HIV/AIDS in South Africa: an overview
HIV/AIDS na África do Sul: um panorama
1 Departm en t of Sociology, Un iversity of th e W itw atersran d ,
Joh an n esbu rg. Private Bag 3, W ITS, 2050, Sou th Africa. 029leah @m u se.w its.ac.z a 2 W its In stitu te for Social an d Econ om ic Research , Un iversity of th e W itw atersran d , Joh an n ersbu rg. Private Bag 3, W ITS, 2050, Sou th Africa. w alk er@w iser.w its.ac.z a Leah Gilbert 1 Liz Walk er 2
Abstract Th is p ap er p resen ts an overview of th e d evelop m en t of HIV/AIDS in Sou th Africa, tak -in g -in to con sid eration th e social con text an d an alyz-in g th e factors m ost lik ely to h ave -in flu en ced its sp read as w ell as th e societal resp on se to it. Th e au th ors argu e th at m acro factors su ch as so-cial an d p olitical stru ctu res, in ad d ition to beh avioral on es, h ave com bin ed to sh ap e th e cou rse of th e ep id em ic. Sin ce variou s factors lin k ed to social in equ alities h ave com bin ed to sh ap e th e p attern an d grow th of th e HIV/AIDS ep id em ic in Sou th Africa, it is in ap p rop riate to focu s on on ly on e d im en sion in an attem p t to com bat th e ep id em ic. Follow in g th e p sych osocio en v iron -m en t a l -m od el, a ll p ot en t ia l con t rib u t in g ele-m en t s n eed t o b e a d d ressed si-m u lt a n eou sly. Th is calls for a t ru e in t erd iscip lin ary an d m u lt isect orial ap p roach . It also requ ires great com m it -m en t as w ell as stron g p olitical w ill.
Key words H IV; Acq u ired Im m u n od eficien cy Syn d rom e; Disea se Ou t b rea k ; Socioecon om ic Factors; Ep id em iology
Resumo O artigo ap resen ta u m p an oram a d a ep id em ia d e HIV/AIDS n a África d o Su l, levan d o em con t a o con t ex t o social e an alisan d o os p rin cip ais fat ores qu e in flu en ciaram su a d issem i-n ação, assim com o, a resp osta p ela socied ad e su l-africai-n a. As au toras argu m ei-n tam qu e fatores m a cro, t a is com o est ru t u ra s socia is e p olít ica s, a lém d e fa t ores com p ort a m en t a is, a gira m em con ju n t o p a ra con figu ra r o cu rso d a ep id em ia . Um a v ez q u e v á rios fa t ores, a ssocia d os a d e-sigu ald ad es sociais, in flu en ciaram o p ad rão e o crescim en to d a ep id em ia d o HIV/AIDS n a África d o Su l, é in ap rop riad o focalizar ap en as u m a d im en são d a ep id em ia n a ten tativa d e com batê-la. Tod os os elem en tos qu e p ossam in flu en ciar o cu rso d a ep id em ia d evem ser abord ad os sim u lta-n eam elta-n te, d e acord o com o m od elo p sico-sócio-am bielta-n tal. Tal abord agem d eve ser verd ad eira-m en t e in t erd iscip lin a r e eira-m u lt i-set oria l, o qu e t a eira-m béeira-m requ er gra n d e coeira-m p roeira-m isso e von t a d e p olítica.
Introduction
“Sou th Africa h as th e fastest grow in g [HIV/AIDS] ep id em ic of an y cou n try in th e w orld . W ith in five years, on e Sou th African w ill d ie of an AIDS-related illn ess every m in u te u n less action is tak en n ow ”(Lowe ll, 2000:1). Th is is b u t o n e of m a n y recen t sta tem en ts in th e Sou th Africa n m e d ia wh ic h c a p t u re s t h e gra vit y o f t h e e p i-d e m ic, its p o te n tia l im p a ct o n so cie ty, a n i-d th e u rge n t n e e d fo r e ffe ct ive in t e r ve n t io n s. H igh p ro file m e d ia cove ra ge is a re la tive ly n e w p h e n o m e n o n in So u t h Afr ica : o n e o f t h e e p id e m -ic’s m a in fea tu res sin ce th e b egin n in g h a s b een sile n c e. Alt h o u gh H IV/ AID S fe a t u re s p ro m i-n e i-n t ly ii-n t h e m e d ia a i-n d is fie rce ly d e b a t e d ii-n gove r n m e n t a l a n d n o n gove r n m e n t a l c irc le s, th e ep id em ic con tin u es to grow ra p id ly, a n d ef-fo rts to co m b a t it h a ve n o t yie ld e d th e e xp e ct-ed resu lts.
HIV/ AIDS is n o t m erely a m ed ica l p ro b lem , b u t p rim a rily a so cia l o n e, a s d e m o n stra te d b y its sp rea d a s well a s b y th e in a b ility a n d in a d e-q u a cy o f t h e m e d ica l e st a b lish m e n t t o co n t ro l a n d cu r t a il it s e xp a n sio n . Th is u n d e rst a n d in g is in lin e with th e p sych o -so cio -en viro n m en ta l (PSE) m o d e l o f h e a lt h a n d d ise a se, in sh a r p con trast to th e b io-m ed ical m od el, wh ich views h e a lt h a n d d ise a se “t h ro u gh t h e m ic ro sc o p e” an d offers tech n ical solu tion s to wh at are la rge-ly so cia l p ro b le m s. Ra th e r th a n ke e p in g h e a lth a n d d ise a se in a b io lo gic a l c o n t e xt , t h e PSE m o d el a n a lyzes th em in a so cia l co n text wh ich t a ke s a m a cro sco p ic vie w a n d o ffe rs a b ro a d e r p ersp ective. Th e m o d el fo cu ses o n th e p ro m o tio n a n d m a in ten a n ce o f h ea lth th ro u gh so cio -en viro n m -en ta l a n d b eh a vio ra l ch a n ge (Gilb ert et a l., 1996). Th is p a p er p resen ts a n overview of th e H IV/ AIDS ep id em ic in So u th Africa , ta kin g t h e so cia l co n t e xt in t o co n sid e ra t io n a n d a n a lyzin g t h e fa c t o r s m o st like ly t o h a ve in flu -en ced b oth th e ep id em ic’s sp rea d a n d th e soci-e t a l rsoci-e sp o n ssoci-e t o it . It is a rgu soci-e d t h a t m a cro fa c-t o r s su c h a s so c ia l a n d p o lic-t ic a l sc-t r u c c-t u re s a s well as b eh avioral on es h ave com b in ed to sh a p e th e cou rse of th e ep id em ic a n d its ou tcom e.
Methodological concerns
On e of th e m a in p rob lem s in Sou th Africa is th e in a d e q u a t e q u a lit y o f st a t ist ic a l in fo r m a t io n . All d a ta m u st th u s b e in terp reted ca refu lly, recogn izin g p oten tia l in a ccu ra cies, m a in ly in p op u la t io n e st im a t e s a n d re gist ra t io n o f in fo r m a -t io n . Th e ge n e ra l d a -t a p re se n -t e d in -t h is p a p e r a re d e rive d fro m five d iffe re n t so u rce s: He a lt h System s Tru st, Dep a rtm en t o f Hea lth , Sta tistics
So u th Africa , UNISA’s Ma rket Resea rch Bu rea u , a n d Co m m u n it y Age n c y fo r So c ia l In q u ir y (CASE).
Socioeconomic and demographic
characteristics of South African society
So u th Africa n so ciety is m a rked b y gro ss so cia l in e q u a lit ie s, m a n ife st in g t h e m se lve s m a in ly a lo n g ra c ia l, c la ss, a n d ge n d e r lin e s. It is a r -gu a b le t h a t ra c ia l in e q u it ie s (in t h e fo r m o f a p a r t h e id ) h a ve m o st sign ifica n t ly sh a p e d t h e so c ia l p ro file a n d c o n se q u e n t ly h e a lt h a n d h e a lth ca re o f So u th Africa . Un d e r th e Po p u la -tio n Registra -tio n Act o f 1950, a ll So u th Africa n s we re c la ssifie d in t o a “p o p u la t io n gro u p” a t b ir t h a n d a ssign e d a ra c ia l c a t e go r y, n a m e ly Wh ite, In d ia n , Colou red , a n d Africa n . Alth ou gh t h is a c t wa s re p e a le d in 1991, it s so c ia l a n d eco n o m ic effects will rem a in p resen t fo r a lo n g tim e to co m e. Th erefo re sta tistics in th is p a p er will b e p re se n t e d a c c o rd in g t o “p o p u la t io n grou p s” or ra ce wh ere a p p rop ria te.
In 1999, 10.5% o f th e So u th Africa n p o p u la -t io n we re Wh i-t e, 2.5% In d ia n , 8.8% Co lo u re d , a n d 77.2% Africa n . Th e n a tio n a l a vera ge a n n u -a l growth a te fo r 1991-1996 w-a s 2.0% -a n d v-a r-ie d fro m 0.5% fo r Wh it e s t o 2.4% fo r Afr ica n s. Th e Afr ica n p o p u la t io n is yo u n g a n d e xp a n d -in g, with over 25% o f th e p o p u la tio n b elow th e a ge o f 15 ye a rs. In co n t ra st , t h e Wh it e p o p u la -t io n is a gin g a n d sh r in kin g, wi-t h a s m u c h a s 9.4% o f t h e p o p u la t io n a ge d 65 ye a rs o r o ld e r. Th e p e rc e n t a ge o f t h e p o p u la t io n in t h e e c o -n o m ica lly a ctive a ge b ra ckets is sm a ller fo r th e Afr ic a n a n d Co lo u re d t h a n fo r t h e Wh it e a n d In d ian grou p s. Th e in fan t m ortality rate is h igh e st fo r t h e Afr ic a n p o p u la t io n (48 p e r t h o u -sa n d ) a n d lowe st fo r Wh it e s (7 p e r t h o u -sa n d ). Me a n n a t io n a l life e xp e c t a n c y a t b ir t h is 62 ye a rs fo r m e n a n d 68 fo r wo m e n . Howe ve r, life e xp e cta n cy ra n ge s fro m 59 fo r Co lo u re d m a le s to 76 for Wh ite fem a les (HST, 2000:405).
co u n t r ie s o f sim ila r st a t u s. In 1991, Wh it e p e r ca p ita in co m e s we re m o re th a n 12 tim e s th o se o f Africa n s. However, in co m e in eq u a lity with in p op u la tion grou p s h a s grown even fa ster a n d is gre a t e st a m o n g Afr ic a n s, wh e re t h e p o o re st 40% e a r n e d o n ly 6.4% o f t h e in c o m e a n d t h e rich e st 10% e a rn e d 46.6% in 1991. Du rin g t h a t sa m e ye a r it wa s e st im a t e d t h a t 17.3 m illio n p e o p le a n d a b o u t h a lf o f a ll h o u se h o ld s live d b e low t h e m in im u m su b sist e n c e le ve l. Two -th ird s o f Africa n h o u seh o ld s were estim a ted to live in p ove r t y, c o m p a re d t o 6.7% o f Wh it e h ou seh old s. Th ese figu res rem a in ed la rgely u n -ch a n ged in 2001.
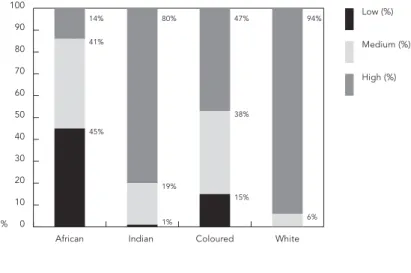
Alt h o u gh t h is p a p e r d o e s n o t e xp lo re t h e com p lexities of class an d its relation sh ip to race, for p u rp oses of an alytical clarity in com e is u sed as an in d icator for class (Gilb ert & Walker, 2000). Figu re 1 is a cle a r d e m o n st ra t io n o f t h e re -la tio n sh ip b etween c-la ss a n d ra ce in th e So u th Africa n con text.
Em p loym e n t in t h e fo r m a l se ct o r is a n im -p o r t a n t gu a ra n t e e o f in c o m e, a d e q u a t e fo o d , a n d a cce ss to o th e r n e ce ssa r y se r vice s. Un e m -p loym e n t in t h e fo r m a l se c t o r n ow st a n d s a t a b o u t 40% o f t h e wo rk fo rc e. Ap a r t h e id p o li-cie s, t o ge t h e r wit h a gr icu lt u ra l p o lili-cie s fa vo r-in g la rge -sca le a gr icu lt u re, p u sh e d m illio n s o f Afr ic a n s o ff t h e ir la n d in t o im p ove r ish e d re -se r ve s, h o m e la n d s, a n d t own sh ip s. At p re -se n t th e Wh ite agricu ltu ral sector own s 88% of a ra b le la n d in So u t h Afr ic a . H ist o r ic a lly, t h e So u t h Africa n e co n o m y wa s stru ctu re d a ro u n d a system of m igran t lab or wh ich sp an n ed th e Sou th -e r n Afr ic a n r-e gio n , l-e a d in g yo u n g m -e n a n d wo m e n t o le a ve t h e r u ra l a re a s t o fin d wo rk in t h e m in e s a n d c it ie s. Ra p id a n d u n c o n t ro lle d u rb a n iza t io n in t h e Afr ica n p o p u la t io n re su lt -e d in fa m ily b r-e a kd own , h igh l-e v-e ls o f u r b a n a n d r u ra l p ove r t y, a n d t h e ra m p a n t sp re a d o f d ise a se s a sso cia t e d wit h im p ove r ish m e n t a n d p op u la tion m ob ility (Ma rks & Tra p id o, 1987).
Sin ce ed u ca tio n is reco gn ized wo rld wid e a s a p rereq u isite for su sta in a b le d evelop m en t a n d h e a lt h , it a lso p la ys a n im p o r t a n t ro le in so ci-e t y’s rci-e sp o n sci-e t o t h ci-e H IV/ AID S ci-e p id ci-e m ic. In So u th Africa , ra cia l im b a la n ce s e xist in e d u ca -t io n o n e ve r y le ve l, wi-t h Afr ic a n p e o p le m o s-t se ve re ly a ffe c t e d . Th e la t e st Na t io n a l Ho u se -h o ld Su r ve y o f He a lt -h In e q u a lit ie s in So u t -h Afr ica (CASE, 1995) re p o r t e d t h a t 92% o f p e r -so n s re sp o n sib le fo r h o u se h o ld h e a lt h c a re we re wo m e n . Am o n g Afr ic a n s, 57% h a d a t t a in e d st a n d a rd five e d u c a t io n o r le ss, c o m -p a red with 50% a m o n g Co lo u red s, 22% a m o n g In d ia n s, a n d 1% a m o n g Wh it e s. Ur b a n iza t io n h a s b e e n a n im p o r t a n t fa c t o r in d e t e r m in in g b o t h t h e p o p u la t io n’s h e a lt h a n d it s d ise a se
p a t t e r n s. By 1985, a b o u t 57% o f t h e So u t h Africa n p o p u la tio n wa s u rb a n ize d a n d lo ca te d m a in ly in t h e m a jo r m e t ro p o lit a n a re a s. Th e c o u n t r y’s u r b a n p o p u la t io n is p re d ic t e d t o d o u b le by th e yea r 2010, crea tin g a n en o rm o u s ch a lle n ge fo r p la n n e rs o f h e a lt h , h o u sin g, a n d o t h e r so c ia l se r vic e s. Ac c o rd in g t o t h e 1991 c e n su s, 9% o f t h e p o p u la t io n live d in u r b a n sh a n tytown s, with in a d eq u a te p rovisio n o f b a -sic fa cilities su ch a s sa fe wa ter, sa n ita tion , elec-tricity, a n d h ea lth services.
Th e in eq u a lities id en tified in So u th Africa n so ciety a re reflected in th e h ea lth secto r. Nea r-ly t h re e -fift h s (58%) o f t h e t o t a l h e a lt h b u d ge t wa s sp e n t o n p r iva t e h e a lt h se r vic e s wh ic h se r ve a p p ro xim a t e ly 20% o f t h e p o p u la t io n , m o st ly Wh it e a n d t h o se fro m t h e h igh e r in -com e grou p s. Th e resu lt is fewer h ea lth ca re re-so u rc e s fo r p o o re r p e o p le. Co u p le d wit h t h e p oor livin g con d ition s d escrib ed ea rlier, th is a l-so m e a n s le ss a va ila b le h e a lt h ca re fo r p e o p le wit h h igh e r in fa n t m o r t a lit y ra t e s a n d ge n e ra l m orb id ity levels.
Th e Na t io n a l Ho u se h o ld Su r ve y o f He a lt h In e q u a lit ie s in So u t h Afr ic a (CASE, 1995) re -vea led a ra n ge of in eq u a lities a lon g ra cia l lin es. Of p a rticu la r re le va n ce to th is p a p e r is th e d if-feren tia l a ccess to h ea lth ca re by ra ce, wh ereby a la rge r p ro p o r t io n o f Afr ic a n s (37%) a n d Co lo u re d s (30%) h a d n o t re ce ive d h e a lt h ca re in t h e p re vio u s ye a r a s c o m p a re d t o Wh it e s (17%) a n d In d ia n s (18%). Th e se fin d in gs a lso su p p o r t t h e n o t io n t h a t t h o se m o st in n e e d o f
Figure 1
Socioeconomic status by race. South Africa.
Source: Health Systems Trust, The Equity Gauge, 2000. 0
% 10 20 30 40 50 60 70 80 90 100
Low (%)
Medium (%)
High (%)
White Coloured
Indian African
6% 94%
15% 38% 47%
1% 19% 80%
h ea lth ca re d o n ot n ecessa rily h a ve a ccess to it. Da ta from th is su rvey a lso in d ica te th a t, in gen -e ra l, p ov-e r t y, ov-e rc rowd in g, a n d u n -e m p loy-m e n t a re a sso c ia t e d wit h la c k o f h e a lt h c a re, p a rticu la rly a m on g Africa n s a n d Colou red s.
Alt h o u gh c la ss/ ra c ia l in e q u a lit ie s ove r -sh a d ow o t h e r t yp e s o f in e q u a lit ie s, o f sp e cific re le va n ce to th is p a p e r a re ge n d e r in e q u a litie s p reva len t in So u th Africa . It is a rgu ed th a t gen -d e r re la t io n s in ge n e ra l, a n -d in So u t h Africa in p a rticu la r, op era te m a in ly to p rivilege m en a n d to su b ord in a te wom en . Gen d er d ifferen ces a n d in eq u a lities in Sou th Africa ca n b e d em on stra t-ed a t va riou s levels, som e of wh ich a re em p loym e n t, co n tro l ove r re p ro d u ctio n , th e la w, e d u -ca t io n , a n d se xu a lit y (Gilb e r t & Wa lke r, 2000). Un e m p loym e n t ra t e s a re h igh e r fo r wo m e n t h a n m e n in a ll ra cia l ca t e go r ie s. In 1995, 47% of econ om ica lly a ctive Africa n wom en a n d 29% of Africa n m en were u n em p loyed , com p a red to on ly 4% of Wh ite m en a n d 8% of Wh ite wom en . On a ve ra ge, wo m e n e a r n b e t we e n 72 a n d 85% o f wh a t m e n wit h sim ila r e d u c a t io n e a r n a n d c o n t in u e t o p re d o m in a t e in low- skille d a n d low- p a id o ccu p a t io n s. Afr ica n wo m e n a re t h e p o o re st, m o st e co n o m ica lly m a rgin a lize d , a n d lea st ed u ca ted secto r o f th e So u th Africa n p o p -u la tio n , th -u s p la cin g th em a t th e b o tto m o f th e h e a lt h p ile in t h is c o u n t r y (Gilb e r t & Wa lke r, 2000; Gilgen et a l, 2000; Su sser & Stein , 2000).
Th is b rief over view o f th e So u th Africa n so -cia l co n t e xt h a s se r ve d t o p rovid e in sigh t in t o
th e h istorica l p rogression a s well a s th e cu rren t sta te of HIV/ AIDS in Sou th Africa .
History of the HIV/AIDS epidemic
Th e fir st AID S c a se s re p o r t e d in So u t h Afr ic a o ccu rred a m o n g h o m o sexu a l m en in 1982. Pri-o r t Pri-o t h e d e ve lPri-o p m e n t Pri-o f H IV a n t ib Pri-o d y t e st s, a b o u t 100 b lo o d tra n sfu sio n -rela ted in fectio n s a re kn own to h a ve o ccu rre d b e twe e n 1982 a n d 1985. HIV testin g of stored sera from a com m u -n it y su r ve y i-n r u ra l Kwa Zu lu - Na t a l a -n d b lo o d d o n o r d a t a d e m o n st ra t e d a ve r y low p re va -le n ce o f H IV in t h e ge n e ra l p o p u la t io n in 1985 (Ab d ool-Ka rim , 2000).
Figu re 2 d e p ict s t h e n u m b e r o f AIDS ca se s in So u t h Afr ica b y ye a r o f d ia gn o sis a n d e xp o su re ca t e go r y. Th e se d a t a a re d e r ive d fro m in -fo rm a t io n re le a se d b y t h e t h e n De p a rt m e n t o f Na t io n a l He a lt h a n d Po p u la t io n De ve lo p m e n t b a se d o n a n o n ym o u s d a t a su p p lie d b y t h e So u t h Afr ic a n In st it u t e o f Me d ic a l Re se a rc h (SAIMR), as well as Ep id em iological Com m en ts. Th is figu re re p re se n t s t h e AID S e p id e m ic b e -t we e n 1982- 1992 a cco rd in g -t o m o d e o f -t ra n s-m ission .
Th is p a in t s a c le a r p ic t u re wit h re ga rd t o t h e e a r ly p a t t e r n o f t h e e p id e m ic. Like t h e d o m in a n t p a tte rn s in We ste rn co u n trie s in th e ea rly to m id -1980s, th e ep id em ic wa s co n fin ed m a in ly t o h o m o se xu a l m a le s a n d a s o f 1988
Figure 2
AIDS cases by pattern of transmission per year. South Africa, 1986-1992.
Source: Information released by the Department of National Health and Population Development, based on anonymous data supplied by the South African Institute of Medical Research.
0
number of cases
50 100 150 200 250 300 350 400
Homo/Bisexual
Heterosexual, Paediatric, Haemophiliac, Transfusion
1992 1991
1990 1989
1988 1987
(wit h in t h is e xp o su re c a t e go r y) se e m e d t o b e u n d er ch eck (Ijsselm u id en et a l., 1988).
Ba sed o n Figu re 2 it ca n b e a rgu ed th a t th is e a rly p a tte rn wa s so o n to ch a n ge, a s in d ica te d b o t h b y t h e d a t a a s we ll a s t h ro u gh a n u n d e r stan d in g of th e u n iq u e Sou th African social con -d ition s an -d con text -d iscu sse-d ab ove. By th e late 1980s it wa s a lre a d y q u it e o b vio u s t h a t t h e fu -tu re growth of th e ep id em ic wou ld m ain ly affect th e h eterosexu al p op u lation an d wou ld b e com -p ou n d ed by -p ed iatric AIDS, as a con seq u en ce of th e in volvem en t of wom en of ch ild -b earin g age. Howe ve r, u n like t h e p a t t e r n in We st e r n cou n tries, a lth ou gh recrea tion a l d ru g u se is ex-t e n sive, in je c ex-t in g d r u g u se h a s b e e n lim iex-t e d , a n d n e e d le sh a r in g d o e s n o t a p p e a r t o b e a ve r y im p o r t a n t m o d e o f H IV t ra n sm issio n in So u t h Afr ica , wit h se xu a l in t e rco u rse re m a in -in g a s th e m a -in m od e (Ab d ool-Ka rim , 2000).
HIV-1 is th e d om in an t strain in Sou th Africa , wit h H IV- 2 re m a in in g ra re. H IV- 1 m o le c u la r ep id em io lo gy h a s d em o n stra ted th a t th e cla d e B viru s p red om in a tes a m on g ga y m en , a n d th a t cla d e C is a sso cia t e d wit h h e t e ro se xu a l t ra n s-m issio n . Acco rd in g to Ab d o o l-Ka ris-m (2000:11), t h e se fin d in gs “su ggest tw o in d ep en d en t HIV ep id em ics u n fold in g in Sou th Africa; th e first an d earlier ep id em ic started in th e early 1980s in w h ich HIV h as sp read m ain ly th rou gh sam e sex con tact an d con tam in ated factor VIII, w h ile th e secon d an d m ost recen t ep id em ic started in abou t 1987 am on g h eterosex u als, w ith a con
-com itan t ep id em ic am on g ch ild ren in fected th rou gh perin atal tran sm ission”.
In 1990 t h e D e p a r t m e n t o f He a lt h b e ga n testin g p regn an t wom en atten d in g p u b lic h ea lth secto r p ren a ta l clin ics; th u s th e H IV/ AIDS d a ta fro m 1991 o n wa rd s h a ve b e e n o b t a in e d fro m th e n a tio n a l a n n u a l su r ve y. Th e se d a ta a re n o t fa u lt le ss, b u t a re t h e o n ly st a t ist ic a l m a t e r ia l a va ila b le o n a n a t io n a l le ve l. Th e re a re a rgu -m en ts to su ggest b o th a n u n d er- a n d over-esti-m a t io n o f t h e t r u e size o f t h e e p id e over-esti-m ic fro over-esti-m t h e se d a t a . Am o n g se xu a lly a c t ive a d u lt s, t h e p re n a t a l su r ve y p re va le n c e figu re s d o n o t re -fle ct t h e lowe r ove ra ll risk o f m e n , p e o p le wh o a re less sexu a lly a ctive, a n d com m u n ities u sin g t h e p r iva t e se c t o r. On t h e o t h e r h a n d , re c e n t stu d ie s in d ica te th a t fe rtility a m o n g H IV-p o si-t ive wo m e n is su b ssi-t a n si-t ia lly lowe r si-t h a n a m o n g u n in fe c t e d wo m e n , su gge st in g t h a t p re n a t a l d a ta m a y in fa ct u n d erestim a te HIV p reva len ce in re p ro d u ct ive a ge wo m e n in m a n y co m m u -n ities. O-n b a la -n ce, h owever, it is felt th a t th ese p re n a ta l d a ta a re su fficie n t fo r p u rp o se s o f e s-t im a s-t in g cu rre n s-t in fe cs-t io n ra s-t e s in s-t h e ge n e ra l p o p u la t io n a n d p ro je ct io n s o f t h e se ra t e s in t o th e fu tu re (ABT Associates In corp oration , 2000). Th e d a t a co lle ct e d in t h e se a n n u a l su r ve ys a re su m m a r ize d in Figu re 3, c le a r ly sh owin g t h e ra p id growt h o f t h e e p id e m ic in So u t h Africa a s a wh ole.
Du e to th e so cio lo gica l sign ifica n ce o f ra ce in So u t h Afr ica , it is im p o r t a n t t o e xa m in e t h e
Figure 3
HIV prevalence trends. South Africa, 1990-1999.
Source: Department of Health, 2000. 0
HIV pr
evalence (%)
5 10 15 20 25
1999 22.4
1998 22.8
1997 17.04
1996 14.17
1995 10.44
1994 7.57
1993 4.01
1992 2.15
1991 1.74
a va ila b le H IV/ AIDS figu re s a cco rd in g t o t h e se ca t e go r ie s. No t e sh o u ld b e t a ke n t h a t p r io r t o 1994 a ll sta tistics in Sou th Africa were collected a n d p re se n t e d b y “p o p u la t io n gro u p”, a s d is-cu ssed ea rlier.
Figu re 4 is a n e xa m p le o f AID S c a se s p re -sen ted a ccord in g to ra cia l ca tegories a n d clea r-ly illu stra tes h ow with th e sh ift o f th e ep id em ic fro m t h e m a in ly h o m o se xu a l p a t t e r n t o t h e h e t e ro se xu a l o n e, b o t h t h e p e rce n t a ge a n d ra -tio of in fected Africa n p eop le h a ve in crea sed a s p re d ict e d . Sin ce 1994 t h e ca t e go r y o f “ra ce” o r “p o p u la t io n gro u p” h a s b e e n e xc lu d e d fro m th e d a ta collected . However, its socia l im p a ct is e vid e n t , a lt h o u gh ca m o u fla ge d , in o t h e r ca t e -go rie s su ch a s ge o gra p h ic lo ca tio n (p rovin ce s) a n d / or cla ss (in com e grou p s).
Current state of the epidemic
Fo llowin g t h e n e w p o lit ic a l d isp e n sa t io n (1994), So u th Africa h a s b een d ivid ed in to n in e p rovin c e s wit h t h e a im o f re d re ssin g so m e o f t h e p a st in e q u a lit ie s a n d fa cilit a t in g sm o t h e r a d m in ist ra t io n a n d gove r n a n ce. Howe ve r, t h e rea lity is th a t th ere a re strikin g in eq u a lities b e-tween th e p rovin ces on va riou s levels.
Exa m in in g t h e la t e st H IV p re va le n c e d a t a by p rovin ces, Figu re 5 revea ls a d ifferen tia l d is-t r ib u is-t io n o f is-t h e b u rd e n o f H IV/ AID S b e is-t we e n t h e p rovin ce s, wit h Kwa Zu lu Na t a l h a vin g t h e
h igh est rates (32.5%) followed by Free State with 27.9%. It can b e argu ed th at th ese d ifferen ces are m ost likely in flu en ced by th e social factors wh ich facilitate an d exp ed ite th e sp read of th e d isease. Ra c ia l c o m p o sit io n (p o p u la t io n gro u p ) va ries grea tly b etween th e p rovin ces (Figu re 6). Th is is o f p a r t ic u la r sign ific a n c e in t h e So u t h Afr ica n co n t e xt d u e t o t h e co n flu e n ce o f cla ss a n d ra c e, in p a r t b e c a u se o f t h e le ga c y o f a p a r t h e id . It a c q u ire s a d d it io n a l sign ific a n c e o n ce exa m in ed in co m b in a tio n with so cio eco -n om ic sta tu s by ra ce (Figu re 1).
So cio eco n o m ic sta tu s is a go o d in d ica to r o f b u rd en of d isea se. Th e lower th e socioecon om -ic sta tu s o f a co m m u n ity th e m o re likely it is to b e u n h e a lt h y. D a t a in Figu re 1 m a n ife st t h e gro ss d isp a rities b etween ra cia l gro u p s, wh ere-b y 94% o f t h e Wh it e p o p u la t io n , in co n t ra st t o o n ly 14% o f th e Africa n p o p u la tio n , h a s a h igh so cio eco n o m ic sta tu s. Th e u n em p loym en t ra te a t t h e t im e o f t h e 1996 p o p u la t io n ce n su s wa s 34%. An a n a lysis o f u n e m p loym e n t ra t e s b y p rovin ces (Sta tistics So u th Africa , 2000) id en ti-fies fo u r with h igh er u n em p loym en t ra tes th a n t h e c o u n t r y a s a wh o le : Ea st e r n Ca p e (49%), North ern Provin ce (46%), KwaZu lu -Natal (39%), a n d No r t h We st (38%). Th e se a re a lso t h e p rovin ce s wit h t h e lowe st le ve ls o f d isp o sa b le in c o m e p e r c a p it a (U N ISA, 2000). Alt h o u gh th ese d a ta were d erived fro m d ifferen t so u rces, t h e y cle a rly a t t e st t o t h e e xist e n ce o f in e q u a li-ties b etween th e p rovin ces.
Figure 4
Transmission category by race and year of diagnosis. South Africa.
Source: Information released by the Department of National Health and Population Development, based on anonymous data supplied by the South African Institute of Medical Research.
0
number of transmissions
50 100 150 200 250 300
White homo/bisexual
White heterosexual
Black homo/bisexual
Black heterosexual
1991 1990
1989 1988
Figure 5
HIV prevalence by province. South Africa, 1999.
Source: Department of Health, 2000. 0
HIV pr
evalence (%) 5
10 15 20 25 30 35
Western Cape 7.1
Northern Cape
10.1
Northern Province
11.4
Eastern Cape 18.0
Gauteng 22.5
North West 23.0
Mpumalanga 23.8
Free State 27.9
Kwazulu-Natal 32.5
Figure 6
Population group by province. South Africa, 1996.
Source: Statistics South Africa, 2000.
0 1,000,000 2,000,000 3,000,000 4,000,000 5,000,000 6,000,000 7,000,000 8,000,000 9,000,000
Unspecified/ Other
White
Indian
Coloured
African
Western Cape Northern
Cape Gauteng Kwazulu-Natal Free State
Eastern Cape Mpumalanga North West
Th e la test rep o rt b y th e Un iversity o f So u th Afr ic a’s Bu re a u o f Ma rke t Re se a rc h (U N ISA, 2000) co n clu d e s t h a t So u t h Afr ica n in e q u a lit y rem a in s a m o n gst th e h igh est in th e wo rld , giv-in g th e co u n tr y th e sta tu s o f o n e o f th e wo rld ’s m o st u n e q u a l so c ie t ie s (Ka t ze n e lle n b o ge n , 2000). Th e re p o r t p o in t s t o o n e o f t h e m o st vivid in d ic a t io n s o f So u t h Afr ic a n in e q u a lit y: th e sh a rp ly d ifferin g levels of th e h u m a n d evel-o p m e n t in d e x fevel-o r th e va rievel-o u s p revel-ovin ce s. Ga u t-e n g (So u t h Afr ic a’s t-e c o n o m ic h u b ) a n d t h t-e We st e r n Ca p e h a ve t h e sa m e ra n kin g in t e r m s of th e h u m a n d evelop m en t in d ex, a t 0.73, sim i-la r to a m id d le -in co m e co u n tr y like Tu rke y. By co n tra st, th e No rth ern Provin ce, th e p o o rest in So u th Africa , h a s a h u m a n d e ve lo p m e n t in d e x o f 0.57, clo se to th a t o f Zim b a bwe, wh ich ra n ks 130t h in t h e in d e x. Ove ra ll, So u t h Afr ica h a s a h u m a n d e ve lo p m e n t in d e x o f 0.67, m e a n in g th a t it is fa r sh ort of th e 0.8 th a t th e UNDP con -sid ered n ecessa ry for a h igh level of h u m a n d e-velop m en t (Ka tzen ellen b ogen , 2000).
Yo u n ge r p e o p le a re t h e m o st se ve re ly a f-fe c t e d b y H IV/ AID S. Th is is n o t su r p r isin g, sin ce a b o u t 45% o f t h e So u t h Afr ica n p o p u la -tio n (16 m illio n ) a re u n d e r 20 ye a rs o f a ge. It is e st im a t e d t h a t ove r 60% o f a ll n e w in fe c t io n s cu rren tly o ccu r a m o n g in d ivid u a ls b etween 15 a n d 25 ye a rs o f a ge, wit h wo m e n ge n e ra lly b e -in g -in fe c t e d e a r lie r t h a n m e n (Figu re 7). Th e ove ra ll ra t e is a lso h igh e r fo r wo m e n : 35% a s op p osed to 29% for m en in th e 15-30 a ge grou p (ABT Associa tes In corp ora tion , 2000).
Th is p a t t e r n is sim ila r t o t h a t o f m o st Su b -Sa h a ra n c o u n t r ie s (N d ia ye, 2000; Tu r sh e n , 1991; Wh it e sid e & Su n t e r, 2000). D a t a fro m a recen t stu d y in Ca rleton ville (a m in in g town on t h e We st Ra n d o f Ga u t e n g) su p p o r t a n d a u g-m en t th is a la rg-m in g scen a rio: a n extra ord in a rily h igh ra te of in fection wa s fou n d a m on g a d oles-c e n t gir ls, re a oles-c h in g n e a r ly 60% a t 25 ye a r s o f a ge (Gilgen et a l., 2000).
Social and economic impact
of the epidemic
An ep id em ic o f th is m a gn itu d e in a p o p u la tio n will in e vit a b ly h a ve d ire e c o n o m ic a n d so c ia l co n seq u en ces. Th ese will b e m a n ifested o n th e m a c ro - so c ie t a l a n d c o m m u n it y le ve ls a n d b e e xp e r ie n c e d b y fa m ilie s a n d in d ivid u a ls. Al-t h o u gh Al-t h e e p id e m ic is p ro je cAl-t e d Al-t o p e e k o n ly a rou n d 2010 ( Wh itesid e & Su n ter, 2000), its im p a c t is a lre a d y e vid e n t o n va r io u s le ve ls. Re -p o r t s e m a n a t in g fro m t h e c o m m e rc ia l se c t o r in d ic a t e h igh le ve ls o f a b se n t e e ism a n d ill-h e a lt ill-h in t ill-h e wo rkp la c e ; t ill-h e n u m b e r o f AID S o rp h a n s is a lrea d y p la cin g a serio u s b u rd en o n we lfa re a n d h e a lt h a ge n cie s; t h e lo ca l m u n icip a lities a re icip red ictin g a la ck of sicip a ce a n d in fra -stru ctu re to co p e with th e growin g n u m b ers o f t h e d e a d ; t h e e xist in g h e a lt h ca re fa cilit ie s a re stru gglin g to co p e with th e tre a tm e n t o f AIDSre la t e d co n d it io n s; a n d t h e gove rn m e n t is u n -willin g to p rovid e effective treatm en t to all
HIV-Figure 7
Proportion of all new infections projected between 1995 and 2010 by gender and age categories.
Source: ABT Associates Incorporation, 2000. 0
% of all new infections
5 10 15 20 25 30
Females (%)
Males (%)
50-54 45-49 40-44 35-39 30-34 25-29 20-24 15-19 10-14 5-9
in fe c t e d p e o p le, in c lu d in g p re gn a n t wo m e n . Th is u n a ccep ta b le govern m en t p olicy h a s b een a m ajor sou rce of d eb ate in p u b lic h ealth circles. AIDS is p ro jected to in crea se in fa n t m o rta l-it y t wo - fo ld a n d c h ild m o r t a ll-it y t h re e - fo ld , e ra sin g ga in s m a d e ove r 50 ye a rs in ch ild su r-viva l. By 2010 a t le a st 4 m illio n So u t h Afr ica n s will h a ve d ie d o f AIDS (IMPACT Pro je ct, 2000). Life e xp e ct a n cy will d e cre a se fro m 63 in 1999 t o 40 in 2010 (Bo u r n e, 2000). Th is a n d t h e fa ct th a t m o st o f th e d ea d will b e in th eir m o st eco -n o m ica lly p ro d u ctive yea rs will h a ve p ro fo u -n d e ffe c t s b o t h o n t h e p o p u la t io n st r u c t u re, t h e econ om y, a n d society a s a wh ole.
Societal response
Govern m en t resp o n se b efo re th e 1994 electio n wa s in a d e q u a t e a n d ve r y slow. Alt h o u gh t h e st a t e a ckn owle d ge d t h a t AIDS ca se s h a d b e e n d ia gn osed sin ce 1982, it d id n ot la u n ch a n y ed -u ca t io n a l ca m p a ign s -u n t il se ve ra l ye a r s la t e r. On ce la u n ch e d , th e se ca m p a ign s we re illco n -ce ive d , ra cist , ju d gm e n t a l, a n d b a se d o n fe a r. Th e gove r n m e n t d id n o t a llow a n y ca m p a ign -in g -in sch o o ls o r o n p u b lic t e le visio n o r ra d io. Du e t o t h e a d m in ist ra t io n’s c o n se r va t ive n a -t u re -t h e re wa s a n a b so lu -t e re lu c -t a n c e -t o d isc u ss se x in p u b liisc fo ra . Alt h o u gh t h e gove r n -m e n t h a s c h a n ge d , t h is re lu c t a n c e p e r sist s, th u s seriou sly h a m p erin g h ea lth p rom otion in -terven tion s.
Ne e d le ss t o sa y, t h is a p p ro a c h h a s b e e n stro n gly criticized by co n cern ed h ea lth p ro fession a ls a n d va riou s b od ies with a m ore resp on -sib le visio n (Crewe, 1997; Evia n , 1993). Howev-er, p rotests fell on d ea f ea rs a n d were n ot tra n s-la te d in to e ffe ctive in te r ve n tio n . Mo st o f th e se b od ies con ven ed in 1992 to form NACOSA (Na -t io n a l AIDS Co m m i-t -t e e o f So u -t h Africa ) wh ich was m an d ated to d evelop a n ation al AIDS stra t-e gy a n d im p lt-e m t-e n ta tio n p la n s. By 1994, So u th Afr ic a h a d a Na t io n a l AID S Pla n b a se d o n t h e u n d e rst a n d in g o f t h e d ise a se, it s so cia l d e t e r-m in a n ts, a n d its p o ten tia l ir-m p a ct o n so ciety a s a wh o le. As a sse r t e d b y Cre we (2000:27): “N o on e cou ld claim th at th e cou n try d id n ot k n ow w h at it w as facin g”.Th e Na t io n a l Pla n wa s a c-ce p t e d a n d e n d o r se d b y t h e Gove r n m e n t a n d su p p o rt e d b y a ra n ge o f o t h e r re le va n t o rga n i-za t io n s. Th e cr u cia l ro le o f p e o p le livin g wit h H IV/ AIDS wa s reco gn ized , a n d th ey were to b e in vo lve d in a ll st a ge s o f p o lic y a n d p ro gra m p la n n in g a n d im p le m e n t a t io n . Alt h o u gh it se e m e d a t t h e t im e t h a t a ll p a r t ie s we re fu lly c o m m it t e d , t h e p la n d id n o t c o m e t o ge t h e r,
a n d “in stead Sou th Africa h as been in m an y
w ays tou ch ed by th e ven gean ce of AIDS”(Crewe, 2000:28). It is b e yo n d t h e sco p e o f t h is re vie w t o e xa m in e t h e re a so n s b e h in d t h is sit u a t io n , b u t se r io u s le sso n s fo r fu t u re p u b lic h e a lt h p ro gra m s ca n b e le a rn e d fro m it (Cre we, 2000; Ma ra is, 2000; Sch n eid er & Stein , 2001).
Fo llowin g t h e fa ilu re o f t h e st a t e t o in t e r -ven e effectively, so ciety a t la rge wa s m a in ly ign oraign t at th e begiign ign iign g aign d p reju diced th rou gh -o u t , m a in t a in in g t h e d e a fe n in g sile n ce a n d in c o m b in a t io n wit h t h e so c ia l fa c t o r s o u t lin e d ea rlier fa cilita tin g th e ep id em ic’s ra p id growth .
Discussion and conclusions
Th ere is n o d o u b t th a t th e H IV/ AIDS ep id em ic in So u th Africa is a t a critica l p h a se. Acco rd in g to Crewe (2000:23), it h a s th ree m a in ch a ra
cter-istics: “rap id an d u n ch eck ed grow th”; “a lack of
an y coh eren t p olicy d ocu m en ts on cru cial is-su es”; a n d “failu re of p u blic p reven tion cam -paign s to h ave an im pact”.
Th e ove r vie w p re se n t e d in t h is p a p e r co n -firm s t h is, b u t su gge st s a fo u rt h fe a t u re, p e rt i-n e i-n t t o t h e u i-n d e r st a i-n d ii-n g o f t h e e p id e m ic ii-n So u t h Afr ica , n a m e ly, t h a t m o st o f t h e p e o p le a ffe ct e d b y t h e e p id e m ic a re d isa d va n t a ge d in t e r m s o f c la ss, ra c e, a n d ge n d e r, a n d a re t h u s a lso m o re vu ln e ra b le (Gilb e r t & Wa lke r, 2000). It is e vid e n t t h a t we m u st t a ke b o t h t h e so cia l a n d b io lo gic a l d im e n sio n s o f H IV/ AID S in t o a cco u n t . Howe ve r, t h e So u t h Afr ica n sce n a r io su p p o r t s t h e n o t io n t h a t t h e so cia l d im e n sio n is fa r m o re p erva sive a n d cen tra l th a n is u su a l-ly b elieved , even by p u b lic h ea lth p ra ctitio n ers (Crewe, 1997).
Th e re a re a n u m b e r o f so cia l fa ct o rs wh ich h a ve in flu en ced th e p a ttern a n d severity o f th e H IV/ AIDS ep id em ic in So u th Africa . Acco rd in g t o ABT Asso cia t e s In co rp o ra t io n (2000), t h e se in clu d e: esta b lish ed ep id em ics of oth er sexu a l-ly t ra n sm it t e d d ise a se s; d isr u p t e d fa m il-ly a n d c o m m u n a l life, d u e in p a r t t o a p a r t h e id , m i-gra n t la b o r p a ttern s, a n d h igh levels o f p overty in t h e re gio n ; go o d t ra n sp o r t in fra st r u c t u re a n d h igh m o b ilit y, a llowin g fo r ra p id m ove -m en t o f th e viru s in to n ew co -m -m u n ities; resis-ta n ce to co n d o m u se, b a se d o n so cia l a n d cu l-tu ra l n orm s; th e low sta l-tu s of wom en in society a n d with in rela tio n sh ip s; so cia l n o rm s th a t a c-cep t or en cou rage large n u m b ers of sexu al p a rt-n e r s, e sp e c ia lly fo r m e rt-n ; a rt-n d p a ra lle l rt-n o r m s th at frown u p on op en d iscu ssion of sexu al m a t-t e rs, in clu d in g se x e d u ca t-t io n fo r ch ild re n a n d teen a gers.
References
ABDOOL-KARIM, Q., 2000. Tren d s in HIV/ AIDS in fec-tion : Beyon d cu rren t statistics.Sou th African Jou r-n al of Ir-n terr-n atior-n al Affairs,7:1-21.
ABT ASSOCIATES IN CORPORATION , 2000. Th e Im -p en d in g Catastro-p h e: A Resou rce Book on th e Em ergin g HIV/AIDS Ep idem ic in Sou th Africa.Jo -h a n n esb u rg: Love Life Progra m m e.
BOURNE, D., 2000. Dem ogra p h ic im p lica tion s for d e-ve lo p m e n t in So u th Africa a s a re su lt o f th e AIDS e p id e m ic – A gra p h ic re vie w. Urban Health an d Developm en t Bu lletin ,3:8-12.
CASE ( Th e Co m m u n it y Age n c y fo r So c ia l In q u ir y), 1995. Th e N ation al Hou seh old Su rvey of Health In equ alities in Sou th Africa.Du r b a n : He n r y J. Ka iser Fa m ily Fou n d a tion .
CREWE, M ., 1997. How m a rgin a l is a m a rgin a lise d grou p ? Social Scien ce an d Medicin e,45:967-970. CREWE, M ., 2000. So u t h Afr ic a : To u c h e d b y t h e
ve n ge a n c e o f AID S – Re sp o n se s t o t h e So u t h Africa n e p id e m ic. Sou th African Jou rn al of In ter-n atioter-n al Affairs,7:23-37.
EVIAN , C., 1993. Th e so cio - e co n o m ic d e t e r m in a n t s o f t h e AIDS e p id e m ic in So u t h Africa – A cycle o f p ove r t y. Sou th African Med ical Jou rn al, 83:635-636.
GILBERT, L.; SELIKOW, T. A. & WALKER, L., 1966. So-ciety, Health an d Disease – An In trodu ctory Read-er for Health Profession als. Jo h a n n e sb u rg: Ra va n Press.
GILBERT, L. & WALKER, L., 2000. Treadin g th e Path of Least Resistan ce: HIV/AIDS an d Social In equ alities: A Sou th African Case Stu dy. In : XVth In tern a -t io n a l Co n fe re n c e o n -t h e So c ia l Sc ie n c e s a n d Me d icin e <h t t p :/ / www.m so c m rc.gla .a c.u k/ So -cia l Scien ceMed icin e/ ssm .h tm l>.
GILGEN , D.; CAM PBELL, C.; WILLIAM S, B.; TAL-JAARD, D. & M ACPH AIL, C., 2000. Th e N atu ral History of HIV/AIDS in Sou th Africa: A Biom edical an d Social Su rvey in Carleton ville. Jo h a n n esb u rg: Cou n cil for Scien tific a n d In d u stria l Resea rch . IJSSELM ID EN , C. B.; STEIN BERG, M . H .; PAD
AY-ACH EE, G. N .; SCH OU B, B. D.; STRAU SS, S. A.; BUCH , E.; DAVIES, J. C.; DE-BEER, C.; GEAR, J. S. & H U RWITZ, H . S., 1988. AIDS a n d So u t h Afr ica : Towa rd s a c o m p re h e n sive st ra t e gy. Pa r t III. Th e ro le o f ed u ca tio n . Sou th African Medical Jou rn al, 73:465-467.
IM PACT PROJECT (Im p le m e n t in g AID S Pre ve n t io n a n d Ca re Pro je c t ), 2000. Corrid ors of Hop e in Sou th ern Africa.Virgin ia : Fa m ily He a lth In te rn a -tion a l.
HST (Health System s Tru st), 1996. Sou th African Health Review 1995. Du rb a n : Hea lth System s Tru st. KATZENELLENBOGEN, J., 2000. Rep o rt co n firm s gu lf
b e twe e n rich a n d p o o r. Bu sin ess Dayo n th e we b, 25 Ju ly <h ttp :/ / www.bday.co.za/ bday/ in dex/ direct/ 0,3524,6078-0,00.h tm l>.
LOWELL, J., 2000. SA AIDS d ea th ra te h ea d in g for on e a m in u te. Clin ic,22 Novem b er 2000 <h ttp :/ / www. iclin ic.co.za/ n ov00/ reu ters/ aidsstats22.h tm >. MARAIS, H., 2000. To th e Edge: AIDS Review 2000.
Pre-toria : Un iversity of PrePre-toria .
MARKS, S. & TRAPIDO, S., 1987. Th e Politics of Race, Class & Nation alism in Tw en tieth Cen tu ry Sou th Africa. Lon d on : Lon gm a n .
NDIAYE, C. F., 2000. Wo m e n a n d AIDS in Afr ica : Th e exp erien ce o f th e so ciety fo r wo m en a n d AIDS in Africa . Sou th African Jou rn al of In tern ation al Af-fairs,7:59-66.
SCH N EID ER, H . & STEIN , J., 2001. Im p le m e n t in g AID S p o lic y in p o st - a p a r t h e id So u t h Afr ic a . So-cial Scien ce an d Medicin e, 52:723-731.
STATISTICS SOUTH AFRICA, 2000. Stats in Brief 2000. Preto ria : Govern m en t.
SU SSER, I. & STEIN, Z., 2000. Cu lt u re, Se xu a lit y, a n d Wo m e n’s Age n cy in t h e Pre ve n t io n o f H IV/ AID S in So u t h e r n Afr ic a . Am erican Jou rn al of Pu blic Health ,90:1042-1048.
TU RSH EN , M . (e d .), 1991. Wom en an d Health in Africa. New Jersey: Africa World Press.
U N ISA (Un ive r sit y o f So u t h Afr ic a ), 2000. Rep ort of th e Bu reau of M ark et Research,Ju ly 2000.Pre t o -ria : Un iversity of Sou th Africa Press.
WH ITESIDE, A. & SUNTER, C., 2000. AIDS: Th e Ch al-len ge for Sou th Africa. Ca p e Town : Hu m a n & Rou ssea u , Ta felb erg.
Su b m itted on 1 Ma rch 2001
Fin a l version resu b m itted on 8 Au gu st 2001 Ap p roved on 7 Novem b er 2001