www.jped.com.br
ORIGINAL
ARTICLE
Association
between
the
Brazilian
Breastfeeding
Network
implementation
and
breastfeeding
indicators
夽
Danusa
S.
Brandão
a,b,∗,
Sonia
I.
Venancio
c,
Elsa
R.J.
Giugliani
daUniversidadeFederaldoRioGrandedoSul(UFRGS),PortoAlegre,RS,Brazil bMunicipalHealthSecretariatofCaxiasdoSul,CaxiasdoSul,RS,Brazil cInstitutodeSaúde,StateHealthSecretariat,SãoPaulo,SP,Brazil
dDepartmentofPediatrics,FaculdadedeMedicina,UniversidadeFederaldoRioGrandedoSul(UFRGS),PortoAlegre,RS,Brazil
Received21January2014;accepted11June2014 Availableonline6November2014
KEYWORDS
Breastfeeding; Primaryhealthcare; Healthpromotion; Evaluationofhealth programsand projects
Abstract
Objective: ToestimatetheassociationbetweentheimplementationoftheBrazilian
Breast-feedingNetworkandprevalenceofbreastfeedinginamedium-sizecityinsouthernBrazil.
Methods: Thiswasacross-sectionalstudyinvolving405childrenunder1yearwhoparticipated
inthesecondphaseofthemultivaccinationcampaignin2012.Children’sconsumptionoffood onthedaybeforetheinterviewwasobtainedthroughinterviewswithmothersorguardians. ThemanagerandonehealthprofessionalfromeveryhealthfacilitythatjoinedtheNetwork wereinterviewedinordertoinvestigatetheprocessofimplementationofthisinitiative.The associationbetweenprevalenceofbreastfeedingandexclusivebreastfeedingandadherenceto theNetworkimplementationprocesswastestedusingPoissonregressionwithrobustvariance.
Results: Multivariate analysisrevealed thatamong thechildren assisted byhealth facilities
who joined theNetwork andthose attendingservices thatdidnot adhere tothis strategy, the prevalenceofbreastfeeding (74%and70.4%among children under1year,respectively) andexclusivebreastfeeding(43.3%and38.1%amongchildrenunder6months,respectively) didnotdiffersignificantly.DifficultiesinimplementingtheNetwork,suchashighturnoverof professionals,notmeetingthecriteriaforaccreditation,andinsufficientparticipationoftutors intheprocesswereidentified.
夽
Pleasecitethisarticleas:BrandãoDS,VenancioSI,GiuglianiER.AssociationbetweentheBrazilianBreastfeedingNetworkimplementation
andbreastfeedingindicators.JPediatr(RioJ).2015;91:143---51.
∗Correspondingauthor.
E-mail:[email protected](D.S.Brandão).
http://dx.doi.org/10.1016/j.jped.2014.06.009
Conclusion: Contrary to the hypothesis of this study, there was no significant association betweentheimplementationoftheBrazilianBreastfeedingNetworkandprevalenceof breast-feedingandexclusivebreastfeedinginthestudiedcity.Itispossiblethatthedifficultiesfound inimplementingtheNetworkinthiscityhaveinfluencedthisresult.
©2014SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Aleitamentomaterno; Atenc¸ãoprimáriaà saúde;
Promoc¸ãodasaúde; Avaliac¸ãode
programaseprojetos desaúde
Associac¸ãoentreaimplantac¸ãodaRedeAmamentaBrasileindicadoresde aleitamentomaterno
Resumo
Objetivo: Estimaraassociac¸ãoentreaimplementac¸ãodaRedeAmamentaBrasileas
prevalên-ciasdealeitamentomaterno(AM)emummunicípiodemédioportedosuldoBrasil.
Métodos: Estudotransversalenvolvendo405crianc¸asmenoresdeumanoqueparticiparamda
segundafasedacampanhademultivacinac¸ãode2012.Oconsumodealimentospelacrianc¸a nodiaanterioràentrevistafoiobtidomedianteentrevistascomasmãesouresponsáveis.Para investigaroprocessodeimplementac¸ãodaRedeforamentrevistadosogerenteeumprofissional desaúdedecadaunidadequeaderiuaesseprocesso.Aassociac¸ãoentreasprevalênciasdeAM eAMexclusivo(AME)eaadesãoaoprocessodeimplementac¸ãodaRedefoitestadautilizando-se regressãodePoissoncomvariânciarobusta.
Resultados: Aanálisemultivariadarevelouque,entreascrianc¸asassistidasporunidadesque
aderiram ao processo de implementac¸ão daRede eas que frequentavamservic¸os que não aderiram a essa estratégia, as prevalências de AM(74% e 70,4% em menores de um ano, respectivamente) e AME (43,3% e 38,1% em menores de seismeses, respectivamente) não diferiramsignificativamente.Foramidentificadasdificuldadesnaimplementac¸ãodaRede,tais como alta rotatividadedos profissionais,não cumprimentodos critérios para certificac¸ãoe acompanhamentoinsuficientedasunidadespelostutoresdaRede.
Conclusão: Contrariando a nossa hipótese, não houve associac¸ão significativa entre a
implementac¸ãodaRedeAmamentaBrasileasprevalênciasdeAMeAMEnomunicípio estu-dado.Épossívelqueasdificuldadesencontradasnaimplementac¸ãodaRedenessemunicípio tenhaminfluenciadoesseresultado.
©2014SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Brazil has shown progress on indicators of breastfeeding (BF) since the 1980s, due to the efforts of the govern-ment, non-governmental organizations, universities, and the media,among others.1 However, theseindicators are
stillnotadequate.AccordingtotheNationalDemographic andHealth Survey(DHS) carriedout in 2006, the median durationof exclusive breastfeeding (EBF)and BF was1.4 monthsand 14months, respectively,2 indicating the need
forstrategiesthatpromoteEBFinthefirst6monthsofthe child’slife andcomplemented BFupto2 yearsof age or more.
Until recently, policies for the promotion, protection, and support of BF in Brazil were focused on hospital care, including the adoption of the Baby-Friendly Hospi-tal Initiative and kangaroo care, and the creation of the Brazilian Network of Human Milk Banks. Aiming to meet thelack of BFincentiveactionsinprimary care,the Min-istryofHealthlaunchedtheBrazilianBreastfeedingNetwork [RedeAmamentaBrasil]in2008,aimingtomobilizehealth professionalsworkingatthisattentionlevel,using critical-reflexivemethodology.
Thisstrategyincludedconductingaworkshoplastingsix hours with the entire staff of the health unit, with the participationof at least oneprofessionalfrom each func-tional category, including administrative and outsourced personnel,duringwhichtheprocessofworkingtowardsthe promotion, protection, and support of BF was discussed, exposingdifficultiesandagreeingonactionswhileseeking solutionsbasedonthelocalreality.3Italsoprovidedforthe
supportofthehealthunitthoughregularvisitsofaNetwork tutor, trainedtoencourageandsupporttheservice inthe promotion,protection,andsupportofBFintheircoverage area.
Fortheunittobecertified,ithadtomeetthefollowing criteria: participationof atleast80%of staffin the work-shop;continuousmonitoringofBFindicatorsinitscoverage area;completionofatleastoneactionagreeduponatthe workshop; andimplementation of the care flow chartfor bothmotherandchildduringtheBFperiod.4
thePromotionofHealthyComplementaryFeeding [Estraté-gia Nacional de Promoc¸ão da Alimentac¸ão Complementar Saudável---ENPACS]in 2011),resulting inhealth care facil-ities witha differentstatus regarding this strategy. As to datethisstrategyhasnothaditsresultsevaluated,itwas deemedappropriatetocarryoutthisstudy,aimedto esti-matethe association between the implementationof this strategy and the prevalence of BF and EBF in a city in southernBrazil.Theinitialhypothesiswasthatpopulations assistedbyhealthservicesthatjoinedtheBrazilian Breast-feedingNetworkimplementationprocesswouldshowbetter indicatorsofBF.
Methods
This was a cross-sectional study conducted in Bento Gonc¸alves,amunicipalityinthemountainousregionofRio Grande doSul, witha population of 107,341 inhabitants, Giniindexof0.45,HumanDevelopmentIndexof0.87, coef-ficientofinfantmortalityof14.1per1,000livebirths,and non-publichealthinsurancecoverageof41.7%.5,6Intheyear
2011,1,274birthsoccurredinthecity.6
Bento Gonc¸alves currently has 22 primary health care facilities (PHCF) and a maternal-child reference center (MCRC).TheprocessofimplementingtheBrazilian Breast-feeding Network in thecity wasstarted inOctober 2009, withsixPHCFhavingbeencertifiedbytheMinistryofHealth untilthetimeofdatacollection, inadditiontotheMCRC, totalingsevencertifiedhealthservices.Duringthisperiod, 14otherPHCFstartedtheNetworkimplementationprocess andhadtheworkshop,but werenotcertified.Twoof the 22PHCF and allprivatehealth servicesor health services fundedbynon-publichealthinsurancecompanieswerenot exposedtoany actionby theBrazilian Breastfeeding Net-work.
To characterize the services that adhered to the pro-cessoftheBrazilianBreastfeedingNetworkimplementation regarding the status of this strategy, the researchers performed interviews with 21 managers and 20 health professionals with higher education from these units. At thattime,informationwascollectedontheverificationof compliance with the four criteria required for the BHU’s certification with the Network, on participation of tutor in the process through visits to the unit, and care pro-videdformothersandbabies,includingtheuseofprotocols andflowcharts,clinicalmanagement,andcounseling.For theseinterviews,thesameresearchquestionnairesusedfor theanalysisoftheimplementationoftheBrazilian Breast-feedingNetwork were utilized.3 These dataallowed for a
comparisonbetween theservicescertified bytheMinistry ofHealth,i.e.,theonesthatmetthecertificationcriteria atthetimetheywereassessed,andthosethathadinitiated theNetworkimplementationprocesswiththeworkshop per-formance,butthathadnotyetbeencertifiedbytheMinistry ofHealthatthetimeofdatacollection.
To estimatethe prevalenceof EBFandBFin thestudy population,thisstudyaimedtoincludeallchildrenyounger than1yearwhocametothePHCFonthedayassignedfor the vaccination against polioduring the 2012 vaccination campaign.ThismethodologyhasbeenwidelyusedinBrazil, bringingimportant contributionstotheanalysis ofthe BF
situationin thecountry,andhelping toformulatepolicies andplanactions.7 Considering thatthe municipality
initi-atedthiscampaigninpublicandprivatepreschoolsinthe weekpriortovaccinationday,datacollectionwasextended totheselocations.Topreventthesamechildfrom partici-patingtwiceinthestudy,thechildren’sdatawereverified todetectanyduplication.
Totest thesamplerepresentativeness,the characteris-ticsof the children included in the study were compared withthoseof children younger than1 year in the munic-ipality,using datafromthe LiveBirth Information System (Sistema de Informac¸ão sobre Nascidos Vivos [SINASC]), relatedtobirthsin2011.Forthatpurpose,thechi-squared test withYates correction wasperformed andthe signifi-cancelevelwassetatp<0.05.
Thedatacollectiontoolwasbasedonthequestionnaire used in the II Breastfeeding Prevalence Survey (Pesquisa dePrevalência de Aleitamento Materno [PPAM]) and con-tainedsevenquestionsonconsumptionofbreastmilk,other kindsofmilk, andother foods,includingwater, teas,and otherliquidsonthedaybeforetheinterview,followingthe WHOrecommendations forBFsurveys.7 Inadditiontothe
dietarysurvey,thequestionnaireincludedquestionsrelated tothehealthservicethechildusedtomonitorgrowthand development,includingpublic,fundedbynon-publichealth insurancecompaniesandprivatehealthservices.Datawere collectedby40properlytrainedinterviewersrecruitedfrom healthservicesandtechnicalandhighereducationcourses oftheregion,distributedin25vaccinationunitsthroughout thecity,includingallPHCF.
Tocharacterizethedietaryhabits,thefollowing defini-tions were considered: EBF when the child received only breastmilkwithoutanyotherfood,solidor liquid,except medications;andBF,whenthechild receivedbreastmilk, regardless of whether she received other foods or not, includingliquids.8
Stata11.0software(StataCorpLP,TX,USA)wasusedfor the database and statistical analysis. Descriptive analysis wasperformedbycalculatingmeansandstandarddeviations ofquantitativevariables andsimple frequency of qualita-tivevariables.ThecomparisonoftheprevalenceofEBFand BFaccordingtofollow-uplocationwasperformedusingthe Yates-correctedchi-squaredtest,usingasignificancelevel of0.05.
To test the association between the child’s place of follow-upandBFindicators,Poissonregressionwithrobust variance was used, taking into account variables which, according tothe literature,could be interferingwiththe results.Initiallysimpleregressionswereused,considering the dependent variable and each of the following inde-pendent variables: child’s age; mother’s age, parity, and educationallevel;cohabitationwiththechild’sfatherand grandmother; area of residence (urban or rural); type of delivery;BFinthefirsthourafterbirth;problemswithBF; timethatthemotherspendswiththechild;andpacifieruse. Independentvariableswithp<0.20wereselectedforthe multivariatemodel,withtheexceptionofmaternal educa-tionandage,astheyhavebeenconsideredrelevantfactors inother studies9,10 andbecause theyshoweda significant
Table1 Characterizationofhealth servicesaccordingtothecriteria forBrazilian Breastfeeding Networkcertificationand participationoftutors-BentoGonc¸alves,2012.
Certifiedservice(n=7) Servicewithworkshop,non-certified(n=14)
BrazilianBreastfeedingNetwork certificationcriteria
n Frequency N Frequency
Minimumof80%ofemployees/currentstaff attendedtheworkshop,withatleastone professionalfromeachfunctional category,includingadministrativeand outsourcedpersonnel
0 0% 0 0%
MonitoringofBFindicatorsforatleast threeconsecutivemonthsa
7 100% 4 28.6%
Existenceofacareflowchartforboth motherandinfantduringtheBFperiod, collectivelycreatedbytheentireprimary careteam
7 100% 6 42.9%
Implementationofatleastoneactionplan createdandagreeduponattheworkshop
7 100% 6 42.9%
Participationoftutorintheprocess
Regularvisits(withanintervalofatleast threemonths)
0 0% 0 0%
Non-regularvisits(withanintervalof morethanthreemonths)
7 100% 3 14.2%
Novisitrecording 0 0% 11 52.3%
aInformationrelatedtothemonthsofApril,May,andJuneof2012.
This study wasapproved by the Municipal Health Sec-retariat of Bento Gonc¸alves and by the Research Ethics CommitteeofUniversidadeFederal doRioGrandedoSul. Allrespondentssignedtheinformedconsent.
Results
Ofthe20PHCFthatheldtheworkshop,45%(n=9)belongto theFamilyHealthStrategy(FHS),30%(n=6)donotperform childcarefollow-up,and40%(n=8)donotperformprenatal care.Regardingthecertifiedfacilities,allPHCFexceptthe MCRCbelongtotheFHS.
The workshopsinthe healthservicesthat initiatedthe Networkimplementationprocesswerecarriedouton aver-age 24 months before the performance of this study for thosethatwerecertified(SD=6.17)and17monthsforthe non-certified(SD=4.16).
Thecharacterizationofhealthservicesaccordingtothe adequacyofthecriteriaforcertificationandmonitoringof theunitatthetimeofdatacollectionisshowninTable1.
Itwasfoundthat47.5%(n=153)ofthe322health profes-sionalswhowereworkingatthetimeofdatacollectionin the21servicesthatstartedtheprocessofimplementingthe BrazilianBreastfeedingNetworkjoinedtheunitafter com-pletionoftheworkshopandthatotherworkshopswerenot offeredfornewemployeesuntilthen.Approximately one-quarter of the 41 professionals interviewed (26.8%) were unaware of the existence of the care flowchart for both motherand babyduringBF.Regarding theuseof BF man-agementprotocols,thisstudyverifiedtheabsenceofuseof suchprotocolsin95.2%ofunits(n=20).
InformationwasobtainedonBF,EBF,andplaceofgrowth anddevelopmentmonitoringof405 childrenyoungerthan 1year,representing31.7%ofthepopulationyoungerthan1 yearlivinginthecity.Ofthese,191(47.2%)werefollowed intheprimarycarenetworkoftheBrazilianUnifiedHealth System (SistemaÚnicodeSaúde[SUS])and214 (52.8%)in private/funded by non-publichealth insurancecompanies healthservices.Ofallchildrenevaluated,181(94ofwhom were youngerthan 6months) werefollowed in units that joined the implementation of the Brazilian Breastfeeding Network and224 (102youngerthan 6months)at services thatdidnotadheretothisstrategy.
With this sample, to study the association between implementationoftheBrazilianBreastfeedingNetworkand prevalence of BFand EBF, witha confidence level of 95% and astudy power of80%, it wouldbe possibletodetect differencesofapproximately12%intheprevalenceofBFin childrenyoungerthan1yearand14%intheprevalenceof EBF inchildren younger than 6months, starting fromthe prevalenceratesfoundinthepopulationnotexposedtothe Networkimplementation(38%forEBFand70%forBF).
When the sample was compared with the universe of childrenyoungerthan1yearinthecity,therewasno statis-ticallysignificantdifferenceregardinggender,typeofbirth, andmaternaleducationlevel.However,therewere differ-encesregardingthemother’sage.Thesamplehadalower frequencyofadolescentmothers(6.3%versus10.6%inthe referencepopulation,p=0.03).
Table2 Characteristicsofthechildrenyoungerthan1year,accordingtoadherencetotheBrazilianBreastfeedingNetwork implementationprocess,intheserviceswheretheirgrowthanddevelopmentweremonitored-BentoGonc¸alves,2012.
Servicesthatadheredtothe Networkimplementation
process(na=181)
ServicesthatdidnotadheretotheNetwork implementationprocess
(n=224)
Variable n Frequency n Frequency pb
Area
Urban 172 0.95 207 0.924 0.747
Rural 9 0.05 17 0.075
Gender
Male 97 0.536 115 0.513 0.123
Female 84 0.464 109 0.486
Delivery
Normal 99 0.55 50 0.227 0
Cesarean 81 0.45 170 0.772
Child’sage
0to90days 47 0.26 48 0.214 0.611
91to180days 47 0.26 54 0.241
181to270days 41 0.226 58 0.258
271to365days 46 0.254 64 0.285
Useofpacifier 102 0.576 147 0.677 0.095
Mother’sage
11to19years 16 0.11 5 0.026 0
20to34years 109 0.752 137 0.717
35yearsorolder 20 0.138 49 0.256
Educationallevel
1to7years 30 0.205 17 0.089 0
8to11years 102 0.699 95 0.497
12yearsormore 14 0.096 79 0.414
Timespentwiththechild
Fulltime 94 0.653 107 0.566 0.08
Parttimeduringthedayandatnight 10 0.069 27 0.142
Onlyatnight 40 0.278 55 0.291
EBFandBFadviceduringprenatalperiod 135 0.925 182 0.957 0.143
Firstchild 67 0.462 120 0.628 0.001
ProblemsduringBF 40 0.274 53 0.301 0.34
Liveswiththechild’sfather 129 0.896 176 0.931 0.17
EBF,exclusivebreastfeeding;BF,breastfeeding.
a n=numberofchildren.
b Yatescorrectedchi-squaredtest.
a higherproportion of childrenborn by cesarean section, tomothersolderthan 35years,motherswitheducational level equal to or greater than 12 years of schooling, and primiparouswomen.
The EBF prevalencein children youngerthan6 months was 38.8%, with a median duration of 54.5 days. The prevalence of BF among infants younger than 1 year was 71.9%,withamediandurationof157days.Ifonlythe pri-vate/fundedbynon-publichealthinsurancecompaniescare networkis considered,theserates were36.2%and 70.1%, respectively.
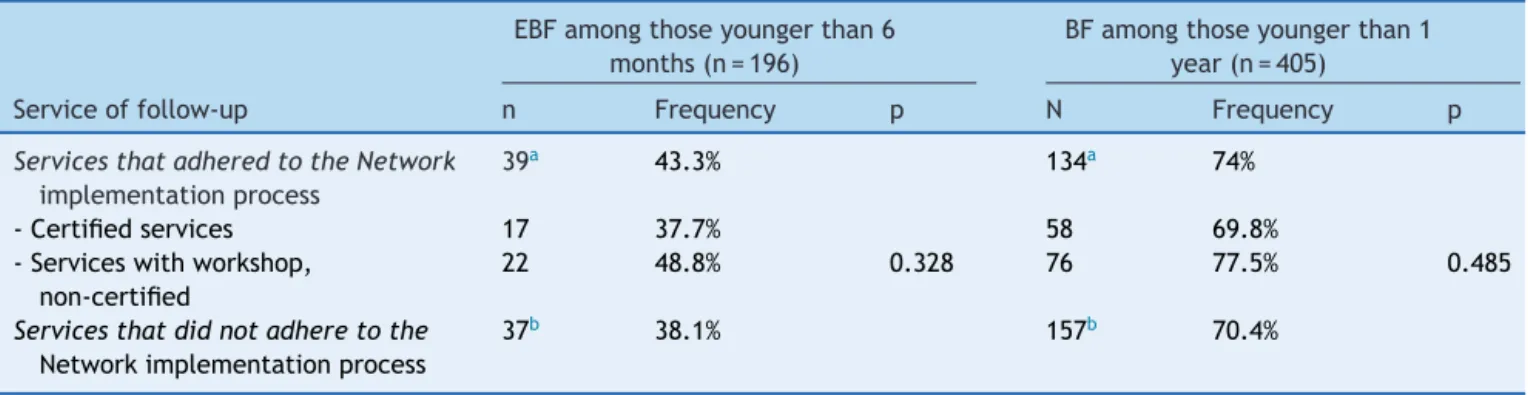
Table3showstheprevalenceofEBFandBFaccordingto placeoffollow-up.Thebivariateanalysisshowedno statis-ticallysignificantdifferencesintheprevalenceofEBFand BFamongchildrenfollowedatunitsthatjoinedtheBrazilian
BreastfeedingNetwork (certifiedor undergoingthe certifi-cation process) andthose attending services that didnot jointhe Network. This resultwasconfirmed in the analy-sisofPoissonregressionwithrobustvarianceandcrudeand adjustedPR(Table4).
Discussion
Table3 Prevalenceofexclusivebreastfeedingandbreastfeedingaccordingtotheserviceofchildfollow-up-BentoGonc¸alves, 2012.
EBFamongthoseyoungerthan6 months(n=196)
BFamongthoseyoungerthan1 year(n=405)
Serviceoffollow-up n Frequency p N Frequency p
ServicesthatadheredtotheNetwork
implementationprocess
39a 43.3% 134a 74%
-Certifiedservices 17 37.7% 58 69.8%
-Serviceswithworkshop, non-certified
22 48.8% 0.328 76 77.5% 0.485
Servicesthatdidnotadheretothe
Networkimplementationprocess
37b 38.1% 157b 70.4%
EBF,exclusivebreastfeeding;BF,breastfeeding.
an=numberofchildren.
b Yatescorrectedchi-squaredtestcomparing‘‘a’’and‘‘b’’.
Thisresultmayberelatedtothedifficultiesfoundinthe networkimplementationinthiscity,suchasdiscontinuityof compliancewiththecriteriaforcertificationintheBrazilian BreastfeedingNetworkinunitsthathadalreadybeen certi-fied,duetohighstaffturnover;lowdegree ofcompliance withthecriteriabymostunitsthatinitiated the certifica-tionprocessintheNetwork,buthadnotyetbeencertified at the time of data collection; and lack of awareness by theprofessionalsoftheexistenceofthecareflowchartfor bothmotherandbabyduringBFintheseunits,eveninthose whereitwasestablished.FailuretousetheBFmanagement protocols,including by the certifiedunits, mayalso have contributedtothelack ofassociation betweenthe imple-mentation of the Brazilian Breastfeeding Network and BF indicators.
Althoughregularvisitsfromthetutortrainedtoexercise this function is not a criterion for certification, the Min-istryofHealth,whenproposingthecreationoftheBrazilian BreastfeedingNetwork, emphasizedtheimportanceofthe participationoftutorintheimplementationprocessforthe success of thestrategy, suggesting a minimum intervalof threemonthsbetweenvisits.4Itwasobservedthatthecity
haddifficultyfollowingthisroutinefollow-up,asnoservices werevisitedbythetutorquarterly.Thevisitsoccurred pri-marilyincertifiedunits,althoughatagreaterintervalthan the recommended schedule of three months.Considering thattheBrazilianBreastfeedingNetworktutorhastherole ofencouragingandsupportingthehealthunitinthe promo-tion,protection,andsupportofBF,insufficientparticipation oftutorsfoundinBentoGonc¸alvesmayhavesubstantially contributedtothelackofassociationbetweenthisstrategy andtheprevalenceofBF.
Some difficulties found in the implementation of the Brazilian Breastfeeding Network in the study municipality had already been indicated in a study on the analysis of theimplementationoftheBrazilianBreastfeedingNetwork carriedoutin2011inthreemunicipalities(Ribeirão Preto-SP,Corumba-MT,andPortoAlegre-RS),suchasdifficultyin maintainingthemonitoringofindicators,highstaffturnover, andlackofBFmanagementprotocols.3
ItisimportanttomentionthattheprevalenceofBFand EBF weresimilar among certified services andthose that hadhadtheworkshop,butwerenotcertifiedatthetimeof
theresearch,withanevenhigherprevalence,althoughnot statisticallysignificant,oftheseindicatorsinnon-certified units. Theexpectationwasthat BFindicatorsamong chil-drenfollowedatcertifiedserviceswouldbemorefavorable thanintheothers.Thisresultreinforcesthehypothesis of difficultiesinthefullimplementationofthestrategyasit wasconceivedandsuggeststheneedtoreassessthecriteria adoptedforcertificationandrecertification.
TheEBFprevalenceinchildrenyoungerthan6monthsin thepresentstudy(38.8%)showedtobealittlelowerthan the national prevalence found in the II Surveyon Breast-feedingPrevalence(41%),butsimilartothatfoundinPorto Alegre,capitalcityofthestate(38.2%)7andintheNational
DHScarriedoutin2006(38.6%).2
TheprevalenceofBFinchildrenyoungerthan12months foundinthisstudy(68.5%)wasslightlylowerthanthe preva-lencefoundinthesamemunicipalityinastudyperformed in2008(71.1%),11suggestingnoimprovementinBF
indica-torswiththeimplementationoftheBrazilianBreastfeeding Networkuptothetimeofthisresearch.Althoughthe pur-poseofthisstudywasnottoinvestigatefactorsassociated toEBFandBF,it isemphasizedthat thefactorsfoundfor bothEBF(child’sageandproblemsinthebreastduringBF) as well asfor BF (child’s age,pacifier use, andproblems inthebreastduringBF)havebeen previouslydescribed in otherstudies.7,12---17
Thelimitationsofthestudymayincludean insufficient numberofchildrentodetectsmalldifferencesinthe preva-lenceofBFamongthechildrenfollowedatPCHFthatjoined anddidnotjointheNetwork,asoccurredinthisstudy(5.2% forEBFand3.6%forBF).Usingclassicalsampling parame-ters (confidence level of 95% andstudy power of 80%), it would onlybepossible todetect differencesgreater than thosefoundinthisstudy,butthathavebeenfoundin sev-eral more successfulinterventions in Brazil18,19 andother
countries.20,21
Thefactthattherewasalowerrateofadolescent moth-ers in the sample when comparedwith thepopulation of children younger than 1 year in the municipality might overestimatetheprevalenceofEBF,consideringthatsome studies show an association between young maternal age andlowerprevalenceofEBF.7,16 However,this
Table4 Resultofthemultivariateanalysiswhentestingtheassociationbetweenprevalenceofexclusivebreastfeeding(EBF)in childrenyoungerthan6monthsandbreastfeeding(BF)inchildrenyoungerthan1yearandservicesofchildfollow-upaccording toadherencetotheBrazilianBreastfeedingNetwork-BentoGonc¸alves,2012.
Exclusivebreastfeeding Breastfeeding
Variable CrudePR CI Adjusted PR
CI CrudePR CI Adjusted PR
CI
Serviceoffollow-up
Servicesthatadheredto theNetwork
implementationprocess
1.00 - 1.00 - 1.00 - 1.00
-Servicesthatdidnot adheretotheNetwork implementationprocess
0.78 0.50-1.23 0.871 0.53-1.41 0.95 0.75-1.19 1.03 0.79-1.33
Child’sage
0to90days 1.00 - 1.00 - 1.00 - 1.00
-91to180days 0.38 0.26-0.61 0.42 0.25-0.71 0.91 0.67-1.21 0.97 0.70-1.34 181to270days - - - - 0.64 0.47-0.87 0.77 0.53-1.09 217to365days - - - - 0.58 0.42-0.80 0.59 0.40-0.85
Mother’sage
11to19years 0.52 0.15-1.77 0.51 0.14-1.76 0.73 0.40-1.33 0,79 0.42-1.46 20to34years 0.72 0.41-1.24 0.80 0.45-1.42 0.89 0.66-1.19 0,94 0.69-1.28
35yearsorolder 1.00 - 1.00 - 1.00 - 1.00
-Timespentwiththechild
Fulltime 1.00 - 1.00 - 1.00 - 1.00
-Parttimeduringtheday andatnight
0.15 0.03-0.63 0.51 0.12-2.15 0.86 0.57-1.30 1.17 0.75-1.84
Onlyatnight 0.02 0.00-0.21 0.17 0.02-1.31 0.72 0.54-0.97 0.97 0.67-1.41
Educationallevel
1to7years 1.13 0.53-2.40 0.72 0.33-1.55 0.91 0.60-1.36 0.81 0.53-1.24 8to11years 0.99 0.56-1.73 0.87 0.49-1.55 0.97 0.73-1.29 0.90 0.67-1.21
12yearsormore 1.00 - 1.00 - 1.00 - 1.00
-Useofpacifier
Yes 0.5 0.32-0.79 0.68 0.43-1.07 0.61 0.49-0.76 0.73 0.57-0.95
No 1.00 - 1.00 - 1.00 - 1.00
-ProblemsduringBF
Yes 0.5 0.26-0.96 0.45 0.23-0.87 0.69 0.50-0.93 0.71 0.51-0.96
No 1.00 - 1.00 - 1.00 - 1.00
-Firstchild
Yes 0.71 0.44-1.13 0.80 0.49-1.29 0.95 0.74-1.21 1.04 0.81-1.35
No 1.00 - 1.00 - 1.00 - 1.00
-PR,prevalenceratio;CI,confidenceinterval.
intothemultivariateanalysismodel,whichminimizes this possiblelimitation.Anotherpossibilityofbiaswouldbethe factthatmost oftheinfants followedin servicesthatdid notjointheBrazilianBreastfeedingNetworkwerefollowed inthenon-publichealthsystem,attendedbymotherswith highereducationallevel.
The National DHS-20062 showed that the duration of
EBF and BF among women with higher educational level is shorter, and the II Survey onBreastfeeding Prevalence in Brazilian Capital Cities7 confirmed this finding for BF,
but showed opposite results for EBF. It is believed that thispossiblebiasissmallinthepresentstudy,asprevious research carriedout in the same municipality showed no
associationbetweenprevalence ofEBFandmaternal edu-cational level, familyincome, or service of prenatal care (SUSornotSUS).11
Several studies have shown that educational interven-tions topromote and support BF significantly improve BF indicators.23---27Thus,asignificantpositiveassociationwould
beexpectedbetween theimplementationoftheBrazilian BreastfeedingNetwork anda higherprevalence ofBFand EBF,whichdidnotoccur.However,cautionisneededwhen interpretingthisresult.Thesamestrategy,whenassessedin RibeirãoPreto,SP,showedpositiveresults.Inthatcity,the prevalenceof EBF inchildren youngerthan 6months was significantly higher (OR=1.41, 95% CI=1.01-1.95) among children followed in health facilities that performed the workshopoftheBrazilianBreastfeedingNetwork.22
This resultsuggeststhat theNetwork can bean effec-tivestrategytoincreaseEBFrates.Moreover,aspreviously mentioned,severaldifficultieswereobservedwhen imple-menting the strategy in the municipality of the present study.These difficulties must be analyzed in the context of the current Brazilian health system: lack of material and human resources, excessive responsibilities of health professionals, lack of an attractive career plan to keep the professionals in their workplaces, and discontinuity of programs and adoption of new programs with new policy-makers,oftenresultingindemotivationofhealth pro-fessionals.
In this scenario, the implementation of the Brazilian Breastfeeding Network, as planned in the current health caremodel,becomesachallenge.Theanalysisofthe imple-mentation of the Network, conducted by the Ministry of Health in 2011, already showed low prioritization of the Network in state health plans, difficulties in the discus-sion process about its implementation at the municipal level,andcompetitionwithexistinggovernmentalprojects and programs as hindering factors to the adherence and maintenanceof the Network in healthcare facilities. This evaluationalsoshowedthatthegoodexperiencesregarding theimplementationofthisstrategywerenotrelatedto iso-latedmotivationor performanceofindividuals,butrather linked to an institutional project, with support from the municipalmanagement.3
Thus, we believe that the inclusion of the promotion, protectionandsupportofbreastfeedinginthelistofhealth prioritiesinthethreegovernmentalspheres(federal,state andmunicipal)andareflection onthelack of association betweentheimplementationoftheBrazilianBreastfeeding Network andBFindicators described here maycontribute forplanning andstrengtheningof actionsaimedat better feedingpracticeswithimpactonchildren’shealth.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Rea MF. Reflexões sobre a amamentac¸ão no Brasil: de como passamosa 10 mesesde durac¸ão. CadSaude Publica. 2003;19:37---45.
2.Brasil,MinistériodaSaúdePesquisaNacionaldeDemografiae
SaúdedaCrianc¸aedaMulher---PNDS2006:dimensõesdo
pro-cessoreprodutivoedasaúdedacrianc¸a.Brasília:Ministérioda
Saúde;2009.
3.Brasil,MinistériodaSaúdeAnálisedeimplantac¸ãodaRede
Ama-mentaBrasil.Brasília:MinistériodaSaúde;2013.
4.Brasil,MinistériodaSaúdeRedeAmamentaBrasil:osprimeiros
passos(2007-2010).Brasília:MinistériodaSaúde;2011.
5.ProgramadasNac¸õesUnidasparaoDesenvolvimento.Atlasdo
desenvolvimentohumanonoBrasil.[cited11Mar2012].
Avail-ablefrom:http://www.pnud.org.br/atlas/
6.BentoGonc¸alves,SecretariaMunicipaldeSaúde.Relatório
Epi-demiológico:natalidade. 6a revisão. BentoGonc¸alves, 2011.
[cited 15 Nov 2011]. Available from:
http://www.bento-goncalves.rs.gov.br/
7.Brasil.MinistériodaSaúdeII.PesquisadePrevalênciade Aleita-mento Materno nas Capitais Brasileiras e Distrito Federal. Brasília:MinistériodaSaúde;2009.
8.WorldHealthOrganization.Indicatorsforassessinginfantand
youngchildfeedingpractices:conclusionsofaconsensus
meet-ingheld6---8November2007inWashingtonD.C.,USA.Geneva:
WHO;2009.
9.Faleiros FT, Trezza EM, Carandina L. Aleitamento materno: fatores de influência na sua decisão e durac¸ão. Rev Nutr. 2006;19:623---30.
10.EspíritoSantoLC,deOliveiraLD,GiuglianiER.Factors associ-atedwithlowincidenceofexclusivebreastfeedingforthefirst 6months.Birth.2007;34:212---9.
11.Beche N, Halpern R, Stein AT. Prevalência do aleitamento maternoexclusivoemummunicípioserranodoRioGrandedo Sul,Brasil.RevAMRIGS.2009;53:345---53.
12.Chaves RG, Lamounier JA, César CC. Fatores associados com a durac¸ão do aleitamento materno. J Pediatr (RioJ). 2007;83:241---6.
13.ScottJA,BinnsCW,OddyWH,GrahamKI.Predictorsof breast-feeding duration: Evidence from a cohort study. Pediatrics. 2006;117:646---55.
14.HowardCR, HowardFM, Lanphear B, EberlyS, deBlieck EA, OakesD,etal. Randomizedclinicaltrialofpacifier useand bottle-feedingorcupfeedingandtheireffectonbreastfeeding. Pediatrics.2003;111:511---8.
15.Salustiano LP, Diniz AL, Abdallah VO, Pinto Rde M. Fatores associados à durac¸ão do aleitamento materno em crianc¸as menores de seis meses. Rev Bras Ginecol Obstet. 2012;34: 28---33.
16.VieiraGO,MartinsCC,VieiraTO,OliveiraNF,SilvaLR.Factors predictingearlydiscontinuationofexclusivebreastfeedingin thefirstmonthoflife.JPediatr(RioJ).2010;86:441---4.
17.Franc¸aGV,BrunkenGS,daSilvaSM,EscuderMM,VenancioSI. Determinantesdaamamentac¸ãonoprimeiroano devidaem Cuiabá,MatoGrosso.RevSaudePublica.2007;41:711---8.
18.CoutinhoSB,LiraPI,LimaMC,AshworthA.Comparisonofthe effectoftwosystemsfor thepromotion ofexclusive breast-feeding.Lancet.2005;366:1094---100.
19.BicaOC,GiuglianiER.Impactofcounselingsessiononthe preva-lenceofbreastfeedinginthefirstyearoflife:arandomized clinicaltrialwithadolescentmothersandgrandmothers.Birth. 2014;41:39---45.
20.Guise JM, Palda V, Westhoff C, Chan BK, Helfand M, Lieu TA.Theeffectivenessofprimary care-basedinterventionsto promotebreastfeeding:systematicevidencereviewand meta-analysisfortheUSPreventiveServicesTaskForce.AnnFamMed. 2003;1:70---80.
21.KramerMS,ChalmersB,HodnettED,SevkovskayaZ,Dzikovich I,ShapiroS,etal.Promotionofbreastfeedinginterventiontrial (PROBIT):arandomizedtrialintheRepublicofBelarus.JAMA. 2001;285:413---20.
22.PassanhaA. Padrão dealeitamentomaterno em menores de
seis meses do município de Ribeirão Preto, segundo apoio
recebidonasmaternidadesenoacompanhamentoambulatorial
[dissertation].SãoPaulo:UniversidadedeSãoPaulo,Faculdade
http://www.teses.usp.br/teses/disponiveis/6/6138/tde-21082012-134251/
23.DysonL,McCormickFM,RenfrewMJ.Interventionsfor promot-ingtheinitiationofbreastfeeding.CochraneDatabaseSystRev. 2005;2:CD001688.
24.OliveiraMI,CamachoLA.Impactodasunidadesbásicasdesaúde nadurac¸ãodoaleitamentomaterno exclusivo. RevBras Epi-demiol.2002;5:41---51.
25.AlbernazE,VictoraCG.Impactofface-to-facecounselingon durationofexclusivebreast-feeding:areview.RevPanamSalud Publica.2003;14:17---24.
26.OliveiraMI,CamachoLA, TedstoneAE.Extending breastfeed-ing duration through primary care: a systematic review of prenatal and postnatal interventions. J Hum Lact. 2001;17: 326---43.