Artigo Original
Letícia Ribeiro Pifaia1 Glaucya Madazio2 Mara Behlau2
Descritores
Voz Acústica da fala Qualidade da voz Percepção auditiva Distúrbio da voz
Keywords
Voice Acoustic Voice quality Auditory perception Voice disorders
Correspondence address::
Letícia Ribeiro Pifaia
R. Correia de Lemos, 327, Apto 81, Chácara Inglesa, São Paulo (SP), Brasil, CEP: 04140-000.
E-mail: [email protected]
Received: 24/12/2010
Accepted: 22/9/2011
Study carried out at the Centro de Estudos da Voz – CEV– São Paulo (SP), Brazil. (1) Graduate program at Centro de Estudos da Voz - CEV - São Paulo (SP), Brazil.
Conlicts of iterests: nothing to declare.
rehabilitation
Diagrama de desvio fonatório e análise perceptivo-auditiva
pré e pós-terapia vocal
ABSTRACT
Objective: Verify whether PDD relects vocal changes obtained by vocal rehabilitation and whether it relects the changes in perceptual analysis. Methods: Samples of the sustained vowel / ε /, pre and post-therapy, from 34 individuals with different dysphonia diagnosis were collected. The voices were acoustically analyzed by the PDD and an auditory perceptual analysis was performed using a visual analog scale (VAS) of 100 points. The acoustic samples were classiied according to PDD density (concentrate or spread), shape (horizontal, vertical or circular) and position within the quadrants of the graph (lower left = 1, = lower right = 2, upper right = 3 and upper left = 4). Statistical analysis of acoustic parameters, distribution of samples and correlation between acoustic analysis and auditory perceptual analysis were performed. Results: Acoustic data showed improvement after therapy. Density did not differ in the two moments, while shape showed differences pre and post-therapy (p = 0.031). The vertical form characterized pre-therapy samples (12, 35.29%), and the circular form was associated to post-therapy samples (7, 20.59%). In pre-treatment condition, samples were distributed in three of the four quadrants, while in post-therapy, 90% were located in the irst quadrant (normality area). The average perceptual deviation reduced from moderate to mild-moderate (p <0.001). There is a relationship between quadrant location and perceptual analysis (p <0.001). Conclusion: PDD is useful to identify changes acquired with voice therapy and correlates with perceptual voice analysis.
RESUMO
INTRODUCTION
Voice production involves complex multidimensional aspects. For this reason it has to be analyzed in different per-spectives (1,2). Auditory perceptual and acoustic analyzes are the
main tools for vocal evaluation.
Auditory perceptual and acoustic analyzes are important clinical instruments that complement themselves for monitor-ing and followmonitor-ing patients’ development along the therapeutic process.Acoustic analysis, considered as an objective evaluation has recently become a reality in many voice clinics, since low cost voice acoustic’s analysis softwares were made available. Nowadays there are no inancial reasons for not performing acoustic analysis associated with auditory analysis in dysphonic patients(3). Auditory perceptual analysis provides important
information about the anatomy and physiology of the larynx, presence, degree and type of vocal deviation. It is considered the gold standard for voice evaluation, despite the fact that it is a subjective method(4-6).
Acoustic analysis allows the determination of isolated and combined measures. However, isolated acoustic measures of-fer partial information and can’t be representative of the vocal quality as a whole. Recent studies(7,8) have shown that the
association between acoustic and auditory measures should be complementary and not exclude either one or other.They can provide more descriptive information of the voice under analysis and therefore more useful, considering that they are important tools to monitor and follow-up patients in vocal training.
The Phonatory Deviation Diagram (PDD), from the VoxMetria software (CTS Informática), is a resource of acoustic analysis that uses combined parameters in a graphic presenta-tion. The diagram was originally proposed by a German group, and it was named as Hoarseness Diagram(7,9,10). Different from
other voice acoustic analyzes, PDD correlates four acoustic measures through a bi-dimensional graphic: horizontal axis relates to jitter, shimmer measures and their correlations and vertical axis presents GNE (glottal-to-noise excitation ratio) measure. PDD is being used in clinical practice to provide a more reliable vocal quality description, being able to follow-up dysphonic patients’ evolution. It also allows identifying any reducing vocal deviations, besides demonstrating the vocal sample distribution according to the normality area projected by the software(8).
PDD is able to differentiate dysphonic groups and indicates different phonatory mechanisms involved in vocal production, facilitating its monitoring during the therapeutic process(7-10).
Besides that, it also contributes to identify different types and degrees of voice deviation(8). Therefore, PDD can be considered
as an acoustic evaluation resource by offering complementary data to the isolated parameters traditionally used in voice clinic. Visual presentation associated with the different degrees of vocal deviation can be used to follow-up patients during voice rehabilitation. This tool can record the results of speech therapy in a clear and simple way, also allowing an easy understanding of the results, either for patients and therapist as for the health team involved in the process.
Therefore, the present study intended to verify if the PDD is capable of pointing out voice changes acquired during therapy and to analyze the correlation between auditory perceptual evaluation and the distribution of vocal samples in the diagram.
METHODS
This retrospective research was approved by the Ethical Committee of the Centro de Estudos da Voz (CEV), under the protocol number 1416/08. Thirty four pairs of vocal registers, pre and post therapy, from a clinical database were analyzed. Samples were collected from patients with voice complaints and with a deined dysphonia diagnosis, independently of type and degree of the deviation. Patients were of both gen-ders, being 13 women and 21 men, aging from 27 to 58 years (average of 49.02 years), randomly selected from those who sought and concluded clinical care during the year 2009.
All those patients, who required for treatment at the voice center, had already had ENT exams with hypothetical diagnosis deined and medical indication of voice therapy (functional dysphonia, minor structural changes, presbyphonia, Reinke’s edema, leukoplakia, granuloma, nodules, acute laryngitis, pa-resis, cordectomy, paralysis and postoperative benign lesions). Samples of patients who inished the proposed treatment with full records at the evaluation moment (pre therapy) and clinical discharge session (post therapy) were included in this study. Some characteristics of the treatment were not considered, such as number and duration of therapy sessions. However, all patients received a personalized treatment program based on techniques withscientiic evidence(11-15).Treatment outline was
directed to vocal hygiene, vocal psychodynamics and vocal training, with exercises done during sessions and at home(16).
The material used for analysis was the sustained vowel /ε/, in habitual frequency and intensity, recorded at two different moments: pre and post vocal therapy. Pre therapy moment constitutes the vocal evaluation session at the treatment onset, and post therapy moment is determined by the clinical discharge session. Samples were recorded and edited via VoxMetria 2,7 software (CTS Informatica), eliminating the irst second of emission, marked by natural instability, and analyzing the fol-lowing 3 seconds.
Voice registers were carried out in a silent environment, with patients sitting and using a unidirectional stand microphone,
speciic algorithm, WMC – Waveform Matching Coeficient
parameter, with normality value limit at 1); Glottal-to-Noise Excitation ratio (GNE — calculation of the noise in a series of
pulses, which indicates if the vocal signs are being generated by the vocal folds or by the turbulent airstream originated at the vocal tract, measured in dB, with normality value equal or higher than 0.5 dB).
Analyzes of voice samples’ coniguration distribution at PDD aimed to assess density, shape and place in quadrants. Density was classiied as concentrated ⎯ when all of the points were located inside of one square deined by the software; or as spread ⎯ if points were distributed into more than one square. Shape coniguration was classiied as horizontal, vertical or circular, regardless of density. Therefore, if the distance between points at coordinate X was longer than the distance between points at coordinate Y (X>Y), shape would be classiied as horizontal, if the distance between point at coordinate X was shorter than at coordinate Y (X<Y), it would be vertical; and if the distance between points in both coordinates were approximately the same (X≈Y), it would be classiied as circular (Figure 1). PDD was didactically split in four quadrants: inferior left – quadrant 1; inferior right – quadrant 2; superior right – quadrant 3; and superior left – quadrant 4(8) (Figure 2). Quadrant 1 corresponds
to the normality area proposed by the software.
Voices were presented in pairs, randomly, regarding pre and post vocal therapy condition. Ten percent of the samples were repeated to prove accuracy. The evaluation of the overall deviation degree was made by using a visual analogscale (VAS) of 100 points (parameter “G”, from CAPE-V(17)), considering:
from 0 to 35.5 points the normal variability of the vocal qual-ity (NVVQ); between 35.6 and 50.5 points mild to moderate degree; between 50.6 and 90.5 moderate degree; and above 90.6 severe deviation. Such values were based in previous studies performed with Brazilian voices(18), with results similar to those
found by the international study that proposed the scale (19).
Auditory perceptual evaluation was performed by a voice specialist, with 14 years of experience in this ield. The high reliability of the evaluator, for both pre-therapy (p=0.317) and post-therapy (p=0.414) samples evaluation, was veriied by the Wilcoxon Signed-Rank Test, with signiicance level of 5% (0.050).
Results were submitted to a statistical treatment (SPSS -
Statistical Package for Social Sciences, 13.0). Wilcoxon Signed-Rank Test application was adopted to verify possible differences between the two observation moments mentioned, for the variables of interest, such as, jitter, shimmer, Glottal-to-Noise Excitation (GNE) signal ratio and for the auditory perceptual analysis at pre and post therapy moments. For the comparison among density, shape and quadrants, pre and post therapy, Cramer’s V test was applied, and to analyze the relation between the diagram’s quadrants and the overall vocal devia-tion degree, the Chi-squared test was used. The signiicance level adopted was 5%.
Spearman’s correlation was used to measure the rela-tion among variables in pre and post vocal therapy groups. Spearman’s Rank Correlation is based on the ordination of two variables, with no restrictions regarding values distribution,
Noise (GNE)
5
4
3
2
1
A
Irregularity (Jitter, Shimmer, Correlation)
Phonat
or
y De
viation Diag
ram
0 1
0 2 3 4 5 6 7 8 9 10
Noise (GNE)
5
4
3
2
1
B
Irregularity (Jitter, Shimmer, Correlation)
Phonat
or
y De
viation Diag
ram
0 1
0 2 3 4 5 6 7 8 9 10
Subtitle 1. Examples of the distribution of vocal samples in the Phona-tory Deviation Diagram.
Legend: A = spread density and horizontal shape; B = spread density and vertical shape; C= concentrated density and circular shape.
Noise (GNE)
5
4
3
2
1
C
Irregularity (Jitter, Shimmer, Correlation)
Phonat
or
y De
viation Diag
ram
0 1
0 2 3 4 5 6 7 8 9 10
Subtitle 2. Didactical division of the Phonatory Deviation Diagram
Noise (GNE)
5
4
3
2
1
Irregularity (Jitter, Shimmer, Correlation)
Phonat
or
y De
viation Diag
ram
0 1
0 2 3 4 5 6 7 8 9 10
Left upper quadrant Right upper quadrant
Left lower quadrant Right lower quadrant
meaning that it is more applied for non-parametric data. A Correlation Matrix was produced by determining correlation signs (positive or negative) and their quality (quality≤20% = poor; 21 to 40%=low; 41 to 60%=fair; 61 to 80%=good;≥ 81%=ex-cellent). Only good or great correlations were chosen for analyzes. Correlation Test has validated the results, by testing the coeficient among variables.
RESULTS
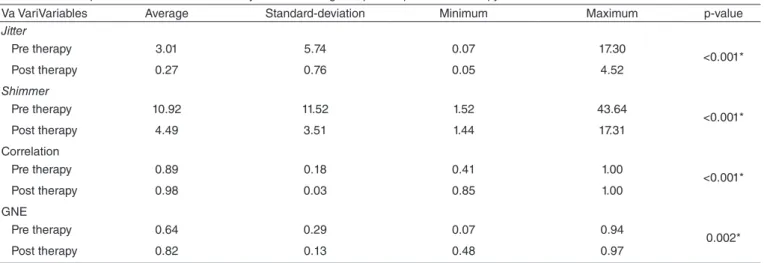
All the acoustic parameters studied presented differences at the pre and post therapy moments. Values obtained at the post therapy moment were closer to the normality levels established by the software (Table 1).
There was difference (p=0.031) in the coniguration between the two studied moments (Table 2). Horizontal shape was more frequent, either in pre and post therapy moments (61.76% and 58.82%, respectively). At the pre therapy, the vertical shape had the second higher frequency (35.26%) and there was only one occurrence of the circular shape. At the post therapy moment, vertical and circular shapes had the same frequency (20.59%). Therefore, there was a reduction of the vertical shape and an in-crease of the circular shape at the post therapy moment (Table 2). There was difference (p=0.019) in the placement of the vo-cal samples in the diagram in the studied moments (Table 3). At the pre vocal therapy, samples were distributed between quadrants 1 and 3 (64.71% and 29.41%, respectively), while at the post vocal therapy more than 90% of the samples were located at quadrant 1 (Figure 2).
There was an association between vocal deviation degree and the location of samples (p<0.001), in both studied mo-ments (Table 4). All voices with intense degree of deviation were placed in quadrant 3. Voices evaluated with mild and moderate degree of deviation were located in quadrant 1. Voices with moderate deviation presented a broad distribution, meaning that they were placed in quadrants 1, 2 and 3. These voices, at the post vocal therapy moment were divided between quadrants 1 and 2.
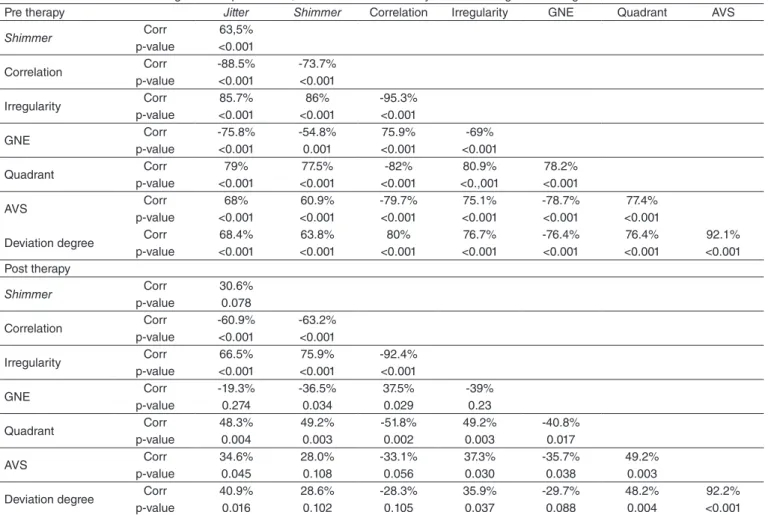
The correlation matrix between the acoustic parameters, PDD location and auditory perceptual analyzes was performed (Table 5). At the pre therapy moment, correlation value was between 61% and 80%, being considered good. At the post therapy moment, it was placed between 21% and 41%, being considered bad.
The average degrees of the vocal deviation, obtained by us-ing the VAS, at the pre and post therapy moments are presented at Figure 3. In the pre therapy, the average of vocal deviation of the studied group was 58.35 points in the VAS, being consid-ered a moderate degree; at the post vocal therapy, the average of vocal deviation was reduced to 40.38 points at the VAS, being considered mild to moderate degree. There was differ-ence between pre and post vocal therapy moments (p<0.001).
DISCUSSION
The Phonatory Deviation Diagram is a recent tool, and al-though not well explored, it is promising. It offers an acoustic analysis that is different from the previous ones, allowing the
Table 1. Acoustic parameters from the Phonatory Deviation Diagram, pre andpost vocal therapy
Va VariVariables Average Standard-deviation Minimum Maximum p-value
Jitter
Pre therapy 3.01 5.74 0.07 17.30
<0.001*
Post therapy 0.27 0.76 0.05 4.52
Shimmer
Pre therapy 10.92 11.52 1.52 43.64
<0.001*
Post therapy 4.49 3.51 1.44 17.31
Correlation
Pre therapy 0.89 0.18 0.41 1.00
<0.001*
Post therapy 0.98 0.03 0.85 1.00
GNE
Pre therapy 0.64 0.29 0.07 0.94
0.002*
Post therapy 0.82 0.13 0.48 0.97
* Significance level (p<0.050) – WilcoxonTest
Table 2. Phonatory Deviation Diagram shape, pre and post vocal therapy
Pre shape
Post shape
p-value
Circular Horizontal Vertical Total
n % n % n % n %
Circular 1 2.94 0 0 0 0 1 2.94
0,031*
Horizontal 3 8.82 16 47.06 2 5.88 21 61.76
Vertical 3 8.82 4 11.76 5 14.71 12 35.29
Total 7 20.59 20 58.82 7 20.59 34 100
extraction of acoustic parameters with a different algorithmic option(10,20,21), besides the combined analyzes of these parameters.
The most applied softwares for vocal acoustic assessment have strong limitations when used to analyze voices with higher degree of deviation, due to its own algorithmic option used to extract perturbation values(10,21). The algorithms proposed
by the authors of the PDD(7,9,10) are capable to analyze voice
samples with severe degrees of deviation, which are frequent at voice clinic.
More important than perform multiple evaluations with patients with vocal complaints is to understand how the results are related. The correlation among vocal behavior, acoustic and auditory perceptual analyzes facilitates the understanding of the anatomophysiologic mechanisms of the phonatory sys-tem presented by the patient and, consequently, it allows the elaboration of a more detailed and eficient therapy plan. PDD favors this combined analysis and suggests probable phonatory mechanisms used by the patient during voice production.
In literature, some studies try to correlate acoustic data with certain aspects of the auditory perceptual evaluation, but not always a straight correlationis established(7,9,10). It is possible
that a speciic dimension of the vocal quality has one or more acoustic clues for its perception, for the auditory evaluation is more comprehensive than acoustic analysis(22). A series of
experiments tried to determine what prompts would be involved in speciic dimensions of the vocal quality. Some acoustic characteristics of the vocal sign are common indings, such as fundamental frequency perturbation or noise, although these are related to voice production models and not its perception(5).
Therefore, the pursuit for vocal quality acoustic clues must go beyond the already proposed measures to quantify the vocal production aspects(5,7,20,21,23-25).
It was observed that the statistic report about acoustic data-provided by the software VoxMetria were different at the pre and post vocal therapy moments (Table 1). The average values of the acoustic parameters were within the expected range.
Table 3. Phonatory Deviation Diagramquadrants, pre and post vocal therapy
Pre Quadrant
Post Quadrant
p-value
1 2 3 4 Total
n % n % n % n % n %
1 22 64.71 0 0 0 0 0 0 22 64.71
0.019*
2 2 5.88 0 0 0 0 0 0 2 5.88
3 7 20.59 3 8.82 0 0 0 0 10 29.41
4 0 0 0 0 0 0 0 0 0 0
Total 31 91.18 3 8.82 0 0 0 0 34 100
* Significance level (p<0.050) – Chi-square test
Table 4. Relation among quadrants in the Phonatory Deviation Diagram and vocal deviation degrees, pre and post vocal therapy
Quadrante NVVQ Mild to moderate Moderate Severe Total p-value
n % n % n % n % n %
Pré
<0.001*
1 3 8.82 15 44.12 4 11.76 0 0 22 64.7
2 0 0 0 0 2 5.88 0 0 2 5.88
3 0 0 0 0 5 14.71 5 14.71 10 29.42
4 0 0 0 0 0 0 0 0 0 0
Total 3 8.82 15 44.12 11 32.35 5 14.71 34 100
Post
1 12 35.29 16 47.06 3 8.82 0 0 31 91.17
<0.001*
2 0 0 0 0 3 8.82 0 0 3 8.82
3 0 0 0 0 0 0 0 0 0 0
4 0 0 0 0 0 0 0 0 0 0
Total 12 35.29 16 47.06 6 17.64 0 0 34 100
* Significance level (p<0.050) – Wilcoxon test Legends: NVVQ = normal variability of vocal quality Legends: NVVQ = normal variability of vocal quality
Figure 3. Averages degrees of vocal deviation in auditory perceptual evaluation using VAS, pre and post therapy
* Significance level (p<0,001) – Wilcoxon test
Pre-vocal therapy Pos-vocal therapy 120
30.66
NVVQ 100
80
60
40
20
0
29.83 42.14
40.31 66.38
61.66 100
58.35 40.38
0 *
Mild t o moder
ate
Moder ate
A large part of the voice samples presented some deviation degree at the pre therapy moment. At the post therapy moment, however, samples were classiied as normal or near almost nor-mal. These data did not determine a direct association between dysphonia and any other isolated acoustic parameter(2,18,26).
Acoustic parameter values followed the improvement of vo-cal quality assessed by means of auditory perceptual analysis of the voice.
Regarding vocal samples distribution on the PDD, con-igurations were evaluated for density, shape and localization within the quadrants.Considering density coniguration, there was no difference between pre and post vocal therapy mo-ments. Despite the absence of statistical difference, a descrip-tive perspecdescrip-tive allows the observation of the increase in the concentrated density on the post therapy moment. Data from this research seem to corroborate the previous study indings (8),
which reported higher concentration of points in less altered voices. Such fact can be justiied by the reduced sample size, the variety of the selected cases, or by the degree of dysphonia, once more than half the voices presented normal variability of the vocal quality or mild or moderate deviation at the pre vocal therapy moment (Figure 3).
The change in distribution pattern of the voice samples dur-ing voice rehabilitation could be clearly observed. Horizontal
shape occurred more often independently of the moment. Circular shape was characteristic of the voices at the post vocal therapy moment, since it occurred only once at the pre therapy moment. When a balance between roughness and breathiness is achieved during phonation, this shape is expected. The vertical shape, less frequent in normal voices(25), occurred in a smaller
number at the post therapy. It is important to remember that even the vocal samples assessed at the post vocal therapy didn’t necessarily present normal voices. If it had happen, maybe the vocal distribution would be even lower, since such shape is characteristic of dysphonic voices.
Considering the voice samples localization in the quad-rants (Figure 2), at the pre vocal therapy moment it was ob-served that although most of them were located in quadrant 1 (inferior left), some samples were distributed in quadrant 2 (inferior right) and 3 (superior right) (Table 3). None of the samples were placed in quadrant 4 (superior left). This data corroborate literature and indicate that as the dysphonia degree decreases, voice sample plots tend to move to quadrant 1, where the normality area proposed by the software is located(8).
At the post vocal therapy moment, more than 90% of the studied samples were located in quadrant 1. The otherswere present in quadrant 2, and, as mentioned before, it should be considered that not all the patients presented normal voices at
Table 5. Correlation matrix among acoustic parameters, location at the Phonatory Deviation Diagram and degree of deviation
Spearman’ Correlation Test
Legends: GNE = glottal-to-noise excitation ratio VAS = visual analog scale
Pre therapy Jitter Shimmer Correlation Irregularity GNE Quadrant AVS
Shimmer Corr 63,5%
p-value <0.001
Correlation Corr -88.5% -73.7%
p-value <0.001 <0.001
Irregularity Corr 85.7% 86% -95.3%
p-value <0.001 <0.001 <0.001
GNE Corr -75.8% -54.8% 75.9% -69%
p-value <0.001 0.001 <0.001 <0.001
Quadrant Corr 79% 77.5% -82% 80.9% 78.2%
p-value <0.001 <0.001 <0.001 <0.,001 <0.001
AVS Corr 68% 60.9% -79.7% 75.1% -78.7% 77.4%
p-value <0.001 <0.001 <0.001 <0.001 <0.001 <0.001
Deviation degree Corr 68.4% 63.8% 80% 76.7% -76.4% 76.4% 92.1%
p-value <0.001 <0.001 <0.001 <0.001 <0.001 <0.001 <0.001
Post therapy
Shimmer Corr 30.6%
p-value 0.078
Correlation Corr -60.9% -63.2%
p-value <0.001 <0.001
Irregularity Corr 66.5% 75.9% -92.4%
p-value <0.001 <0.001 <0.001
GNE Corr -19.3% -36.5% 37.5% -39%
p-value 0.274 0.034 0.029 0.23
Quadrant Corr 48.3% 49.2% -51.8% 49.2% -40.8%
p-value 0.004 0.003 0.002 0.003 0.017
AVS Corr 34.6% 28.0% -33.1% 37.3% -35.7% 49.2%
p-value 0.045 0.108 0.056 0.030 0.038 0.003
Deviation degree Corr 40.9% 28.6% -28.3% 35.9% -29.7% 48.2% 92.2%
the voice therapy discharge, what might indicate therapeutic limitations. From the samples located in quadrant 3 at the pre vocal therapy moment, great part migrated to quadrant 1 and a small part to quadrant 2. The two voice samples placed in the quadrant 2 at the pre therapy moment migrated to quadrant 1. The dislocation of voice samples through the quadrants shows the therapy eficiency, with a reduction in the jitter, shimmer and correlation values, as well as the noise reduction, allowing a more appropriate phonatory adjustment within the phonation process.
Besides acoustic analysis, voices were also submitted to an auditory perceptualevaluation, using VAS(18). The
vo-cal deviation degree average was smaller at the post vovo-cal therapy moment (mild to moderate), and so, closer to normal variability of vocal quality (Figure 3). The average degree of vocal deviation at the pre therapy moment corresponded to a moderate deviation.
The association between voice samples’ localization in the PDD quadrants and the degree of vocal deviation (Table 4) was also assessed. At the pre and post vocal therapy moments, ac-cording to the correspondence of the degree of deviation of the VAS(18), voices that were evaluated within the normal variability
of the vocal quality range or yet with a mild to moderate devia-tion degree, were located in quadrant 1, the normality area(8).
There was a signiicant increase of voices evaluated within this quadrant, post-rehabilitation. Voices evaluated as pre-senting mild to moderate degree of deviation constituted the majority of the group, either in pre and post vocal therapy. At the post therapy moment voices previously classiied as moderate and severe were now classiied as mild degree, due to the improvement on vocal quality, as pointed out by the auditory perceptual analysis.
At the pre therapy moment, moderate voices were distrib-uted among quadrants 1, 2 and 3, and this fact deserves some consideration. First of all, it is noteworthy that localization is also inluenced by voice type(8), what was not considered in the
present study: Besides that, at VAS(18), the moderate deviation
degree band is the most extensive; voices closer to the lower limit, 50.5 points at VAS, were located in quadrants 1 and 2; those closer to the higher limit, 90.5 points, were located in quadrant 3. There was an important reduction of the group representing voices with moderate deviation at the post therapy moment, and these samples were divided between quadrants 1 and 2. None of the voices was evaluated as presenting severe degree of deviation at post vocal therapy moment. Auditory perceptual evaluation and dislocation of voices in the quadrants are evidences of vocal therapy eficiency.
The correlation matrix among acoustic parameters, PDD location and auditory analysis was also considered (Table 5). As expected, there was a positive correlation between the auditory perceptual analysis of the voices and the acoustic parameters obtained from the same audio signals either in pre and post therapy moments, which identiied speciic aspects of the evaluated voice. Values of this correlation were higher at the pre therapy, probably favored by larger deviations in such circumstance.
Acoustic and perceptual evaluations were important tools for the patients’ assessment and follow-up during the therapeu-tic process in the clinical practherapeu-tice, mainly as visual monitoring for the patient(7,9,10). Thus, the parameters analyzed indicated
the positive result of the vocal therapy, showing that the patient was capable of reorganizing the muscle adjustments during phonation, producing a better balanced voice after the vocal therapy(3,18,27,28).
There is some questioning in the literature regarding the use of acoustic analysis to extract parameters from voices with higher degrees of deviation. It is suggested that in these cases a descriptive qualitative spectrographic analysis should be performed(29,30). However, the PDD algorithmic option
al-lows the analysis of voices with higher deviation degrees while maintaining the reliability of the measures obtained(7,10,30).
More than identifying the vocal quality, it is important to quantify the magnitude of the quality(5). For monitoring therapy,
or even to quantify an improvement in vocal performance, PDD coniguration and auditory perceptual analysis can be used as complementary tools in the determination of acoustic parameters. During vocal quality monitoring, PDD does not induce contradictions in the interpretationof the obtained results, revealing itself as a useful and reliable instrument for clinical practice, especially for patient’s self-monitoring, who can visualize the therapeutic evolution through the dislocation of the voice on the diagram.
CONCLUSION
PDD is useful to identify changes with vocal rehabilitation and it correlates with the auditory perceptual analysis data.
* MB was the counselor and in charge of the research design, databank organization and correction of the text. GM was the co-counselor and responsible for the execution of the research and correction of the text. LRP was responsible for the research, data analysis and text.
REFERENCES
1. Takahashi H, Koike Y. Some perceptual dimensions and acoustical correlates of pathologic voices. Acta Otolaryngol. 1976;338: 2-22.
2. Carding PN, Steen IN, Webb A, Mackenzie K, Deary IJ, Wilson JA. The reliability and sensitivity to change of acoustic measures of voice quality. Clin Otolaryngol. 2004;29(5):538-44.
3. Oates,J. Auditory-perceptual evaluation of disordered voice quality: pros, cons and future directions. Folia Phoniatr Logop. 2009;61(1):49-56. 4. Behlau M, Madazio G, Feijó D, Pontes P. Avaliação de voz. In: Behlau
M, Voz: o livro do especialista. v.1. Rio de Janeiro: Revinter; 2001. p. 85-246.
5. Speyer R, Wieneke GH, Dejonckere PH. Documentation of progress in voice therapy: perceptual, acoustic, and laryngostroboscopic indings pretherapy and posttherapy. J Voice. 2004;18(3):325-40.
6. Patel S, Shrivastav R. Perception of dysphonic vocal quality: some thoughts and research update. Perspectives on Voice and Voice Disorders. 2007;17(2):3-6.
8. Madazio G, Leão S, Behlau M. The phonatory deviation diagram: a novel objective measurement of vocal function. Folia Phoniatr Logop. 2011;63(6):305-311.
9. Michaelis D, Gramss T, Strube HW. Glottal-to-noise excitation ratio – a new measure for describing pathological voices. Acta Acustica. 1997;83:700-6.
10. Fröhlich M, Michaelis D, Strube HW, Kruse E. Acoustic voice quality description: Case studies for different regions of the hoarseness diagram. In: Wittenberg T, Mergell P, Tigges M, Eysholdt U. (Eds). Advances in quantative laryngoscopy, 2 nd “Round Table”. Erlangen; 1997. p. 143-150. 11. Werth K, Voigt D, Döllinger M, Eysholdt U, Lohscheller J. Clinical
value of acoustic voice measures: a retrospective study. Eur Arch Otorhinolaryngol. 2010;267(8):1261-71.
12. Roy N, Weinrich B, Gray SD, Tanner K, Stemple JC, Sapienza CM. Three treatments for teachers with voice disorders: a randomized clinical trial. J Speech Lang Hear Res. 2003;46(3):670-88.
13. Lessac A. The use and training of the human voice: a Bio-Dynamic approach to vocal life. Mountain View, Mayield; 1997.
14. Roy N, Leeper HA. Effects of the manual laryngeal musculoskeletal tension reduction technique as a treatment for functional voice disorders: perceptual and acoustic measures. J Voice. 1993;7(3):242-9.
15. Roy N, Weinrich B, Gray SD, Tanner K, Stemple JC, Sapienza CM. Three treatments for teachers with voice disorders: a randomized clinical trial. J. Speech Lang Hear Res. 2003;46(3):670-88.
16. Behlau M, Madazio G, Feijó D, Azevedo R, Gielow I, Rehder MI. Aperfeiçoamento vocal e Tratamento fonoaudiológico das disfonias. In: Behlau M, organizador. Voz: o livro do especialista. v.2. Rio de Janeiro: Revinter; 2005. p. 409-528.
17. Behlau M. Consensus auditory – perceptual evaluation of voice (CAPE-V), ASHA 2003. Rev Soc Bras Fonoaudiol. 2004;9(3):187-9. 18. Yamasaki R, Leão S, Madazio G, Padovani M, Azevedo R, Behlau
M. Correspondência entre escala analógico-visual e escala numérica na avaliação perceptivo-auditiva de vozes. Rev Soc Bras Fonoaudiol. 2008;13(Suppl):1080.
19. Simberg S, Laine A, Sala E, Rönnemaa AM. Prevalence of voice disorders among future teachers. J Voice. 2000;14(2):231-5.
20. Eskenazi L, Childers DG, Hicks DM. Acoustic correlates of vocal quality. J Speech Lang Hear Res. 1990;33(2):298-306.
21. Madazio G, Leão S, Behlau M. Hoarseness diagram in voice predominantly rough, breath and strain. In: The Voice Foundation; 2006; Philadelphia. Abstract.
22. Titze I, Liang, H. Comparison of F0 extraction methods for high precision voice perturbation measurement. J Speech Hear Res 1993;36(6):1120-33
23. Kreiman J, Gerrat BR, Kempster GB, Erman A, Berke GS. Perceptual evaluation of voice quality: review, tutorial and a framework for future research. J Speech Lang Hear Res 1993;36(1):21-40.
24. Dejonckere PH. Principal components in voice pathology. J Voice. 1995;4:96-105.
25. Dejonckere PH, Lebacq J. Acoustic, perceptual, aerodynamic and anatomical correlations in voice pathology. ORL J Otorhinolaryngol Relat Spec. 1996;58(6):326-32.
26. Kreiman J, Gerrat B, Ito M. When and why listeners disagree in voice quality assessment tasks. J Acoust Soc Am. 2007;122(4): 2354-64.
27. Frölich M, Michaelis D, Strube HW. Acoustic breathiness measures in the description of pathological voices. In: Proceedings ICASSP 1998, Seattle, WA; 1998. p. 937-40.
28. Rabinov CR, Kreiman J, Gerrat BR, Bielamowicz S. Comparing reliability of perceptual ratings of roughness and acoustic measures of jitter. J Speech Lang Hear Res. 1995;38(1):26-32.
29. Bielamowicz S, Kreiman J, Gerratt BR, Dauer MS, Berke, GS. Comparison of voice analysis systems for perturbation measurement. J Speech Lang Hear Res. 1996;39(1):126-34.