w w w . r b o . o r g . b r
Original
Article
Revision
of
unicompartmental
knee
arthroplasty:
implants
used
and
causes
of
failure
夽
Alan
de
Paula
Mozella
∗,
Felipe
Borges
Gonc¸alves,
Jansen
Osterno
Vasconcelos,
Hugo
Alexandre
de
Araújo
Barros
Cobra
KneeSurgeryCenter,InstitutoNacionaldeTraumatologiaeOrtopedia(Into),RiodeJaneiro,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received3April2013 Accepted9April2013
Availableonline31March2014
Keywords:
Arthroplasty,replacement,knee Revision
Bonegraft
a
b
s
t
r
a
c
t
Objective:todeterminethecausesofunicondylarkneearthroplastyfailures,aswellas iden-tifytheimplantsusedandtheneedofbonegraftinginpatientsundergoingrevisionUKA inCenterofKneeSurgeryattheInstitutoNacionaldeTraumatologiaeOrtopedia(INTO)in theperiodbetweenJanuary1990andJanuary2013.
Methods:aretrospectiveanalysisofthemedicaldocumentationandimaging,determining thecauseoffailureofUKAandthetimeofitsoccurrence,aswellasprostheticcomponents implantedduringthereviewandtheneedforbonegrafting.
Results:inthisstudy,27UKAfailuresin26patientswereincluded.Collapseofoneormore componentswasthemaincauseoffailure,occurringin33%ofpatients.Asepticfailure wasidentifiedin30%ofcases,progressionofosteoarthrosisin15%,infectionandpain7% each,andosteolysisandpolyethylenefailurein4%each.Earlyfailureoccurredin41%ofall revisionsofUKAandlatefailurein59%.23patientshaveundergonerevisionofUK. Conclusion:in35%ofrevisionstheuseofbonegraftingwasneededintibialarea;in3cases weneededallograftfromTissueBank.Wedidnotusemetalincreaseinanyoftherevision. Inonepatientweusedimplantconstraintforinstability.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Revisão
de
artroplastia
unicompartimental
de
joelho:
implantes
usados
e
causas
de
falha
Palavras-chave: Artroplastiadojoelho Revisão
Enxertoósseo
r
e
s
u
m
o
Objetivo:determinarascausasdefalhadaartroplastiaUnicondilar,assimcomoidentificar osimplantesutilizadoseapossívelnecessidadedeenxertiaósseanospacientes submeti-dosàcirurgiaderevisãodeAUJnoCentrodeCirurgiadoJoelhodoInstitutoNacionalde TraumatologiaeOrtopedia-INTO,noperíodoentrejaneirode1990ajaneirode2013foram analisados.
Métodos:análise retrospectiva da documentac¸ão médica e exames de imagem, determinando-seacausadafalhadaAUJeomomentodesuaocorrência,assimcomoos componentesprotéticosimplantadosdurantearevisãoeanecessidadedeenxertiaóssea.
夽
Pleasecitethisarticleas:MozellaAdP,BackerRC,BorgesGonc¸alvesF,OsternoVasconcelosJ,deAraújoBarrosCobraHA.Revisãode artroplastiaunicompartimentaldejoelho:implantesusadosecausasdefalha.RevBrasOrtop.2014;49:154–159.
∗ Correspondingauthor.
E-mail:[email protected](A.d.P.Mozella).
Resultados: foramincluídosnestasérie27falhasderevisãodeAUJ(26pacientes).Colapso (afundamento)deumoumaiscomponentesrepresentouaprincipalcausadefalha, ocor-rendo em 33%dos pacientes,soltura assépticafoi identificado em 30%dos casos,por progressãodaosteoartroseem15%,infecc¸ãoedorem7%cada,desgastedopolietileno eosteóliseem4%cada.Falhaprecoceocorreuem41%detodasasindicac¸õesderevisõese falhatardiaem59%.Acirurgiaderevisãodaartroplastiaunicompartimentalfoirealizada em23pacientes.
Conclusões: em35%dascirurgiasderevisãofoinecessáriaenxertiaósseanoladotibial, sendotrêscasosnecessárioenxertohomólogodeBancodeTecidosMúsculoEsquelético. Nãoutilizamosaumentometálicoemnenhumcaso.Emumcasofoiimplantadoprótese semiconstritaporinstabilidade.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Unicompartmentalkneearthroplasty(UKA)wasintroduced into clinical practice for treating unicompartmental osteoarthrosisbyMcKeever,1whoperformedthefirstimplant
in1952.Attheendofthe1960s,Marmor2disseminatedthe
technique and it was subsequently advocated by Cartier etal.3
Overthecourseoftheseyears,thepopularityofthis tech-niqueand theenthusiasmforapplyingit oscillatedgreatly. Several short and medium-term studies published in the 1980s,whichcomparedtheclinicalandradiographicresults fromthistechnique,cametounfavorableconclusionsbecause theyfoundthattheresultswerenotreproducibleandthere wasahighfailurerate,inrelationtototalkneearthroplasty (TKA).2,4–6
Overthelastdecade,theadventoftheconceptsof mini-mallyinvasivesurgerytogetherwithevolutionoftherigorof patientselectionanddevelopmentandrefinementofsurgical techniquesandimplantdesignhaveledtofavorableevolution oftheclinicalresultsand,consequently,renewedinterestin UKA.7,8
Recentlypublishedstudies,withmediumand long-term follow-up, which evaluated unicompartmentalarthroplasty usingmodern implants in properly selected patients, have confirmedthesegoodandexcellentresultsandhave demon-strateddurabilitycomparabletothatofTKA.9–12
AlthoughUKAisatherapeuticmethodofproven effective-nessandsafety,itmayleadtoeitherearlyorlatefailurewith unsatisfactoryresultsinafewcases.13,14Intheinitialseries
reportedbyMarmor,2 withfirst-generationimplants,
reope-rationwasnecessaryin35%ofthecases.Studiesanalyzing modernimplantshaveidentifiedratesofconversiontoTKA rangingfrom6%to8%.15–17
PreservationofthebonestockincasesoffailureofUKA theoreticallymakesconversiontoconventionaltotal arthro-plastypossible.Thus,therewouldnotbeaneedformetallic expanders,intramedullarynails,bonegraftsorincreased con-strictionoftheimplants.18,19
However,severalauthorshavequestionedthepossibility ofconvertingTKAwithouttheneedformetallicexpanders, intramedullarynailsorbonegrafts.20–24
The aims of the present study were to determine the causesoffailureofUKAinpatientswhounderwentrevision
atasinglehospitalinstitutionandtoidentifytheimplants usedandthepossibleneedforbonegrafting.
Materials
and
methods
Themedicalfiles ofpatients who underwent UKArevision surgeryattheKneeSurgeryCenteroftheNationalInstituteof TraumatologyandOrthopedics(InstitutoNacionalde Trauma-tologiaeOrtopedia,INTO)betweenJanuary1990andJanuary 2013wereanalyzed.
Thisstudy wasfirstlysubmittedtoandapprovedbythis institution’sResearchEthicsCommittee.
Aretrospectiveanalysiswasconductedonthemedicalfiles andthecauseofUKAfailureandtimeofitsoccurrencewere determined,alongwiththeprostheticcomponentsimplanted duringtheUKArevisionandanyneedforbonegrafting.
Demographicdataweregatheredandthepatients’ histo-ries,preoperativephysicalexaminations,laboratorytestsand imagingexaminationswereevaluated,alongwiththe surgi-caldescriptionsandfindingsfromtheoperation.Inaddition, informationobtainedfromculturesonfluidsandtissueswas analyzed.
UKA revision was defined as any surgical procedure performed subsequent to unicompartmental arthroplasty in which prosthetic components were removed, added or exchanged.
UKAfailureswerecategorizedinconformitywithcurrent conceptsintheliterature,asduetomechanical,septicor dis-easeprogressionfactors,incompartmentsthathadnotcome backtothesurface.
Mechanical failure of UKA was defined as situations in whichalterationstooneormorecompartmentsoccurred, cul-minatinginimposinglimitationsonthe functioningofthe prostheticdeviceand,consequently,limitationsontheclinical results.
Failures due to mechanical alterations were subdivided intolooseningofoneormorecomponentsoftheprosthetic device,worn-outpolyethylene,migrationorcollapseofoneor morecomponents,instabilityandperiprostheticfractures.
Diagnosesofinfectionwereprovenbasedonthecriteria establishedbytheCentersforDiseaseControlandPrevention (CDC),intheUSA.25
clinicalmanifestationsofpainandfunctionallimitationthat incapacitatedtheindividualwithregardtoactivitiesofdaily living,wereconsideredtobeUKAfailuresandindicatedthe needforconversiontoTKA.Manifestationsofthisnaturewere provenbymeansofradiographicexaminationswith weight-bearing,whentheseshowedseveredegenerativealterations incompartmentsthathadnotcomebacktothesurface.
In chronological terms,failures were divided into early, whentheyoccurrednotmorethan twoyearsafterUKA,or late,whentheyoccurredafterthistime.
Datarelatingtotheimplantusedduringtheunicondylar arthroplastyprocedureandtherevisionsurgeryweregathered fromthesurgicalreport.
Theunicompartmental implants usedwere the Omnifit implant (Stryker®) with a first-generation cemented fixed
metallicplatformandtheMillerGalanteimplant(Zimmer®)
withthesamespecifications,ofsecondandthirdgenerations. Theimplantsusedduringtherevisionsurgerywerepart ofthe PFC Sigma DePuy® system and were categorized as
primaryconventionalorsemi-constricted(TotalCondylarIII DePuy®).
Likewise,we analyzedoccurrences ofbonedefects that mayhaveexistedandhowtheyweremanaged:bonegrafting, with discrimination between autologous and homologous; andalsouseofwedge-likemetallicexpanders,withorwithout associatedintramedullarynails.
Results
Twenty-sevenUKA revisionsurgeries wereincluded inthis series (26 patients). Ten patients were male and 17 were female.Theiragesatthetimeoftheconversionprocedureon theUKArangedfrom45to78years,withameanof64.8years. Thefailureofthe unicompartmentalarthroplasty occurred onthe right sidein14 patientsand on theleft side in13. In25patients,theunicompartmentalarthroplastyhadbeen performedatINTOandinonecase,atanotherinstitution.
ThemostprevalentetiologyforUKAwas unicompartmen-talosteoarthrosis,inthecasesof14patients(52%),followedby osteonecrosisofthemedialfemoralcondylein11cases(41%), whileUKAwaspost-traumaticintwocases(7%).
Unicondylar arthroplasty was performed in the medial compartmentin22patientsandinthelateralcompartment infive.
Inevaluatingthetotalsampleof27UKAfailures,collapse (sinking)ofoneormorecomponentswasthemaincauseof failure,in33% ofthepatients (ninecases).Aseptic loosen-ing wasthe second mostfrequentcause offailure, in30% ofthecases(eight patients).These werefollowed,inorder ofprevalence,bythefollowingothercauses:progressionof osteoarthrosisin15%(fourpatients),infectionandpainin7% each(twopatients)andworn-outpolyethyleneandosteolysis in4%each(onepatient).
Casesoflooseningofonlyonecomponentoccurredmore frequentlyonthetibialside(60%)(Fig.1).
EarlyfailureoftheUKAoccurredin11cases,which rep-resented41%ofalltheindicationsforrevisionmadeduring theperiodstudied.Latefailureoccurredin16casesand cor-respondedto59%.
Collapse/sinking Aseptic loosening Progression of arthrosis Infection
Pain
Worn-out polyethylene
Fig.1–DistributionofthecausesofUKAfailure(n=27).
Collapse/sinking Infection Pain
Progression of arthrosis Aseptic loosening
Fig.2–DistributionofearlycausesofUKAfailure(n=11).
Themaincauseofearlyfailurewascollapse/sinkingofthe tibialcomponent,in45.5%ofthecases(fivetimes).Thiswas followedbyinfectionandpain,in18.25%ofthepatients(two cases),amongothercausesinsmallernumbers.Progression ofthearthrosisandlooseningofthefemoralcomponentwere identifiedasthecauseofrevisionin9%each(onecase)(Fig.2). Themaincauseoffailureinthegroupwithrevisionafter morethan twoyears(16patients)wasasepticlooseningof oneormorecomponents,in44%(sevencases).Thiswas fol-lowedbycollapse/sinkingofoneormorecomponentsin25% each(fourcases)andprogressionoftheosteoarthrosisin19% (threepatients).Worn-outpolyethyleneandosteolysiswere identifiedin6%each(onecase).
In the casesofloosening or migrationofasingle com-ponent,this occurredonthetibialsidein75%ofthecases (Fig.3).
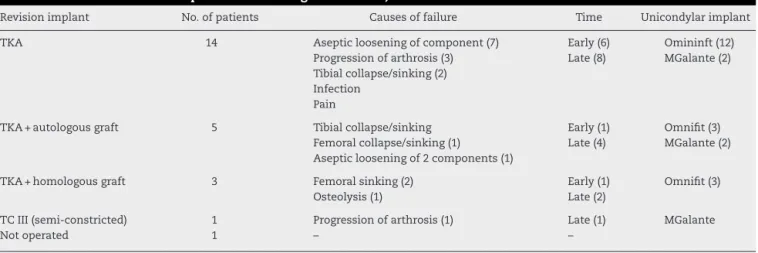
Revision surgeryonunicompartmentalarthroplasty was performedon23patients.Detailedanalysisontheimplants usedandtheneedforgrafts,alongwiththetimeandcauseof failure,isshowninTable1(Fig.4A–D).
Discussion
Manystudieshaveanalyzeddetailsofthesurgicaltechnique forUKAandimplantsavailable,andtheclinicalresults. How-ever, studies reporting the causes and chronology ofthese failures,alongwiththeimplantsneededduringtherevision surgery,arerareintheliterature.4–14
Despite thelow incidenceoffailureofmodern unicom-partmentalarthroplasty,thepersonalimpact,expenditureof financialresourcesandincidenceofmorbidityandmortality
Aseptic loosening Sinking
Progression of arthrosis Osteolysis
Worn-out polyethylene
Table1–Distributionoftheimplantsusedduringtherevision,numbersofcasesandtimeandcauseoffailure.
Revisionimplant No.ofpatients Causesoffailure Time Unicondylarimplant
TKA 14 Asepticlooseningofcomponent(7) Early(6) Omininft(12)
Progressionofarthrosis(3) Late(8) MGalante(2) Tibialcollapse/sinking(2)
Infection Pain
TKA+autologousgraft 5 Tibialcollapse/sinking Early(1) Omnifit(3)
Femoralcollapse/sinking(1) Late(4) MGalante(2) Asepticlooseningof2components(1)
TKA+homologousgraft 3 Femoralsinking(2) Early(1) Omnifit(3)
Osteolysis(1) Late(2)
TCIII(semi-constricted) 1 Progressionofarthrosis(1) Late(1) MGalante
Notoperated 1 – –
relatingtorevisionproceduresmakeitnecessaryforsurgeons toseek tounderstandthe mechanisms thatlead to occur-rencesoffailure,sothatthesecausescanbepreventedand corrected.13–16
Data from the Swedish arthroplasty register, in which approximately15,000unicondylarimplants wereevaluated, showedthatfailurewithaneedforrevisionoccurredin7.7% ofthepatients.Asepticlooseningwasidentifiedasthemain failuremechanism,in43%oftherevisions.Progressionofthe osteoarthrosiswasresponsiblefor26%ofthecasesofrevision andwasthesecondmostprevalentcause.Worn-out polyeth-ylene,mechanicalfailuresandfracturesrepresented15%of theproceduresforconversiontoTKA.15
Ourstudyanalyzedsurgicalproceduresperformedusing first,secondand third-generationimplants andatdifferent timesduringthedevelopmentofknowledgeofthistechnique. Thus,itincludedsomepatientswhounderwentprocedures with characteristics that do not express today’s level of
Fig.4–(A–D)Failureofunicompartmentalarthroplasty revisedusingasemi-constrictedimplant.
technological development. Thus, the typesof failure may havepresentedchangesover thecourseofdevelopmentof thetechnique.
Inourseries,componentmigrationwithsinking/collapse ofthecompartmentwasthemaintypeoffailure,in33%of our sample. Most ofthe cases occurred in the tibial com-ponent.Ourdataareconcordantwiththoseofthestudyby Aletoetal.,23inwhichtibialcollapsewasidentifiedin47%
ofthecasesofrevisionandalsorepresentedthemost preva-lentcause.However,thiscausediffersfromthemainfailure mechanismidentifiedinlargerseries.13–15,20–26
In the Swedish register15 and Norwegian register,26
col-lapsewithsinking ofthe componentoccurred inlessthan 10%ofthesample.However,asepticlooseningwasthemain causeoffailure,inapproximately40%ofthecases.
Inourstudy,asepticlooseningofoneormorecomponents wasthesecondmostprevalentcause,andwasidentifiedin 30%oftherevisionsurgicalprocedures.Inanalyzingaseries with15yearsofsurvival,Foranetal.16didnotidentify
asep-ticlooseningasacauseoffailureintheirsample.However, Saragagliaetal.27identifiedasepticlooseningin67%oftheir
sample.
Several authors,suchasFroimsonet al.6and Saragaglia
et al.,27 highlighted progression of osteoarthrosis in
com-partments that that had not come back to the surface as frequentalterationsinradiographicexaminationsfollowing unicompartmentalarthroplasty, witharange ofoccurrence from17%to60%.However,theneedforrevisionduetothis cause was 3–12%. In our series, 15% ofthe indicationsfor revisionofaunicompartmentalprosthesisoccurred dueto functionallimitationscausedbyprogressionof osteoarthro-sis.
Froimsonetal.6emphasizedthatinfectionmaybeanearly
cause offailureormay occurlater onandaffect asmaller numberofcases(notmorethan10%).Inoursample,infection wasresponsibleforrevisionintwopatients(8%),duringthe earlyperiodinbothcases,whichisthereforeconcordantwith thedataintheliterature.
Itwasnotedthataworn-outpolyethylenecomponentwas thereasonforrevisioninonlyonepatientinourseries. There-fore,ourdataarenotconcordantwiththoseofthestudiesby Springeretal.14andLevineetal.22Webelievethatpartofthis
andsterilizationofpolyethylenecomponentsfromdifferent manufacturersduringtheinitialperiodofdevelopmentofthe technique.
UKAhasthetheoreticaladvantageofbeingtechnicallyeasy torevise,withlimitedbonelossesandwithoutligament insuf-ficiency,whichenablesconversiontoTKAwithconventional implants.However,severalauthorshaveidentifiedneedsfor bonegrafting,metallicexpandersand intramedullarynails, and to a lesser extent, a need for implantation of semi-constrictedprostheses.20,27–29
Barretetal.20studiedfailuresinfirst-generation
unicondy-lararthroplastyproceduresandfoundthatthecauseofthe revisionwasasepticlooseningofcomponentsin55%ofthe cases and progression of osteoarthrosis in 31%. Out of 29 conversionstototalprostheses,93%weretoimplantsthat pre-servedtheposteriorcruciateligament(PCL).However,more thanhalfoftheseriesrequiredbonegrafts,metallicexpanders ornails.Thedifficultieswere attributedtounderdeveloped implant designand limitations relating toselection ofthe patientswhounderwentUKA.
In a series published by Padgett et al.,21 bone defects
requiring treatment were identified in 76% of the surgical procedures. These authors classified revision of unicom-partmentalprosthesesasaprocedureoftechnicaldifficulty similartothatofTKArevision.
Amongrevisionsof31second-generation unicompartmen-tal arthroplasty procedures publishedina study byLevine etal.,22defectsthatcouldbedealtwithusingautologousgrafts
were identifiedin23%ofthe cases,while19%ofthe bone defectshadtobemanagedusingmetallicexpandersandthree patientsrequiredanintramedullarynail.Alltherevisionshad beenindicatedduetoworn-outpolyethyleneorprogression ofarthrosis.
Astudyonconversionof32modernunicondylarimplants conductedbyMcAuleyetal.24showedthattherewasaneed
forautologousbonegraftsin31%,whilein25%ofthecases thedefect wasmanagedusing ametallicexpander and,in 44%,implantswiththeadditionofanintramedullarynailwere needed.
Springeretal.14highlightedthat68%ofthepatientswho
underwent conversion of third-generation UKA presented bonedefectswithaneedformanagementusingautologous bonegrafts,whilemetallicexpanderswereusedin23%.Chou etal.28corroboratedthesedataandfoundintheirseriesthat
autologousbonegraftswereusedin67%ofthecases,while metalwedgeswereusedasfillersin33%.
Inoursample,61%oftherevisionsurgerieswereperformed usingconventionalimplantsandwithouttheadditionofbone grafts.Thebonedefectswereconcentrated inthetibiaand requiredautologousgraftingin22%ofthesurgicalprocedures (fivecases)andhomologousgraftingin13%(threecases). Man-agementofbonedefectsusingmetallicexpanderswas not observedinourstudy.
Aletoetal.23andSpringeretal.14highlightedthatthetype
offailurewasapredictivefactorforabonedefectduringthe revisionsurgery.Thiswasproveninourseries,inwhich migra-tionorcollapseofthemedialcompartmentmorefrequently ledtoaneedforbonegrafting.
Severalauthors, suchasAleto etal.,23 McAuley etal.,24
Springeretal.14andLaietal.,18didnotidentifyanyneedfor
homologousgraftingformanagingbonedefects.However,as notedinourstudy,useoftissuebankgraftswasalsoidentified bySaldanhaetal.13andOtteetal.,29in6%and69%oftheir
surgicalprocedures,respectively.
Inourseries,aneedforanimplantwithagreaterdegreeof constrictionwasseeninthecaseofonepatient(5%)who pre-sentedprogressionofosteoarthrosisinalateralcompartment, associated with valgus deformity and insufficiency of the medialstructures.InthestudybySaldanhaetal.,13although
theanteriorcruciateligamentwasintactin77%oftheir sam-ple, semi-constricted implants were needed in 22% of the casesbecause ofinsufficiencyofthe medialcollateral liga-ment.
Conclusions
Weidentifiedthe followingascauses offailure of unicom-partmental arthroplasty: collapse (sinking) ofone or more components,in33%ofthepatients;looseningin30%; progres-sionofosteoarthrosisin15%;infectionandpainin7%each; andworn-outpolyethyleneandosteolysisin4%each.
Aneedforbonegraftingwasseenin35%ofthepatients. No metallic expanders or intramedullary nails were used, althoughasemi-constrictedimplanthadtobeusedinone casebecauseofligamentinsufficiency.
Thecauseoffailurewasrelatedtotheneedforbone graft-ing.Amongthe eightpatientswhoneededbonegrafts,the failure mechanism wasmigration/collapse ofthe compart-mentinsixcases.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.McKeeverDC.Thechoiceofprostheticmaterialsand evaluationofresults.ClinOrthop.1995;6:17–21.
2.MarmorL.Unicompartmentalarthroplastyofthekneewitha minimumten-yearfollow-upperiod.ClinOrthopRelatRes. 1988;228:171–7.
3.CartierP,ChaibS,VanvoorenP.Unicompartmentalprosthetic replacementoftheknee.Aproposof159casesmaximum follow-upof10years.RevChirOrthop.1987;73:130–3. 4.LaskinRS.Unicompartmentaltibiofemoralresurfacing
arthroplasty.JBoneJointSurgAm.1978;60:182–5. 5.InsallJ,AgliettiP.Afive-sevenyearfollow-upunicondylar
arthroplasty.JBoneJointSurgAm.1980;62:1329–37. 6.FroimsonMI,BloomfieldMR,ShermanRA.Revisionofthe
failedunicompartimentalkneearthroplasty.Semin Arthroplasty.2009;20:23–8.
7.GioeTJ,KillenKK,HoeffelDP,BertJM,ConfortTK,Schetelma K,etal.Analysisofunicompartimentalkneearthroplastyina community-basedimplantregistry.ClinOrthopRelatRes. 2003;416:111–9.
9. BiswalS,BrightonRW.Resultsofunicompartimentalknee arthroplastywithcemented,fixed-bearingprosthesisusing minimallyinvasivesurgery.JArthroplasty.2010;25(5):721–7. 10.CamanhoGL,ViegasAC,CamanhoLF,CamanhoCR,ForgasA.
Artroplastiaunicompartimentalnotratamentoda osteoartrosemedialdojoelho.RevBrasOrtop. 2007;42(9):285–9.
11.NewmanJ,PydisettyRV,AckroydC.Unicompartmentalor totalkneearthroplasty.JBoneJointSurgBr.2009;91-B: 52–7.
12.BorusT,ThornhillT.Unicompartmentalkneearthroplasty. JAAOS.2008;16(1):9–18.
13.SaldanhaKAN,KeysGW,SvardUCG,WhiteSH,RaoC. RevisionofOxfordmedialunicompartmentalknee arthroplastytototalkneearthroplasty–resultsofa multicentrestudy.Knee.2007;14:
275–9.
14.SpringerBD,ScottRD,ThornhillTS.Conversionoffailed unicompartimentalkneearthroplastytoTKA.ClinOrthop RelatRes.2006;446:214–20.
15.LewoldS,RobertssonO,KnutsonK,LidgrenL.Revisionof unicompartmentalkneearthroplasty:outcomeof1,135cases fromtheSwedishKneeArthroplastystudy.ActaOrthop Scand.1998;69:469–74.
16.ForanJR,BrownNM,DellaValleCJ,BergerRA,GalanteJO. Long-termsurvivorshipandfailuremodesof
unicompartimentalkneearthroplasty.ClinOrthopRelatRes. 2013;471:102–8.
17.SteeleRG,HutabaratS,EvansRL,AcroydCE,NewmanJH. SurvivorshipoftheStGeordSledmedialunicompartimental kneereplacementbeyondtenyears.JBoneJointSurgBr. 2006;88:1164–8.
18.LaiCH,RandJA.Revisionoffailedunicompartmentaltotal kneearthroplasty.ClinOrthopRelatRes.1993;287: 193–201.
19.BerendKR,GeorgeJ,LombardiAV.Unicompartmentalknee arthroplastytototalkneearthroplastyconversion:assuringa primaryoutcome.Orthopedics.2009;32(9):684.
20.BarretWP,ScottRD.Revisionoffailedunicondylar unicompartmentalkneearthroplasty.JBoneJointSurgAm. 1987;69(9):1328–35.
21.PadgettDE,SternSH,InsalJN.Revisiontotalknee arthroplastyforfailedunicompartimentalreplacement.J BoneJointSurgAm.1991;73A(2):186–90.
22.LevineWN,OzunaRM,ScottRD,ThornhillTS.Conversionof failedmodernunicompartimentalarthroplastytototalknee arthroplasty.JArthroplasty.1996;11(7):797–801.
23.AletoTJ,BerendME,RitterMA,FarisPM,MeneghiniRM.Early failureofunicompartimentalkneearthroplastyleadingto revision.JArthroplasty.2008;23(2):159–63.
24.McAuleyJP,EnghGA,AmmeenDJ.Revisionoffailed unicompartimentalkneearthroplasty.ClinOrthopRelatRes. 2001;392:279–382.
25.GarnerJS,JavisWR,EmoriTG,HoranTC,HughesM:.CDC definitionsfornosocomialinfections.In:OlmstedRN,editor. APICinfectioncontrolandappliedepidemiology:principles andpractice.St.Louis:Mosby;1996.p.A-1–20.
26.FurnesO,EspehaugB,LeiS.Afterunicompartimentaland tricompartmentalprimarykneereplacementwithcement.J BoneJointSurgAm.2007;89:519–25.
27.SaragagliaD,EstourG,NemerC,CollePE.Revisionof33 unicompartmentalkneeprosthesesusingtotalknee arthroplasty:strategyandresults.IntOrthop.2009;33:969–74. 28.ChouDTS,SwamyGN,LewisJR,BadheNP.Revisionof
implantconstraintonresultsofconversionof unicompartimentalkneearthroplastytototalknee arthroplasty.Orthopedics.2002;25:1353–7.