REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Anesthesia
management
by
residents
does
not
alter
the
incidence
of
recall
of
tracheal
extubation:
a
teaching
hospital-based
propensity
score
analysis
Satoki
Inoue
∗,
Ryuichi
Abe,
Yuu
Tanaka,
Masahiko
Kawaguchi
NaraMedicalUniversity,DepartmentofAnesthesiologyandDivisionofIntensiveCare,Shijo-choKashihara,Nara,Japan
Received15December2015;accepted23February2016 Availableonline17April2016
KEYWORDS
Awareness; Airwayextubation; AcademicMedical Centers
Abstract
Backgroundandobjectives: Thememoryofemergencefromanesthesiaisrecognizedasone
typeofanesthesiaawareness.Apartfromplanedawakeextubation,unintentionalrecallof tra-chealextubationisthoughttobetheresultsofinadequateanesthesiamanagement;therefore, theincidencecanberelatedwiththeexperienceofanesthetists.Toassesswhetherthe inci-denceofrecalloftrachealextubationisrelatedtoanesthetists’experience,wecomparedthe incidenceofrecalloftrachealextubationbetweenpatientsmanagedbyanesthesiaresidents orbyexperiencedanesthetists.
Methods:Thisisaretrospectivereviewofaninstitutionalregistrycontaining21,606general
anesthesiacases andwas conductedwiththeboardofethical reviewapproval.Allresident trachealextubationswereperformedunderanesthetists’supervision.Toavoidchannelingbias, propensityscoreanalysiswasusedtogenerateasetofmatchedcases(residentmanagements) andcontrols(anesthetistmanagements),yielding3,475matchedpatientpairs.Theincidence ofrecalloftrachealextubationwascomparedasprimaryoutcomes.
Results:Intheunmatchedpopulation,therewasnodifferenceintheincidencesofrecallof
trachealextubationbetweenresidentmanagementandanesthetistmanagement(6.5%vs.7.1%,
p=0.275).Afterpropensityscorematching,therewasstillnodifferenceinincidencesofrecall oftrachealextubation(7.1%vs.7.0%,p=0.853).
Conclusion: Inconclusion,whensupervisedbyananesthetist,residentextubationsarenomore
likelytoresultinrecallthananesthetistextubations.
©2016SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗Correspondingauthor.
E-mail:[email protected](S.Inoue). http://dx.doi.org/10.1016/j.bjane.2016.02.008
PALAVRAS-CHAVE
Consciência; Extubac¸ão; CentrosMédicos Acadêmicos
Aadministrac¸ãodeanestesiaporresidentesnãoalteraaincidênciadememória daextubac¸ãotraqueal:umaanálisedepontuac¸ãodepropensãobaseadanoensino hospitalar
Resumo
Justificativaeobjetivos: Arecordac¸ãodaemergência daanestesia éreconhecida como um
dostiposdememóriadaanestesia.Excluindoaextubac¸ãoplanejadacomopacienteacordado, acredita-sequearecordac¸ãonãointencionaldaextubac¸ãotraquealsejaoresultadodemanejo inadequadodaanestesia;portanto,aincidênciapodeestarrelacionadacomaexperiênciados anestesistas.Paraavaliarseaincidênciaderecordac¸ãodaextubac¸ãotraquealestárelacionada coma experiência dos anestesistas,comparamos aincidência de recordac¸ão daextubac¸ão traquealentrepacientestratadosporresidentesdeanestesiaouporanestesistasexperientes.
Métodos: Estudoretrospectivoderevisãodeumregistoinstitucionalcontendo21.606casosde
anestesiageral,conduzidocomaaprovac¸ãodoComitêdeÉtica.Todasasextubac¸ões traque-ais foram realizadas por residentessob asupervisão de anestesistas. Para evitar oviés de canalizac¸ão,aanálisedoíndicedepropensãofoiusadaparagerarumgrupodecasospareados (manejoporresidentes)edecontroles(manejoporanestesistas),obtendo-se3.475pares com-binadosdepacientes.Aincidênciadememóriaduranteaextubac¸ãotraquealfoicomparada comosdesfechosprimários.
Resultados: Na populac¸ão incomparável, não houve diferenc¸a na incidência de recall de
extubac¸ãotraquealentreagestãoresidenteegestãoanestesista.(6,5%vs.7,1%,p=0,275). Depoisdecorrespondênciaescoredepropensão,aindanãohaviadiferenc¸anaincidênciade recalldeextubac¸ãotraqueal(7,1%vs.7,0%,p=0,853).
Resultados: Napopulac¸ãonãopareada,nãohouvediferenc¸anaincidênciaderecordac¸ãoda
extubac¸ãotraquealentreomanejoporresidenteseomanejoporanestesistas(6,5%vs.7,1%,
p=0,275).Apósparearosíndicesdepropensão,tambémnãohouvediferenc¸anaincidênciade recordac¸ãodaextubac¸ãotraqueal(7,1%vs.7,0%,p=0,853).
Conclusão:Em conclusão, quandosupervisionados porum anestesista, asextubac¸ões feitas
porresidentesnãosãomaispropensasaresultaremrecordac¸ãoqueasextubac¸õesfeitaspor anestesistas.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Thememoryofemergencefromanesthesiaisrecognizedas oneoftypesofanesthesiaawareness.1,2Apartfromdifficult
airway cases, awake tracheal extubation is unnecessary.3
Though,asaresultofpracticalchangesinanesthesia includ-ingdevelopmentofshortactingdrugsandenhancedpatient recovery and operating room turnover,it mayreasonably bepredicted that patients more frequently awake during emergencefromgeneralanesthesia.Onoccasion, uninten-tionallypatientsmightbefullyawakenedduringemergence. Patientswhoreportedaccidental awareness during emer-gence rarely mentioned feeling the trachealtube per se, butrathertheyexperienceddistressingparalysis.1,2
There-fore, the incidence of recall of tracheal extubation can beoverlookedandhappenmorefrequentlythanexpected. Takahashi etal.4 reportedthat of 1993 surgical patients,
202 had the memory of tracheal extubation. They found thatsex, age,andanesthesiamaintainedby propofolwas relatedtothememoryoftrachealextubation.4Inaddition,
they considered that the memory of tracheal extubation contributes to patient’s dissatisfaction with anesthesia.4
Therefore,feelingthetrachealtubeshouldbeunpleasantat themoment,therefore,itcanbeanunpleasantexperience
duringanesthesiaiftherecallisexplicitorconscious mem-ory.Itisreasonabletothinkthataccidentalfullawakeness duringemergenceisrelatedtolackofeducationand knowl-edge about the variability of duration of neuromuscular blockadeandtherapidityofoffsetofnewervolatileagents andpropofol,which might resultininadvertent mismatch betweenthetimecourseofreturnofconsciousness,return ofmotorcapacity,andthetimingfortrachealextubation.2
Therefore, unintentional recall of tracheal extubation is thoughttoberesultsofinadequateanesthesiamanagement; therefore, the incidence can be related with the experi-enceofanesthetists.However,itisnotclearwhetherornot anesthetists’ experienceaffectstheincidenceofrecall of trachealextubationoranyinvestigationaboutthisconcern hasneverbeenreported.
byresidentsinanesthesiologyonrecalloftracheal extuba-tion.Toreduce theeffectofselection bias,we compared theincidenceofrecalloftrachealextubationin propensity-matchedpairswithanesthesiamanagementbyresidentsor byconsultantanesthetists.
Methods
Approvalforreviewofpatientclinicalchartsandaccessto dataoftheinstitutional registryof anesthesia,and repor-tingtheresultswasobtainedfromtheInstitutionalReview Board.Therequirementfor written informedconsentwas waivedbytheInstitutionalReviewBoard.
Perioperativepatienttreatment
No standardization was made for the methods of induc-tion and maintenance of anesthesia. However, methods of anesthesia did not differ so much because this study was performed in a single hospital. No premedication was used. General anesthesia was usually induced with intravenous propofol (1---2.5mg·kg−1) plus either fentanyl
(0.1---0.2g·kg−1) or remifentanil (0.2---0.3g·kg−1·min−1), andneuromuscularblockadewasachievedwithrocuronium (0.6---0.9mg·kg−1). In most cases, bispectral index
moni-toring was used; however, the decision of use depended on the attendant’s preference. Tracheal intubation was performed using a Macintosh-type laryngoscope. Tracheal intubations were performed by residents under the guid-ance of the registered (consultant) anesthetist or by the consultant anesthetist.A resident wasdefinedasa medi-cal school graduate, who had a medical qualification, in a two-year mandatory clinical training program currently onrotationinthe anesthesiadepartment(for acoupleof months)oraresidentanesthetistinatwo-yeartrainingafter the mandatory training. In Japan, anesthetists can apply forregistered anesthetiststatustotheMinistry ofHealth, LabourandWelfareaftertwoyearsoftrainingasa mem-beroftheJapaneseSociety ofAnesthesiologists.Allthese residentshavecompletedasimulation-basedtrainingcourse in airwaymanagementand passed thepractical examina-tionaboutairwaymanagement.Anesthesiawasmaintained with sevofiurane (1.5---2%) in a 40% oxygen and air mix-tureorwithpropofol(6---10mg·kg−1
·h−1).Nitrousoxidewas
not used. Fentanyl (0.1---0.2g·kg−1·h−1) or remifentanil (0.1---0.2g·kg−1·min−1) were used for analgesia. Rocuro-nium (0.2---0.3mg·kg−1
·h−1) was used for neuromuscular
blockade and sugammadex (2---4mg·kg−1) for reversal of
neuromuscular blockade after evaluating status of neu-romuscular blockade by a nerve stimulator. Immediately afterpatientsregainedconsciousness,trachealextubation wasperformed. Exceptdifficult airwaycases,fullyawake extubationwasnotplaned.Trachealextubationswerealso performedbyresidentsundertheguidanceofthe consult-antanesthetistorbytheconsultantanesthetist.Incaseof managementofresidents,residentsfirstinformed consult-antanesthetists ofthe end of surgery througha personal handyphonesysteminadvanceofpatient’semergencefrom anesthesia. Again,residentscalled consultantanesthetists to come and see after they judged that extubation was possible inthe case.The timing for thecalldepended on
the situations. Occasionally, postoperative analgesia was providedwithintravenousfentanylorepiduralropivacaine combinedwithfentanylusingapatientcontrolled analge-siadevice. After completionof anesthesia, the attendant in charge filled out the form for the institutional reg-istry of anesthesia, which includes the attendant’sname, the name of the person who performed intubation, the patient’sdemographicvariables,informationonfinal diag-nosisandsurgicalprocedures(latercategorizedintothree classesbasedonthemodified surgicalriskstratification),5
backgroundillnesses(hypertension,diabetesmellitus, coro-naryarterydisease,historyofheartfailure,lungdisease), duration of anesthesia and surgery, ASA physical status, urgencyofsurgery(emergencyorelective),anesthesia tech-nique(inhalationalorintravenouswithorwithoutregional analgesia),intraoperativepatientpositioning,finalairway assessment, requirement of transfusion, implementation of postoperative analgesia, requirement of postoperative intensivecare,andadverse intraoperativeevents(cardiac events,hypotension,arrhythmia,hypoxia,etc.).The atten-dantinchargeofthecasealsofollowed-upthepatientand recordedanycomplicationincludinganyunpleasant experi-enceduringanesthesiaoverseveralpostoperativedays.In addition,untilthe14thpostoperativeday,thepatients com-pletedaquestionnaire,includingitemsonrecalloftracheal extubation.The incidenceofrecalloftrachealextubation wasdetermined by referring to both the patient’s report and the postanesthetic round record. Intensity of recall (implicit or explicit memory) was not distinguished, but lumpedtogetherandtreatedasthefinalanswer.
Datahandling
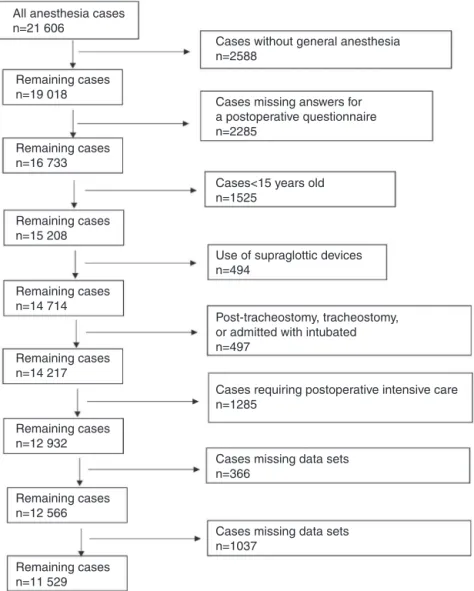
DatawerecollectedbetweenJanuary2009andDecember 2013,duringwhichtherewere21,606anesthesiacases.The exclusioncriteriaforthecurrentstudy(andreasonsfor con-sequentreductionsineligiblepatients)wereasfollows:(1) caseswithoutgeneralanesthesia(n=2588),(2)cases miss-inganswers onthe postoperative questionnaireor unable toanswer the questionnaire due to disturbanceof cogni-tivedysfunction(n=2285),(3)cases<15-year-old(n=1525), (4) use of supraglottic devices (n=494), (5) cases with post-tracheostomy,undergoing tracheostomy, or admitted withintubated(n=497),(6)casesjudgedasdifficultairway becausefully awake extubation wasusually performed in suchcases(n=366), (7)cases missingdata sets(n=1037) (Fig.1).
Statisticalanalysis
All anesthesia cases n=21 606
Cases without general anesthesia n=2588
Cases<15 years old n=1525
Use of supraglottic devices n=494
Cases missing data sets n=1037
Cases missing data sets n=366
Cases requiring postoperative intensive care n=1285
Post-tracheostomy, tracheostomy, or admitted with intubated n=497
Cases missing answers for a postoperative questionnaire n=2285
Remaining cases n=19 018
Remaining cases n=16 733
Remaining cases n=15 208
Remaining cases n=14 714
Remaining cases n=14 217
Remaining cases n=12 932
Remaining cases n=12 566
Remaining cases n=11 529
Figure1 Flowdiagramforpatientinclusionandexclusion.
Next, to avoid channeling bias, we used propensity scoreanalysistogenerateasetofmatchedcases(resident managements) and controls (anesthetist managements). Ultimately,4579patientswereexcludedfromtheanalysis. Apropensityscorewasgeneratedfor each patientfroma multivariablelogisticregressionmodelbasedonthe covari-ates, which included the institutional registry data items suchasthepatient’sdemographicvariables,surgical risk, background illnesses, duration of anesthesia and surgery, ASA physical status, urgency of surgery, anesthesia tech-nique, intraoperative patient positioning, requirement of transfusion,implementationofpostoperativeanalgesia,and adverse intraoperative events, as independent variables, withtreatmenttype(residentmanagementvs.anesthetist management)asabinarydependentvariable.Assuggested byareviewofstatisticalresearchonpropensityscore devel-opment,weusedastructurediterativeapproachtorefine this model, with the goal of achieving covariate balance betweenthematched pairs.6 Covariatebalancewas
mea-suredusingthestandardizeddifference,whereanabsolute difference of <0.1 was taken as a meaningful covariate imbalance.7 Wematchedpatientsusingagreedy-matching
algorithm with a caliper width 0.001 of the estimated
propensity score. A matching ratio of 1:1 was used.This procedure yielded 3475 patients managed by residents propensitymatchedto3475patientsmanagedbyconsultant anesthetists.Forstatisticalinference,methodsthataccount forthematchednatureofthesampleswereused.Foroverall incident rate, the Cochran---Mantel---Haenszel test, strati-fied onthe matched pair, wasused toestimate the odds ratioand95%CIofincidence(residentmanagementvs. con-sultantanesthetistmanagement).Analyseswerecomputed usingR(version3.0.3,RFoundationforStatistical Comput-ing,Vienna,Austria).Ap<0.05wasconsideredstatistically significant.
Samplesizecalculation
Wefinallyconductedasamplesizecalculation.Weassumed a10%incidenceoftrachealextubationrecallbasedonthe previous report from the previous report.4 We estimated
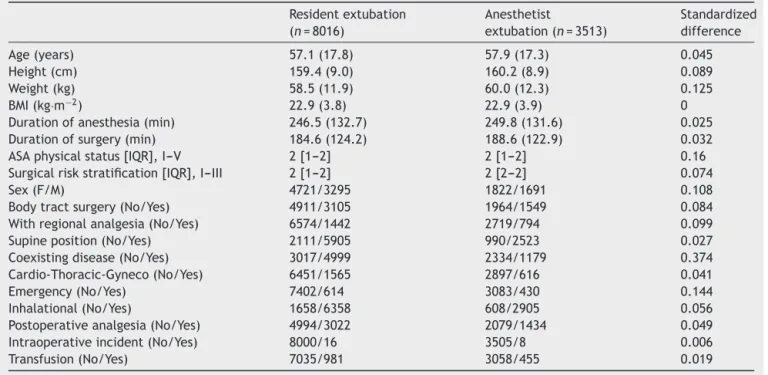
Table1 Clinicalcharacteristicsofthetwounmatchedstudygroups.
Residentextubation (n=8016)
Anesthetist
extubation(n=3513)
Standardized difference
Age(years) 57.1(17.8) 57.9(17.3) 0.045
Height(cm) 159.4(9.0) 160.2(8.9) 0.089
Weight(kg) 58.5(11.9) 60.0(12.3) 0.125
BMI(kg·m−2) 22.9(3.8) 22.9(3.9) 0
Durationofanesthesia(min) 246.5(132.7) 249.8(131.6) 0.025 Durationofsurgery(min) 184.6(124.2) 188.6(122.9) 0.032 ASAphysicalstatus[IQR],I---V 2[1---2] 2[1---2] 0.16 Surgicalriskstratification[IQR],I---III 2[1---2] 2[2---2] 0.074
Sex(F/M) 4721/3295 1822/1691 0.108
Bodytractsurgery(No/Yes) 4911/3105 1964/1549 0.084 Withregionalanalgesia(No/Yes) 6574/1442 2719/794 0.099 Supineposition(No/Yes) 2111/5905 990/2523 0.027 Coexistingdisease(No/Yes) 3017/4999 2334/1179 0.374 Cardio-Thoracic-Gyneco(No/Yes) 6451/1565 2897/616 0.041
Emergency(No/Yes) 7402/614 3083/430 0.144
Inhalational(No/Yes) 1658/6358 608/2905 0.056
Postoperativeanalgesia(No/Yes) 4994/3022 2079/1434 0.049 Intraoperativeincident(No/Yes) 8000/16 3505/8 0.006
Transfusion(No/Yes) 7035/981 3058/455 0.019
Valuesaremean(SD),median[IQR],ornumber.
wassafetosaythatoursamplesizewassufficienttodetect adifferenceinoutcome.
Results
Median(IQR)yearsofexperiencewas1.8(1---2.7)for resi-dentsand 13(9---18) for consultant anesthetists. Recallof trachealextubationwasobservedin773of11,529patients, whichcomesto6.7%oftheoverallincidentrate.Therewas nopatientwithrecalloftrachealextubationwhoresulted in serious psychological sequelae. The clinical character-istics of the two groups (patients managed by residents and patients managed by consultant anesthetists) based on11,529 patients arepresented in Table 1.Many of the variablesweresimilarbetweengroups(standardized differ-ence<0.1) before matching. However, variables including weight, sex, ASA physical status, presence of co-existing disease, emergency case were imbalanced, one of which waspreviouslyreportedfactorsinfluencingthememoryof tracheal extubation.Patient outcomes aresummarized in
Table2.Theincidenceofrecalloftrachealextubationdid notdifferbetweentrachealextubationbyresidentsand tra-chealextubationbyconsultantanesthetists(6.5%vs.7.1%). The clinical characteristics of the twomatched groups (patientswhosetracheaswereextubatedbyresidentsand
patientswhosetracheaswereextubatedbyconsultant anes-thetists)extractedbypropensityanalysisarepresentedin
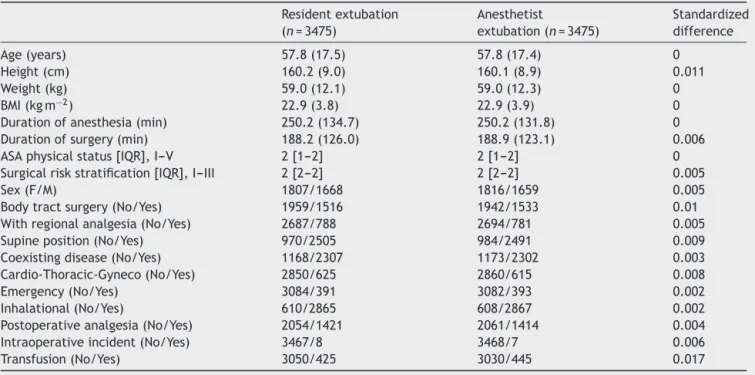
Table3.Accordingtothestandardizeddifference,covariate balancebetweenthematchedpairswasconfirmed.Patient outcomesaresummarizedinTable4.Theincidenceofrecall oftrachealextubationdidnotdifferbetweentracheal extu-bationby residentsandtrachealextubation byconsultant anesthetistsafterpropensitymatching(7.1%vs.7.0%).
Discussion
Theincidenceofrecalloftrachealextubationdidnot dif-ferbetweenanesthesiacasesmanagedbyresidentsandby consultant anesthetists. This study suggests that patients receive equal medical care regarding possible unpleas-antexperienceduringtrachealextubation andemergence in teaching hospitals because residents are appropriately trainedbeforeparticipatinginanesthesiamanagementand arecloselysupervisedbyconsultantanesthetistthroughout theemergenceprocess.
As mentioned in ‘‘Methods’’ section, we leaved resi-dentstojudgethetimingforextubationbecauseresidents were sufficientlytrained and educated before participat-inginanesthesiamanagement.However,weassumedthat thetimecourse mismatchduringemergence processfrom
Table2 Patientoutcomepriortomatching.
Resident extubation
Anesthetist extubation
Oddsratio(95%CI) Effectsize p-Value
Incidenceofrecallof extubation(n=Yes/No)
Table3 Clinicalcharacteristicsofthetwostudygroupsafterpropensityscorematching.
Residentextubation (n=3475)
Anesthetist
extubation(n=3475)
Standardized difference
Age(years) 57.8(17.5) 57.8(17.4) 0
Height(cm) 160.2(9.0) 160.1(8.9) 0.011
Weight(kg) 59.0(12.1) 59.0(12.3) 0
BMI(kgm−2) 22.9(3.8) 22.9(3.9) 0
Durationofanesthesia(min) 250.2(134.7) 250.2(131.8) 0 Durationofsurgery(min) 188.2(126.0) 188.9(123.1) 0.006 ASAphysicalstatus[IQR],I---V 2[1---2] 2[1---2] 0 Surgicalriskstratification[IQR],I---III 2[2---2] 2[2---2] 0.005
Sex(F/M) 1807/1668 1816/1659 0.005
Bodytractsurgery(No/Yes) 1959/1516 1942/1533 0.01 Withregionalanalgesia(No/Yes) 2687/788 2694/781 0.005 Supineposition(No/Yes) 970/2505 984/2491 0.009 Coexistingdisease(No/Yes) 1168/2307 1173/2302 0.003 Cardio-Thoracic-Gyneco(No/Yes) 2850/625 2860/615 0.008
Emergency(No/Yes) 3084/391 3082/393 0.002
Inhalational(No/Yes) 610/2865 608/2867 0.002
Postoperativeanalgesia(No/Yes) 2054/1421 2061/1414 0.004 Intraoperativeincident(No/Yes) 3467/8 3468/7 0.006
Transfusion(No/Yes) 3050/425 3030/445 0.017
Valuesaremean(SD),median[IQR],ornumber.
anesthesiacouldincreasebecauseoflackofclinical experi-encebutnotknowledgenoreducation,whichwouldresult in increase of theincidence of recall of tracheal extuba-tion.Inaddition,wealsoexpectedthatinexperiencewould have affected the extubation process, which might have takenmoretimethan incase of experiencedanesthetist. Onthecontrarytoourassumption,theincidenceofrecall oftrachealextubationdidnotincreaseinanesthesiacases managedbyresidents.Thereasonforthisresultmightbe becauseresidentscalledconsultantanesthetistsearlierthan expected and consultant anesthetists properly supervised theemergenceprocessandtheextubationprocessdoesnot consistofverycomplexprocedures.Inthispoint,weshould haveneededtodeclareinadvancethat,unfortunately,such mismatch could not be evaluated retrospectively in our anesthesiaregistrydatabase becausethedatabasedidnot includesuchinformation.
Occasionally,recallduringtrachealextubationand emer-gence from anesthesia can be recognized as a kind of accidental awareness during general anesthesia.1,2 Most
patientswhoreported accidentalawareness during emer-gencerarelymentionedfeelingthetrachealtubeperse,but rathertheyexperienceddistressing paralysis.1,2Wecannot
distinguishpatients who reportedrecall of tracheal extu-bationfromoneswithdistressingparalysisoroneswithout
distressing paralysisby thepostanesthetic interviewdata. Also, we cannot either distinguish patients who reported recall of tracheal extubation from ones who took it as unpleasantexperienceornot.Consideringthatourpractical protocolfacilitatedtouseanervestimulatorandtherewas nopatientwithrecalloftrachealextubationwhoresulted in any seriouspsychological outcomesat least during this followupperiod,itmayseemasifso-called‘‘awake extu-bation’’ had been unintentionally performed in our cases althoughthetruthremainsunknownduetothelackofdata sources.Eitherway,ithasbeenreportedthatthememoryof trachealextubationcontributestopatient’sdissatisfaction withanesthesia.4 Inaddition,acasehasbeen reportedin
whichmemoryofeventsduringemergencefromanesthesia resultedinseriouspsychologicalsequelae.8Therefore,itis
importanttoinformthepatientsofthepossibilityofrecall ofthetubeintheairwayordifficultyinmovingorbreathing atthistimeinadvanceofprovisionofgeneralanesthesia.2
Thereareseverallimitationsofthestudythatmerit dis-cussion.Thereisagrowinginterestintheuseofpropensity score-based methods in observational studies to estimate treatment effects. The propensity score is defined asthe conditional probability of assigning a subject to a par-ticular treatment protocol given a vector of measured covariates.9,10 To minimize theeffectof selection biason
Table4 Patientoutcomeafterpropensitymatching.
Resident extubation
Anesthetist extubation
Oddsratio(95%CI) Effectsize p-Value
Incidenceofrecallof extubation(n=Yes/No)
outcomes,we used propensity scorematching for clinical characteristics to reduce distortion by confounding fac-tors.However,thisstudywasretrospectiveinnature;thus, unmeasuredvariables couldstillconfoundtheresults.We used data from the institutional registry of anesthesia, which includes only minimum essential informationabout each case but does not include precise details. There-fore, we did not obtain several variables which might have affectedrecall oftracheal extubation.However,our anesthesia practices were relatively constant during the sampling period, so the effects of unmeasured variables werelikelyminimal.Datawerealsonotavailableregarding neuromuscular function at tracheal extubation, a critical determinant of unpleasant experience during emergence fromanesthesia.1,2 But, consultantanesthetists mayhave
closelysupervisedtheemergence process.Thus,itis sup-posed that motor capacity at tracheal extubation was equivalent whether managed by residents or consultant anesthetists.Theincidenceofrecalloftrachealextubation inthisstudy(773:11,529)wasconsiderablyhighercompared withthereportofthe5thNationalAuditProject(1:69,200or 1:35,000).2Thereasonwasthoughttobethatwedidnot
dis-tinguishtherecallfromimplicitorexplicitmemory.Previous Japanese study,whichusedthesame questionnaireabout anesthesia care, showed almost the same incidence rate (10.1%).4 Nopremedication wasgiven inthis study,which
might explain the relatively high incidenceof awareness. Finally,theconsiderable numberof patientswasexcluded fromthestudy.However,theexcluded patientsmight not have affected the results because theexclusion was per-formedaccordingtotheobjectivecriteriaandthemissing datawereatleastmissingatrandom.
Summary
Whensupervisedbyananesthetist,residentextubationsare nomorelikelytoresultinrecall thananesthetist extuba-tions.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.PanditJJ,AndradeJ,BogodDG,etal.The5thNationalAudit Project(NAP5)onaccidentalawarenessduringgeneral anaes-thesia:summaryofmainfindingsandriskfactors.Anaesthesia. 2014;69:1089---101.
2.PalmerJHM,O’SullivanEP,RadcliffeJJ.Chapter10AAGA dur-ingextubationandemergence.In:PanditJJ,CookTM,editors. NAP55thNationalAuditProjectofTheRoyalCollegeof Anaes-thetistsand theAssociationofAnaesthetistsofGreatBritain andIreland.AccidentalAwarenessduringGeneralAnaesthesia intheUnitedKingdomandIreland,London.TheRoyalCollege ofAnaesthetists.;2014.p.84---92.
3.Difficult Airway Society Extubation Guidelines Group, Popat M, Mitchell V, et al. Difficult Airway Society Guidelines for the management of tracheal extubation. Anaesthesia. 2012;67:318---40.
4.TakahashiM,NakahashiK,KarashimaY,etal.Thememoryof tracheal extubationduringemergencefrom general anesthe-sia.Masui(JpnJAnesthesiol).2001;50:613---8[inJapanesewith Englishabstract].
5.Eagle KA, Berger PB, Calkins H, et al. ACC/AHA guideline update for perioperative cardiovascular evaluation for non-cardiacsurgery----executivesummaryareportoftheAmerican CollegeofCardiology/AmericanHeartAssociation TaskForce onPracticeGuidelines(CommitteetoUpdatethe1996 Guide-linesonPerioperativeCardiovascularEvaluationforNoncardiac Surgery).Circulation.2002;105:1257---67.
6.Austin PC. Propensity-score matching in the cardiovascular surgery literature from 2004 to 2006: a systematic review and suggestionsfor improvement.J ThoracCardiovasc Surg. 2007;134:1128---35.
7.AustinPC,GrootendorstP,AndersonGM.Acomparisonofthe abilityofdifferentpropensity score modelstobalance mea-sured variables between treated and untreated subjects: a MonteCarlostudy.StatMed.2007;26:734---53.
8.HoAM.‘Awareness’and‘recall’duringemergencefromgeneral anaesthesia.EurJAnaesthesiol.2001;18:623---5.
9.D’AgostinoRBJr.Propensityscoremethodsforbiasreduction inthecomparisonofatreatmenttoanon-randomizedcontrol group.StatMed.1998;17:2265---81.