with cardioscopy, pulse oximetry, and noninvasive blood pressure,usingthemultiparameterPhilipsC3Monitor,type glasses nasal catheter placement with O2 flow (3L/min)
andperipheral22Gvenouspuncturecatheterinantecubital regionfor 0.9% isotonicsalineandsedativesinfusion. The patientswerethenplacedintheleftlateralpositionforthe exam.
Using a syringe, 10mL isotonic 0.9% saline at a rate of1mLevery 3s wasadministered tothe Control Group; remifentanil0.2g/kgtotheStudyGroup 1;and
remifen-tanil0.3g/kgtotheStudyGroup2.Subsequently,propofol
wasadministered usinga 20mLsyringe at a rate of 1mL every3s.Duringpropofolinjection,thepatientwasasked if he felt any pain in the arm with the catheter and if it was located at the injection site. All patients were askedidentically.Propofolwasinjectedtolossof conscious-ness,checkedbythelackofresponsetoverbalstimulation and loss of ciliary reflex and confirmed by all team members. All examinations were performed by the same endoscopist, and the time of the patient’s recovery was verifiedby spontaneouseye openingin responsetoverbal stimulation.
Dataonage,weight,sex, height,physicalstatus, pres-ence or absence of propofol injection pain and propofol doseat mg/kgwererecordedinspecific worksheetatthe proposedtimepoints.
Accordingtothenatureofthedatastudied,the appro-priate statistical analysis was performed. We used the t
testtocomparebetweengroupsthemeanofthevariables age, weight,height (cm), and dose (mg/kg). The 2 test
wasusedtocomparegender,physicalstatus,andpropofol injectionpainbetween groups. Thesignificance level was
˛<0.05.
Results
Thegroupswerehomogeneouswithrespecttoage,weight, height,sex, andphysical status.Adescriptivesummaryof eachgroupisshowninTables1---3.
TheincidenceofpropofolinjectionpaininControlGroup waspresent in 40% of patients and significantly lower in thestudygroupspre-medicatedwithdosesofremifentanil 0.2g/kg (14.28%) and remifentanil 0.3g/kg (14.28%).
There was no statistical difference between the Study Groups1andStudyGroup2regardingtheincidencepropofol injectionpain(Table4andFigs.1---3).
Table1 Comparisonofmeanage,weight,andheight(cm) intheanalyzedgroups:ttest.
Groups n Idade p
Min---max Mean±SD
Study1 35 18---60 36.17±11.73 0.34 Study2 35 20---52 33.89±7.99
Study1 35 18---60 36.17±11.73 0.43 Control 35 20---60 34.14±9.28
Study2 35 20---52 33.89±7.99 0.90 Control 35 20---60 34.14±9.28
Groups n Weight p
Min---max Mean±±SD
Study1 35 48---98 69.20±13.19 0.77 Study2 35 50---94 70.09±11.87
Study1 35 48---98 69.20±13.19 0.12 Control 35 50---110 74.00±12.18
Study2 35 50---94 70.09±11.87 0.18 Control 35 50---110 74.00±12.18
Groups n Height(cm) p
Min---max Mean±SD
Study1 35 150---180 165.77±7.01 0.75 Study2 35 150---182 166.34±7.88
Study1 35 150---180 165.77±7.01 0.34 Control 35 155---184 167.57±8.51
Study2 35 150---182 166.34±7.88 0.53 Control 35 155---184 167.57±8.51
n,numberofpatients;min---max,minimumandmaximum val-ues;SD,standarddeviation;p,p-valueprobability.
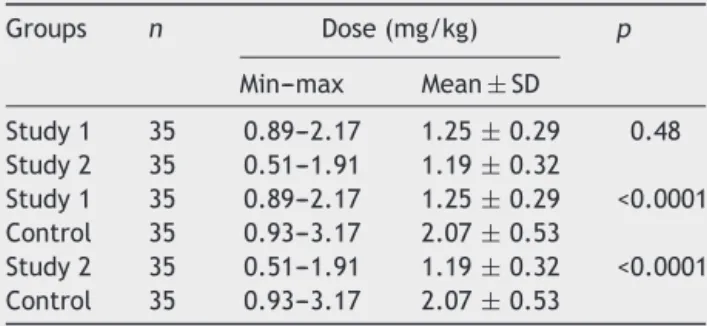
significantlyhigherthanthatrequiredinthestudygroups.
The mean dose of propofol in the premedicated group
withremifentanil0.2g/kg was1.25mg/kg, witha range
from0.89to 2.17mg/kg. Andthe average dose of propo-folinthegrouppremedicatedwithremifentanil0.3g/kg
was1.19mg/kg, with a range of 0.51---1.91mg/kg. There wasno statistical difference in the mean mg/kg dose of propofolusedbetweenthetwostudy groups (Table5and
Fig.4).
Table2 Comparisonofsexintheanalyzedgroups:2test.
Groups Sex Total p
Male Female
Study1 10 25 35 0.78 Study2 8 27 35
Study1 10 25 35 0.61 Control 13 22 35
Study2 8 27 35 0.30 Control 13 22 35
p,p-valueprobability.
Table 3 Comparison of physical status in the analyzed groups:2test.
Groups ASA Total p
1 2
Study1 29 6 35 0.26 Study2 24 11 35
Study1 29 6 35 1.0 Control 30 5 35
Study2 24 11 35 0.15 Control 30 5 35
p,p-valueprobability.
Table4 Comparisonofpropofolinjectionpaininthe ana-lyzedgroups:2test.
Groups Propofolinjectionpain Total p
Yes No
Study1 5 30 35 0.73 Study2 5 30 35
Study1 5 30 35 0.03 Control 14 21 35
Study2 5 30 35 0.03 Control 14 21 35
p,p-valueprobability.
Discussion
Fordiagnostic UDE, the idealcharacteristics of the drugs wouldbeaquickconnectionwiththeeffectsite,reduced accumulation in the body, and rapid elimination, which
would promote rapid pharmacodynamic effects, such as
early hypnosis, deepsedation, rapid andefficient control useofautonomicresponses,andearlyawakening.
Anestheticswiththesecharacteristicshaveahigher pre-dictability of itspharmacodynamic effects, which gives a
Control
Yes
No
Study 1
Yes
No
Figure 2 Frequency of propofol injection pain in Study Group1.
Study 2
Yes
No
Figure 3 Frequency of propofol injection pain in Study Group2.
greatersafetymargintotheanesthesiologistandprevents, for example, a prolonged awakening or late respiratory depression.
Propofol is a safe and effective drug for gastrointesti-nal endoscopic procedures and is associated withshorter recoveryperiodandearlierhospitaldischarge,higherscores
Table5 Comparisonofmeandose(mg/kg)intheanalyzed groups:ttest.
Groups n Dose(mg/kg) p
Min---max Mean±SD
Study1 35 0.89---2.17 1.25±0.29 0.48 Study2 35 0.51---1.91 1.19±0.32
Study1 35 0.89---2.17 1.25±0.29 <0.0001 Control 35 0.93---3.17 2.07±0.53
Study2 35 0.51---1.91 1.19±0.32 <0.0001 Control 35 0.93---3.17 2.07±0.53
n,numberofpatients;min---max,minimumandmaximum val-ues;SD,standarddeviation;p,p-valueprobability.
0 0.5 1 1.5 2 2.5
Control
0 0.2 0.4 0.6 0.8 1 1.2
Propofol dose (mg/kg) Study 1 Study 2
Figure4 ComparisonofpropofoldoseusedinControlGroup andStudyGroups.
ofpost-anestheticrecovery,bettersedationandincreased patientcomplianceregardingtraditionalsedation,withouta increaseincardiopulmonarycomplications.36However,itis
adrugthathasahighrateofinjectionpain,especiallywith smallercaliberveins,suchasthebackofhands.37Toreduce
propofol injection pain, puncture of larger caliber veins, suchastheantecubitalregion,shouldberecommendedfor inductionandmaintenanceofanesthesiatechniquesbased ontheuseofthisdrug.
Inourstudy,it wasshown thatevenwiththepuncture oflargercaliberveins,theincidenceofpropofolinjection painstillremainedveryhigh,around40%.
Although the pain etiology is not exactly established, differentmethods anddifferent drugs have been used to reduce its incidence and severity.24 The combination of
drugs with the aim to reduce propofol injection pain is aneffectiveandtechnicallyeasymethodandindependent ofthepuncturedveinlocation.Mostdrugsassociatedwith propofoltoreduce injectionpainorwasnotstudiedordo notsignificantlyreducethepropofoldoserequiredfor induc-tionofanesthesia.29,38Insomestudies,theuseoflidocaine
combinedwithpropofoldecreasedtheanestheticpotency ofpropofol.39,40
Opioids aredrugs usedinassociation withpropofol for generalanesthesiaand sedation. An importantreason for thischoice inthe present study isthat opioidsare syner-gistically combined with propofol and effectively reduce itstotal dose during anesthesia. Fentanyl and alfentanil, althoughwidelyusedinanesthesia,havethedisadvantage ofextending itsclinical tothe postoperativeperiod, par-ticularlyin shortprocedures. A reasonable goal wouldbe toreduce propofol injectionpainwithout theappearance of other adverse effects, such as delayed recovery from anesthesia.
doseofemifentanilwithoutaninfusionissuitableonlyfor clinicalproceduresthatrequireintenseanalgesia,suchas in diagnostic and therapeutic procedures performed out-sidetheoperatingroomandlastingonly afewminutes.41
Itrequireslesspreparationtimeofanesthesia,hasalower costbecauseit does notrequire infusion pumpsand spe-cificinfusers.In2004,Eganetal.usedremifentanilatdose bolusofupto200g,whichshowedmoresignificant
venti-latoryeffectsintheelderlythaninyoungpatients.41These
effectswereshort-livedandeasilymanagedonlywithverbal stimulationandoxygenaddition(2L/min).Theinteraction model andventilatory involvement proposed by LaPierre etal.42 in2012,suggeststheoccurrenceofgreaterairway
obstructionwithhigherconcentrations of propofolandan intolerableventilatorydepressionwithhighconcentrations ofremifentanil.Thesameauthoralsoproposesasignificant synergism between both drugs. This indicates that lower dosesofeacharerequiredtoachievethesameeffect.The resultsfoundbyHayesetal.,in2008,indicatethatinthe propofol-remifentanilcombination, the option of increas-ing the remifentanil dose (1.5g/kg) and decreasing the
propofol dose (2mg/kg) increased the duration of apnea andreducedtherecoverytime;withreducedremifentanil dose (0.5g/kg) and increased propofol dose (4mg/kg),
the time of apnea was reduced and the recovery period increased.35
Theuseofpre-injectionbolusdosesofremifentanil(0.2 and0.3g/kg)consideredlowcomparedtodosespreviously
studied30,32,35,41 is justifiedbecause it is a diagnostic test
ofshortduration,inwhich thereisarestrictionregarding airwaymanagement,withthegreateststimulusduringthe device introduction, the peak time of the opioid effect that,accordingtoEganetal.,2004,occurred2.5minafter injection.41 The option for a lower dose of remifentanil
wassimilartothat suggested by Droveret al.,43 in 2004,
becauseintheirstudyduringesophagogastroduodenoscopy in children, lower doses minimized episodes of oxygen desaturation.Increasingthedose ofremifentanildoesnot diminishtheneedforpropofolandincreasestheriskofside effectsrelated toopioid.Jeong etal.,44 in 2011,showed
thata dose of0.3g/kg waseffectivein reducing
propo-fol injection pain even with the use of the dorsal hand veinswhenmixedwithlidocaine;however,dosesof0.5and 1.0g/kgweremoreeffective.
Becausebothdrugsarepotentdepressantofventilation and based on the principle of an asymmetric interaction curve between the drugs, as the one proposed by Fidler et al.,45 in 2006, and on the results previously found by
Hayesetal.,35 in 2008,we decidedin thisstudy tousea
lowdoseof remifentanilandassessthepharmacodynamic interactionwithpropofolduringendoscopicexaminations. Anotherreasonforchoosingthesedosesisduetothefact thatlargeveinsoftheantecubitalregionwerechosen for venousaccess,whichwouldbeareductionfactorofpropofol injectionpain.
In our study, as in many others,46---50 it is shown that
remifentaniliseffectiveinreducingpropofolinjectionpain; however,ourstudyalsoquantifiestheeffectof twodoses ofremifentaniloverthepropofoldoserequiredtoachieve apharmacodynamiceffectduringtheproposedprocedure. Atdosesof0.2and0.3g/kg,remifentanildidnotcause
sedativeeffectthatcouldalterthepatient’sperceptionand
his responsiveness to the incidence of propofol injection pain.
Previousstudiesthatusedremifentaniltoreduce propo-fol injection pain have methodological differences from thepresent study.Roehmetal.,46 in2003, collecteddata
from patients pretreated with midazolam, using venous catheteronthedorsumofthehandandcontinuousinfusion of remifentanil.Batra etal.,51 in2004, usedbolus doses,
butwithvenipunctureinthebackofthehandofpediatric patients,inadditiontousingbehavioralparametersfor mea-surementofpain,suchaspresenceofgrimace,cry,andhand removal,andnotbypatient’sobjectiveresponse.Although propofolthe timeofbalance isgreater thanthe remifen-tanil,remifentanilwasgivenfirstbecauseoneofthestudy’s objectives wasprecisely toassess theinterference in the propofoldoserequiredfortheexam.
The objectives were effectively proven. In additionto a significant reductionin propofolinjection pain,we also foundasignificantreductioninthepropofoldose required fordiagnosticUDE.
Thedifferenceinresultscomparedwithpreviousstudies maybe dueto non-useof premedication,different injec-tionrate,differentagepopulationsample,choiceoflarger caliberveinsoftheantecubitalregion,andpre-injectionof remifentanilindifferentdosestopreviousstudies.
Inthisstudy,theassessmentofsedationwithpropofolin combinationornotwithremifentanilinpatientsundergoing diagnosticUDEallowedthefollowingconclusions:
Pretreatment with remifentanil significantly reduced propofolinjectionpain.
Pretreatmentwithremifentanil significantlyreduced the propofoldoserequiredforsedation.
Therewasnostatistically significant differencebetween the groups receiving pretreatment with remifentanil at dosesof0.2g/kgand0.3g/kgregardingpropofol
injec-tionpainandinterferenceintheuseddoseofpropofol.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.PambiancoDJ, Vargo JJ,Pruitt RE,et al. Computer-assisted personalizedsedation for upperendoscopyand colonoscopy: a comparative, multicenter randomized study. Gastrointest Endosc.2011;73:765---72.
2.CohenLB,WecslerJS,GaetanoJN,etal.Endoscopicsedation intheUnitedStates:resultsfroma nationwidesurvey.AmJ Gastroenterol.2006;101:967---74.
3.LewisJR,CohenLB.Updateoncolonoscopypreparation, pre-medication,andsedation.ExpertRevGastroenterolHepatol. 2013;7:77---87.
4.Diprivan(propofol)injectableemulsion[packageinsert]. Wil-mington,DE:AstrazenecaPharmaceuticals;2005.
7.StarkRD,BinksSM,DutkaVN,etal.Areviewofthesafetyand toleranceofpropofol(Diprivan).PostgradMedJ.1985;61Suppl 3:152---6.
8.MangarD,HolakEJ.Tourniquetat50mmHgfollowedby intra-venouslidocainediminisheshandpainassociatedwithpropofol injection.AnesthAnalg.1992;74:250---2.
9.MacarioA,WeingerM,TruongP,etal.Whichclinicalanesthesia outcomesarebothcommonandimportanttoavoid?The per-spectiveofapanelofexpertanesthesiologists.AnesthAnalg. 1999;88:1085---91.
10.Wallentine CB, Shimode N, Egan TD, et al. Propofol in a modifiedcyclodextrinformulation:firsthumanstudyof dose-response with emphasis on injection pain. Anesth Analg. 2011;113:738---41.
11.DyeDWJ.SuspectedanaphylacticreactiontoCremoforEL.Br MedJ.1980;280:1353.
12.KlementW, ArndtJO. Pain oninjection ofpropofol:effects of concentration and diluents. Br J Anaesth. 1991;67: 281---4.
13.VonDardelO,Mebius C,MossbergT,etal.Fatemulsionasa vehiclefordiazepam.Astudyin9,294patients.BrJAnaesth. 1983;55:41---7.
14.GranL, Bleie H, Jeppson R, et al. Etomidat mil intralipid. Eine losung zur schmerzfreien injection. Anaesthetist. 1983;32:475---7.
15.NymanY, Von Hofsten K, PalmC,et al. Etomidate-Lipurois associated with considerably less injection pain in children comparedwithpropofolwithaddedlidocaine.Br JAnaesth. 2006;97:536---9.
16.ShaoX,LiH,WhitePF,etal.Bisulfite-containingpropofol:isit acost-effectivealternativetoDiprivanforinductionof anes-thesia?AnesthAnalg.2000;91:871---5.
17.Kunitz O, Losing R, Schulz-Stubner S, et al. Propofol-LCT versuspropofol-MCT/LCTwithorwithoutlidocaine:a compar-isononpainoninjection.AnasthesiolIntensivmedNotfallmed Schmerzther.2004;39:10---4.
18.RohmKD,Piper SN,SchollhornTA, etal. Injectionpain sec-ondarytopropofol-MCT/LCTandpropofol-LCT:comparisonof prophylaxiswithlidocaine.AnasthesiolIntensivmedNotfallmed Schmerzther.2003;38:643---7.
19.LarsenB,BeerhalterU,BiedlerA,etal.Lesspainoninjection byanewformulationofpropofol:acomparisonwithpropofol LCT.Anaesthesist.2001;50:842---5.
20.DubeyPK, KumarA. Pain oninjection of lipid-freepropofol and propofol emulsion containing medium-chain triglyc-eride: a comparative study. Anesth Analg. 2005;101: 1060---2.
21.LarsenR,BeerhalterU,ErdkonigR,etal.Injectionpainfrom propofol-MCT-LCTinchildren:acomparisonwithpropofol-LCT. Anaesthesist.2001;50:676---8.
22.Rochette A, Hocquet AF, Dadure C, et al. Avoiding propo-fol injection pain in children: a prospective, randomized, double-blinded, placebo-controlled study. Br J Anaesth. 2008;101:390---4.
23.O’HaraJF,SprungJ,LaseterJT,etal.Effectsoftopical nitro-glycerinandintravenouslidocaineonpropofol-inducedpainon injection.AnesthAnalg.1997;84:865---9.
24.CheongMA,KimKS,ChoiWJ.Ephedrinereducesthepainfrom propofolinjection.AnesthAnalg.2002;95:1293---6.
25.AgarwalA,AnsariMF,GuptaD,etal.Pretreatmentwith thiopen-talforpreventionofpainassociatedwithpropofolinjection. AnesthAnalg.2004;98:683---6.
26.MemisD,TuranA,KaramanliogluB,etal.Theuseofmagnesium sulfatetopreventpainoninjectionofpropofol.AnesthAnalg. 2002;95:606---8.
27.KooSW,ChoSJ,KimYK,etal.Small-doseketaminereducesthe painofpropofolinjection.AnesthAnalg.2006;103:1444---7.
28.Canbay O, Celebi N, Arun O, et al. Efficacy of intravenous acetaminophenandlidocaineonpropofolinjectionpain.BrJ Anaesth.2008;100:95---8.
29.BorazanH,SahinO,KececiogluA,etal.Preventionof propo-fol injectionpainin children:a comparisonof pretreatment withtramadolandpropofol---lidocainemixture.IntJMedSci. 2012;9:492---7.
30.Aouad MT, Siddik-Sayyid SM, Al-Alami AA, et al. Multimodal analgesiatopreventpropofol-inducedpain:pretreatmentwith remifentanil and lidocaine versus remifentanil or lidocaine alone.AnesthAnalg.2007;104:1540---4.
31.Al-Refai AR, Al-Mujadi H, Ivanova MP, et al. Prevention of pain on injection of propofol: a comparison of remifen-tanilwithalfentanilinchildren.MinervaAnestesiol.2007;73: 219---23.
32.Basaranoglu G, ErdenV, Delatioglu H. Reduction ofpain on injectionofpropofol:acomparisonoffentanylwith remifen-tanil.AnesthAnalg.2002;94:1040---1[Letter].
33.Minto CF, Schnider TW, Short TG, et al. Response sur-face model for anesthetic drug interactions. Anesthesiology. 2000;92:1603---16.
34.DuarteNMC,PiresOC,NunesCEL,etal.Anestesiavenosatotal. RiodeJaneiro:SociedadeBrasileiradeAnestesiologia;2011.p. 73---82.
35.Hayes JA, Lopez AV, Pehora CM, et al. Coadministration of propofol and remifentanil for lumbar puncture in children. Anesthesiology.2008;109:613---8.
36.WangD,ChenC,ChenJ,etal.Theuseofpropofolasasedative agentingastrointestinalendoscopy:ameta-analysis.PLOSONE. 2013;8:e53311.
37.Scott RP, Saunders DA, Norman J. Propofol: clinical strate-gies for preventing the pain of injection. Anaesthesia. 1988;43:492---4.
38.TanLH,HwangNC.Theeffectofmixinglidocainewithpropofol onthedose ofpropofolrequiredforinductionofanesthesia. AnesthAnalg.2003;97:461---4.
39.Eriksson M, Englesson S, Horte I, et al. The anaesthetic potency of propofol in the rat is reduced by simultaneous intravenous administrationoflignocaine.EurJ Anaesthesiol. 1999;16:315---9.
40.ErikssonM.Prilocainereducesinjectionpaincausedby propo-fol.ActaAnaesthesiolScand.1995;39:210---3.
41.Egan TD, Kern SE, Muir KT, et al. Remifentanil by bolus injection: a safety,pharmacokinetic,pharmacodynamic, and age effectinvestigation inhuman volunteers.Br JAnaesth. 2004;92:335---43.
42.LaPierreCD,JohnsonKB,RandallBR,etal.Asimulationstudy ofcommonpropofol andpropofol-opioiddosingregimens for upperendoscopy.Anesthesiology.2012;117:252---62.
43.Drover DR, Litalien C, Wellis V, et al. Determination ofthe pharmacodynamicinteractionofpropofolandremifentanil dur-ing esophagogastroduodenoscopyin children. Anesthesiology. 2004;100:1382---6.
44.JeongCW,LeeSH,JuJ,etal.Theeffectofpriminginjectionof differentdosesofremifentaniloninjectionpainof microemul-sionpropofol premixedwithlidocaine.KoreanJAnesthesiol. 2011;60:78---82.
45.Fidler M, Kern SE. Flexible interaction model for com-plex interactions of multiple anesthetics. Anesthesiology. 2006;105:286---96.
46.Roehm KD, Piper SN, Maleck WH, et al. Prevention of propofol-induced injection pain by remifentanil: a placebo-controlled comparison with lidocaine. Anaesthesia. 2003;58: 165---70.
48.BasaranogluG,ErdenV,DelatiogluH,etal.Reductionofpain oninjectionofpropofolusingmeperidineandremifentanil.Eur JAnaesthesiol.2005;22:890---2.
49.IyilikciL,BalkanBK,GokelE,etal.Theeffectsofalfentanil orremifentanilpretreatmentonpropofolinjectionpain.JClin Anesth.2004;16:499---502.
50.Lee JY, Yang HJ, Choi SH, et al. The optimal effect-site concentrationofremifentaniltoattenuatethepaincausedby propofol.KoreanJAnesthesiol.2012;63:108---12.