SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Reproducibility
assessment
of
different
descriptions
of
the
Kellgren
and
Lawrence
classification
for
osteoarthritis
of
the
knee
夽
Felipe
Borges
Gonc¸alves,
Felipe
Almeida
Rocha,
Rodrigo
Pires
e
Albuquerque
∗,
Alan
de
Paula
Mozella,
Bernardo
Crespo,
Hugo
Cobra
InstitutoNacionaldeTraumatologiaeOrtopedia,CentrodeCirurgiadoJoelho,RiodeJaneiro,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received19January2016 Accepted15February2016 Availableonline25October2016
Keywords: Knee Radiography Classification
a
b
s
t
r
a
c
t
Objective:Toassesstheinter-andintraobserverreproducibilityoftheoriginalversionand differentdescriptionsoftheKellgrenandLawrenceclassificationusedinepidemiological studiesforosteoarthritisoftheknee.
Methods:Thestudyincluded72patientswithosteoarthritisoftheknee.Threemedical mem-bersoftheBrazilianSocietyofKneeSurgerywereinvitedtoevaluatetheimages.An intra-andinterobserveranalysiswasconducted,withanintervalofonemonth.Theintraobserver agreementwasanalyzedusingtheweightedCohen’sKappacoefficient.Theinterobserver agreementwasanalyzedusingtheKrippendorffalphacoefficient(˛).
Results:The intraobserverassessmentindicated conflictingresults. Intheinterobserver analysis,thelevelofagreementwassuperficial.
Conclusions: TheclassificationofKellgrenandLawrenceanditsvariantsgeneratedalow reproducibilitybetweenobservers.Theintraobserveranalysisshowedalackofuniformity intheuseofthisclassificationanditsvariants,evenamongexperiencedobservers.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Avaliac¸ão
da
reprodutibilidade
das
diferentes
descric¸ões
da
classificac¸ão
de
Kellgren
e
Lawrence
para
osteoartrite
do
joelho
Palavras-chave: Joelho Radiografia Classificac¸ão
r
e
s
u
m
o
Objetivo:Avaliarareprodutibilidadeintereintraobservadordaversãooriginaledas difer-entesdescric¸õesdaclassificac¸ãodeKellgreneLawrenceusadasemestudosepidemiológicos paraosteoartritedojoelho.
Métodos:Foramestudados72pacientescomdiagnósticodeosteoartritedojoelho.Três médi-cosmembrosdaSociedadeBrasileiradeCirurgiadoJoelhoforamconvidadosparaavaliar
夽
StudyconductedattheKneeSurgeryCenter,InstitutoNacionaldeTraumatologiaeOrtopedia(Into),RiodeJaneiro,RJ,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](R.P.Albuquerque).
http://dx.doi.org/10.1016/j.rboe.2016.10.009
asimagens.Análisesintraeinterobservadorforamfeitascomintervalodeummês.A con-cordânciaintraobservadorfoianalisadapormeiodocoeficienteKappadeCohenponderado. NaanáliseinterobservadorfoiusadoocoeficientealphadeKrippendorff(␣).
Resultados: Aavaliac¸ãointraobservadorapresentouresultadosdiscordantes.Na análise interobservador,ograudeconcordânciafoisuperficial.
Conclusões: Aclassificac¸ãodeKellgreneLawrenceesuasvariantesgeraramumabaixa reprodutibilidadeentreosobservadores.Aanáliseintraobservadorapresentouresultados discordantes,demonstrouqueháfaltadeuniformidadenousodessaclassificac¸ãoedesuas variantesmesmoentreobservadoresexperientes.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Osteoarthritisisoneofthemostcommondiseasesworldwide, withnodistinctionorethnicpreference.1Theknee,beinga load-bearingjoint,isafrequentinvolvedsite.1
Theradiologicalevaluationisparamountinpatientswith osteoarthritisoftheknee. Intheradiographicstudy,oneis abletogradetheseverityofjointinvolvement,measurethe axis,assessligamentinstabilityorboneloss,andalsoindicate thetypeoftreatment,aswellasthenecessaryimplantwhen surgeryisneeded.
The Kellgrenand Lawrence grading is the most widely used classificationforknee osteoarthritis when X-raysare assessed2; however,five versionsofthis classificationhave beendescribedinepidemiologicalstudies.2
Inordertobereproducible,aclassificationshouldbe sim-ple,easytoremember,andhelpfulinguidingtreatmentand definingtheprognosisoftheseinjuries.3Acharacteristicthat mustbepresentinanyclassificationisreproducibility.3
Thisstudyaimedtoassesstheinterobserverand intraob-server reproducibility of the original version and of the differentvariantsoftheKellgrenandLawrenceclassification usedinepidemiologicalstudiesforosteoarthritisoftheknee.
Material
and
methods
Thestudy was presentedindetail toand approvedbythe EthicsCommitteeunderCAAENo.31378714.6.0000.5273.All participantssignedainformedconsentpriortoenrollment. Theywerealsoofferedafinancialincentivetoparticipate.
In this hospital’s outpatient clinic, 200 patients with osteoarthritisofthekneewereselected.Therewasnoage lim-itation.Exclusioncriteriawere:patientswhounderwentprior surgicalproceduresinthekneetobeassessedorwho under-wentjointreplacementonthecontralateralknee,aswellas patientswithotherrheumatologicdiseases.Afterapplyingthe exclusioncriteria,72patientsandtheirradiographicstudies wereselectedtocomprisethesample.
Thestudyconsistedofthreeobservers,membersofthe BrazilianSocietyofKneeSurgeryandpartofthehospitalstaff, whoconductedtheradiographicanalysis.
Knee radiographs in anteroposterior (AP) with bipedal load,lateral,axialpatellarat30◦,andRosenbergviewswere
obtainedfromallpatients,followingastandardprotocol.The APviewwas madewiththe kneeinextensionand bipedal support.Thetube-filmdistancewas1m,andtheradiuswas centeredatthelowerpoleofthepatella.Thelateralviewwas achievedwiththekneein20◦offlexionwithpatientstanding;
thetube-filmdistancewas1m.Rosenbergviewwasmadein posteroanterior(PA),underloadand45◦offlexion.Feetwere
positionedparallelandalignedforward.Thepatellatouched thefilm.X-rayswerecenteredattheleveloftheinferiorpole ofthe patella,withacraniocaudalinclinationof10◦ anda
tube-filmdistanceof1m.
AShimatzoX-raydevice,ratedat50kVand40mA,was used. The exams were overseen by the main investigator regardingimagequalityandwere repeatedifconsideredof poortechnicalquality; patientpositioning,knee, andX-ray deviceangulationwerealsoobserved.Anglesweremeasured withagoniometer.
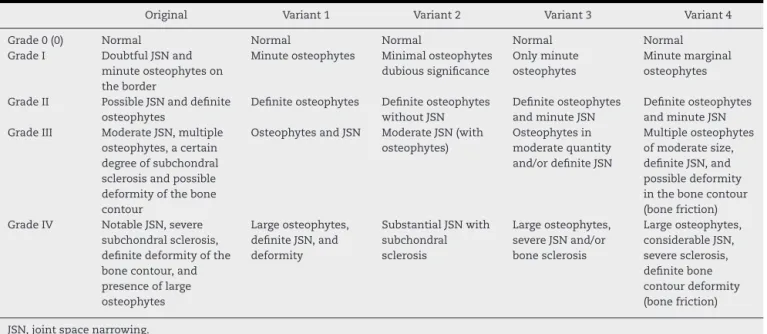
Scanned images were delivered on a CD-ROM to the observers.Inordertominimizebiasduetothedifficultyof interpretationorpossibleforgetfulness,theclassificationand itsvariantsaredescribedinTable1.
Radiographic analyses were performed blindly on two occasions,withaone-monthinterval,andtheinterpretations ofthethreeobserverswerescannedforsubsequentstatistical analysis.
DatawereanalyzedwithstatisticalanalysissoftwareR ver-sion3.1.0,andSPSS(StatisticalPackagefortheSocialSciences) version22.0.Theintraobserveragreement,whichcompared bothassessmentsfromthesameobserverforeachofthefive classifications,wasanalyzedbytheweightedCohen’sKappa coefficient.
TheweightedCohen’sKappacoefficientrangesfrom−1to
1;valueslessthanorequalto0representnoagreementand 1representstotalagreement.Inthisstudy,theclassification adoptedwastheoneproposedbyByrt,4asdescribedinTable2. Thecoefficientswerecalculatedusingthe“psy”packageofR. Intheinterobserver analysis,anothermeasureof agree-mentwasused,Krippendorf’salphacoefficient(˛).Therating
oftheagreement,giventhevalueof˛,wasthesameasthat
Table1–Classificationanditsvariants.
Original Variant1 Variant2 Variant3 Variant4
Grade0(0) Normal Normal Normal Normal Normal
GradeI DoubtfulJSNand minuteosteophyteson theborder
Minuteosteophytes Minimalosteophytes dubioussignificance
Onlyminute osteophytes
Minutemarginal osteophytes
GradeII PossibleJSNanddefinite osteophytes
Definiteosteophytes Definiteosteophytes withoutJSN
Definiteosteophytes andminuteJSN
Definiteosteophytes andminuteJSN GradeIII ModerateJSN,multiple
osteophytes,acertain degreeofsubchondral sclerosisandpossible deformityofthebone contour
OsteophytesandJSN ModerateJSN(with osteophytes)
Osteophytesin moderatequantity and/ordefiniteJSN
Multipleosteophytes ofmoderatesize, definiteJSN,and possibledeformity inthebonecontour (bonefriction) GradeIV NotableJSN,severe
subchondralsclerosis, definitedeformityofthe bonecontour,and presenceoflarge osteophytes
Largeosteophytes, definiteJSN,and deformity
SubstantialJSNwith subchondral sclerosis
Largeosteophytes, severeJSNand/or bonesclerosis
Largeosteophytes, considerableJSN, severesclerosis, definitebone contourdeformity (bonefriction)
JSN,jointspacenarrowing.
Table2–Kappacoefficientvalues(K)andagreement classification.
K-value Concordancerating
−1to0.00 None
0.0to0.20 Poor
0.21to0.40 Superficial 0.41to0.60 Reasonable
0.61to0.80 Good
0.81to0.92 Verygood
0.93to1.0 Excellent
Results
Table3showsthevaluesoftheweightedKappacoefficient (K)anditsconfidenceinterval(CI)at95%confidence,which assesses the intraobserver agreementof each observer for eachoftheratings.ThevaluesindicatethatObserver1 pre-sented a “superficial”agreement between first and second observationfortheoriginalclassificationandforallits vari-ants, with Kappa values equal to 0.34 or 0.35. Observer 2 presenteda “very good” agreement betweenfirst and sec-ondobservationfortheoriginalclassificationandforallits variants,withKappa valuesbetween0.85and 0.92.Finally, Observer3showedan“excellent”agreementbetweenfirstand secondobservationfortheoriginalclassificationandforall variants,withKappavaluesequalto0.97forvariants1and4
andperfectagreement(K=1)betweenthetwoevaluationsin theoriginalclassificationandinvariants2and3.
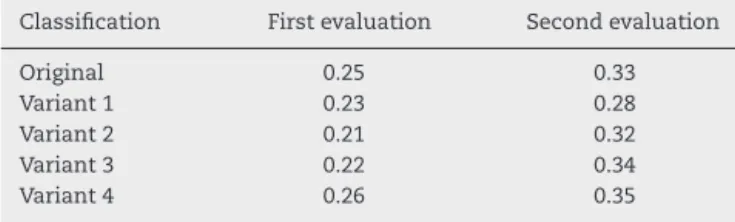
Table 4showsthe valuesofKrippendorff’s alpha coeffi-cient,whichwasusedtoassessinterobserveragreement,in thefirstandsecondevaluation,foreachoftheratings. Val-ues showthat, bothinthe first andsecond evaluation,for all ratings, theagreement betweenobservers was “superfi-cial”. Itisnoteworthythattheagreementwaslower inthe firstevaluation.
Discussion
Classifying diseases is a common practice. A good rating system isdesigned tobe simple,reproducible,and able to group different stages of a lesion into homogeneous sub-groups,allowingforcomparisons,treatmentalgorithms,and prognosis.3Whatusuallyhappensisthatonceaclassification foraparticularinjuryisestablished,basedonarelevantand representativesample,acasethatdoesnotfitthedescribed or classifiedtypesappears.5 Weber,inhisstudyof malleo-larfractures,reservedasubgroupfor“unclassifiable”injuries, i.e.,thosethat,duetotheirpeculiarity,couldnotbefittedinto classesorgroups.5Overtime,someratingshavebeenreplaced bymorecompleteones.
Intheliterature,thereisstillnoconsensusonwhich clas-sification should beused for the study ofosteoarthritis of the knee. Weidow et al.6 reported that knee radiographic
Table3–WeightedKappacoefficientsoftheintraobserveragreementbetweenthefirstandthesecondevaluation,for eachclassification.
Observer Classification
Original Variant1 Variant2 Variant3 Variant4
Table4–Krippendorff’salphacoefficientofthe interobserveragreementinthefirstandsecond evaluationforeachclassification.
Classification Firstevaluation Secondevaluation
Original 0.25 0.33
Variant1 0.23 0.28
Variant2 0.21 0.32
Variant3 0.22 0.34
Variant4 0.26 0.35
classificationsmust bereviewedandimprovedthroughthe examinationtechniqueormethodemployed.Sunetal.,7 in areviewstudyof16classificationsforosteoarthritisofthe knee,concludedthattherewasnounanimouschoiceamong thevariousmedicalspecialties.TheKellgrenandLawrence classification8valuesthepresenceorabsenceofosteophytes. Incontrast,theAhlbäck9classificationassessesreductionof thejointspace;somestudiesconsiderittobethebestmethod foranalyzingprogressionofosteoarthritis.10,11Studiesassuch as that by Danielsson and Hernborg12 demonstrated that osteophytes did not change over 16 years of evolution. In turn,Kijowskietal.13concludedthatosteoarthritisoftheknee shouldbediagnosedbymarginalosteophytes.Infact,itisthe progressionofthediseasethatmustbeassessedbyjointspace narrowing, subchondralsclerosis, and subchondral cysts.12 Felsonetal.14observedthatosteophytesareassociatedwith pooralignmentoftheipsilaterallowerlimb.Pooralignmentis apowerfulriskfactorfortheprogressionofosteoarthritis.14 Thepresentstudy usedthe KellgrenandLawrence8 classi-fication,asit isroutinelyusedbyorthopedicsurgeonsand rheumatologists.
Albuquerque et al.3 observed that the Kellgren and Lawrence8 classificationhadlower levelofagreementon a intra-andinterobserveranalysisofthreedifferent classifica-tions:those byDejouret al.,15 Ahlbäckapud Keyesetal.,10 andKellgrenandLawrence.8Thepresentresearchconfirms thepoorresultsoftheKellgrenandLawrenceclassification.8 Rodrigues et al.16 analyzed the interobserver reproducibil-ityoftheoriginalKellgrenandLawrenceclassification8and didnotobserveastatisticallysignificantdifferencebetween kneespecialistsandgeneralorthopedists.Furthermore,they observedaregularKappacoefficientindex.Thepresentstudy performedanintra-andinterobserveranalysisandattempted toachieveamoreaccurateassessmentwhencomparedwith studiessuchasthosebyRodriguesetal.16
Theliteraturefeaturessomestudiescomparingthe Kell-grenandLawrenceclassification8anditsdifferentvariants.2,17 However,noneofthese studiesused aradiographic analy-sisdescribedbyRosenbergetal.18norincludedpatientswith advancedstagesofosteoarthritisoftheknee.Forthisreason, thepresentresearchincludedthesetwovariables,thus rep-resentinganunprecedentedandextremelyimportantstudy. SomestudiesindicatethattheRosenbergviewprovidesa bet-terevidenceofjointwear.18,19 Furthermore,authors believe that,foraclassificationtobeassessedaccurately,itmust fea-turethepathologystudiedinitsvariousgrades.
Villardi et al.20 and Galliet al.21 observeda low degree ofinterobserveragreementintheuseofAhlbäck classifica-tionmodifiedapudKeyesetal.10Thepresentstudy,although
usingadifferentclassificationsystem,alsoobservedaweak agreementamongobservers.
Theobserversofthepresentresearchareexperienced spe-cialistsinkneesurgery;inordertoreproduceamoreaccurate assessment,aresponsetimewasnotstipulated.21,22 Vilalta etal.23foundthatexperiencedobserversgenerated individ-ualvariabilityandcauseddifferencesinresultsandconfusion in the literature, a belief that the authors of the present studyprovedanddefend.Brandtetal.24andKijowskietal.,25 when assessing patientswith osteoarthritis,compared the AP view in loaded knee extension with arthroscopic find-ings. They emphasize that, in patients withosteoarthritis, theassessmentofjointspaceandosteophytesarenot suit-ableparametersforanalyzingthedisease.Theysuggestthat furtherresearchshouldbeconductedinordertofinda com-plementary test with betteraccuracy. Thepresent authors believe that knee arthroscopy is an excellent therapeutic method,butitisaninvasiveprocedureand,therefore,should notbeusedasadiagnosticmethod.Inthefuture,magnetic resonancewithloadmayperhapsbecomeasuperiorimaging examincomparisonwithradiography.
Osteoarthritis ofthe knee isacommon and fascinating disease.Theradiographicanalysisandtheclassificationused arecrucialpointsofcontroversyonthissubject.Thepresent study suggests that the original Kellgren and Lawrence classification8anditsvariantsgenerateddisagreementamong observers. Thus, it isimportant toresearch and developa radiographicclassificationofthekneetoobtainaconsensus or,perhaps,toimproveagreement.
Conclusions
TheKellgrenandLawrenceclassificationanditsvariants gen-eratedlowreproducibilityamongobservers.
In the intraobserver analysis, discordant results were observed.Thisdemonstratesthelackofuniformityintheuse ofthisclassificationanditsvariants,evenamongexperienced observers.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.CobraH,BarrettoJM,AlbuquerqueRP.Artroplastia unicompartimentaldojoelho.In:PalmaIM,editor.
Artroplastiatotaldojoelho.RiodeJaneiro:Guanabara;2008. p.105–12.
2.SchiphofD,deKlerkBM,KerkhofHJ,HofmanA,KoesBW, BoersM,etal.ImpactofdifferentdescriptionsoftheKellgren andLawrenceclassificationcriteriaonthediagnosisofknee osteoarthritis.AnnRheumDis.2011;70(8):1422–7.
3.AlbuquerqueRP,GiordanoV,SturmL,AzevedoJúniorV,Leão A,AmaralN.Análisedareprodutibilidadedetrês
classificac¸õesparaaosteoartrosedojoelho.RevBrasOrtop. 2008;43(8):329–35.
5. FrancoJS,MusafirM.Classificac¸ãodasfraturasmais freqüente.RiodeJaneiro:Schering-Plough;1991.
6. WeidowJ,CederlundCG,RanstamJ,KärrholmJ.Ahlbäck gradingofosteoarthritisoftheknee.Poorreproducibilityand validitybasedonvisualinspectionofthejoint.ActaOrthop. 2006;77(2):262–6.
7. SunY,GuentherKP,BrennerH.Reliabilityofradiographic gradingofosteoarthritisofthehipandknee.ScandJ Rheumatol.1997;26(3):155–65.
8. KellgrenJH,LawrenceJS.Radiologicalassessmentof osteo-arthrosis.AnnRheumDis.1957;16(4):494–502.
9. AhlbäckS.Osteoarthrosisoftheknee.Aradiographic investigation.ActaRadiolDiagn.1968;Suppl.277:7–72.
10.KeyesGW,CarrAJ,MillerRK,GoodfellowJW.Theradiographic classificationofmedialgonarthrosis–correlationwith operationmethodsin200knees.ActaOrthopScand. 1992;63(5):497–501.
11.PeterssonIF,BoegardT,SaxneT,SilmanAJ,SvenssonB. Radiographicosteoarthritisofthekneeclassifiedbythe AhlbackandKellgren&Lawrencesystemsforthe tibiofemoraljointinpeopleaged35–54yearswithchronic kneepain.AnnRheumDis.1997;56(8):493–6.
12.DanielssonL,HernborgJ.Clinicalandroentgenologicstudyof kneejointswithosteophytes.ClinOrthopRelatRes.
1970;(69):302–12.
13.KijowskiR,BlankenbakerDG,StantonPT,FineJP,DeSmetAA. Radiographicfindingsofosteoarthritisversusarthroscopic findingsofarticularcartilagedegenerationinthe
tibialfemoraljoint.Radiology.2006;239(3):818–24.
14.FelsonDT,GaleDR,ElonGaleM,NiuJ,HunterDJ,GogginsJ, etal.Osteophytesandprogressionofkneeosteoarthritis. Rheumatology(Oxford).2005;44(1):100–4.
15.DejourH,CarretJP,WalchG.LesGonarthroses.In:7émes JournéesLyonnaisesdeChirurgiedeGenou.1991.
16.RodriguesAA,KaramFC,ScorsattoC,MartinsC,PiresLAS. Análisedareprodutibilidadedaclassificac¸ãodeKellgrene
Lawrenceparaaosteoartrosedojoelho.RevAMRIGS. 2012;56(2):107–10.
17.SchiphofD,BoersM,Bierma-ZeinstraSM.Differencesin descriptionsofKellgrenandLawrencegradesofknee osteoarthritis.AnnRheumDis.2008;67(7):1034–6.
18.RosenbergTD,PaulosLE,ParkerRD,CowardDB,ScottSM.The forty-five-degreeposteroanteriorflexionweight-bearing radiographoftheknee.JBoneJointSurgAm.
1988;70(10):1479–83.
19.MasonRB,HorneJG.Theposteroanterior45flexion weight-bearingradiographoftheknee.JArthroplasty. 1995;10(6):790–2.
20.VillardiAE,MandarinoM,VeigaLT.Avaliac¸ãoda reprodutibilidadedaclassificac¸ãodeAhlbäckmodificada paraosteoartrosedojoelho.RevBrasOrtop.2006;41(5): 157–61.
21.GalliM,DeSantisV,TafuroL.ReliabilityoftheAhlbäck classificationofkneeosteoarthritis.OsteoarthritisCartilage. 2003;11(8):580–4.
22.KhanFA,KoffMF,NoiseuxNO,BernhardtKA,O’ByrneMM, LarsonDR,etal.Effectoflocalalignmentoncompartmental patternsofkneeosteoarthritis.JBoneJointSurgAm. 2008;90(9):1961–9.
23.VilaltaC,NunezM,SegurJM,DomingoA,CarbonellJA, MaculéF.Kneeosteoarthritis:interpretationvariabilityof radiologicalsigns.ClinRheumatol.2004;23(6):501–4.
24.BrandtKD,FifeRS,BrausteinEM,KatzB.Radiographic gradingoftheseverityofkneeosteoarthritis:relationofthe KellgrenandLawrencegradetoagradebasedonjointspace narrowingandcorrelationwitharthroscopicevidenceof articularcartilagedegeneration.ArthritisRheum.1991;34(11): 1381–6.