1
Nurse, PhD. Adj unct Professor, Minas Gerais Federal Universit y, College of Nursing, Brazil, e- m ail: acoliveira@ufm g.br
Disponible en castellano/ Disponível em língua portuguesa SciELO Brasil w w w .scielo.br/ rlae
EVALUATI ON OF UNDERREPORTED SURGI CAL SI TE I NFECTI ON EVI DENCED BY
POST-DI SCHARGE SURVEI LLANCE
Adr iana Cr ist ina de Oliv eir a1 Daclé Vilm a Car v alho1
Oliv eir a AC, Car valh o DV. Ev alu at ion of u n d er r ep or t ed su r g ical sit e in f ect ion ev id en ced b y p ost - d isch ar g e sur v eillance. Rev Lat ino- am Enfer m agem 2 0 0 7 set em br o- out ubr o; 1 5 ( 5 ) : 9 9 2 - 7 .
The Sur gical Sit e I nfect ion ( SSI ) has been point ed as one of t he m ost im por t ant infect ion sit es. This
st udy aim ed t o det erm ine t he surgical sit e infect ion incidence during hospit alizat ion and t he im pact of not ificat ion aft er dischar ge t hr ough t w o m et hods. This pr ospect iv e st udy w as car r ied out in t he digest iv e sy st em sur ger y service ( DSS) of t wo general hospit als of São Paulo, in t he period from August , 2001 t o March, 2002. I ncidence lev els of 6 . 7 % an d 4 . 5 % w er e n ot if ied in t h e in st it u t ion s A an d B r espect iv ely . Th e in ciden ce of SSI af t er
dischar ge in t he inst it ut ion A w as 27% and 13.4% in t he inst it ut ion B. Sur v eillance aft er dischar ge ev idenced global rat es of 33.7% and 17.9% for inst it ut ions A and B respect ively. The rat es of infect ion increased 5.02 and 3.98 t im es respect ively in inst it ut ions A and B.
DESCRI PTORS: cr oss infect ion; infect ion cont r ol; nur sing
EVALUACI ÓN DE LA SUB NOTI FI CACI ÓN DE I NFECCI ÓN DEL SI TI O QUI RÚRGI CO
EVI DENCI ADA A TRAVÉS DE LA VI GI LANCI A DESPUÉS DEL ALTA
La I nfección del sit io quirúrgico ( I SQ) ha aparecido com o uno de los m ás im port ant es sit ios de infección. La finalidad de est e est udio fue det erm inar la incidencia de la infección del sit io quirúrgico durant e la int ernación y el im pact o de la not ificación después del alt a a t ravés de dos m ét odos. Se t rat ó de un est udio prospect ivo, en
el ser v icio de cir ugía del sist em a digest iv o ( CSD) de dos hospit ales gener ales de São Paulo, en el per iodo de agost o de 2001 a m arzo de 2002. Se diagnost icaron durant e la int ernación una incidencia de 6,7% y de 4,5% p ar a las in st it u cion es A y B, r esp ect iv am en t e. An alizán d ose la in cid en cia d e I SQ, d esp u és d el alt a, en la inst it ución A est o era del 27% y del 13,4% en la inst it ución B. De est a m anera, con la vigilancia después del
alt a, se verificó una t asa global del 33,7% y del 17,9% de I SQ para las inst it uciones A y B, respect ivam ent e, significando un incr em ent o de la t asa de infección en 5,02 y 3,98 v eces par a las inst it uciones r espect iv as.
DESCRI PTORES: infección hospit alar ia; cont r ol de infecciones; enfer m er ía
AVALI AÇÃO DA SUBNOTI FI CAÇÃO DA I NFECÇÃO DO SÍ TI O CI RÚRGI CO EVI DENCI ADA
PELA VI GI LÂNCI A PÓS-ALTA
A infecção do sít io cirúrgico ( I SC) t em sido apont ada com o um dos m ais im port ant es sít ios de infecção. Est e est udo obj et ivou det erm inar a incidência da infecção do sít io cirúrgico durant e a int ernação, e o im pact o da not ificação pós- alt a por m eio de dois m ét odos. Trat a- se de est udo prospect ivo, realizado no serviço de cirurgia do aparelho digest ivo ( CAD) de dois hospit ais gerais de São Paulo, no período de agost o de 2001 a m arço de
2002. Durant e a int ernação, foi not ificada incidência de 6,7 e de 4,5% para as inst it uições A e B, respect ivam ent e. Analisando- se a incidência da I SC, após a alt a, na inst it uição A foi de 27% e de 13,4% na B. A realização da vigilância pós- alt a evidenciou t axa global de 33,7 e 17,9% de I SC para as inst it uições A e B, respect ivam ent e, represent ando increm ent o da t axa de infecção em 5,02 e 3,98 vezes para as respect ivas inst it uições.
I NTRODUCTI ON
I
n t h e con t ex t of h osp it al in f ect ion s ( HI ) , Surgical Sit e I nfect ion ( SSI ) has st ood out as one oft he m ost im por t ant infect ion sit es, w it h an av er age
60% incr ease in hospit alizat ion per iods. I n addit ion,
it also dem ands gr eat pr event ion effor t s ( 1- 2).
SSI refers t o infect ions t hat occur in surgical
i n ci si o n s, a f f e ct i n g t i ssu e s, o r g a n s a n d ca v i t i e s
m anipulat ed dur ing sur ger y. Diagnosis can occur up
t o 30 day s aft er t he pr ocedur e, or ev en one y ear in
cases inv olv ing pr ost heses ( 1- 2).
S S I i s a r e l e v a n t c o m p l i c a t i o n , s i n c e i t
cont ribut es t o increasing post - surgery pat ient m ort alit y
an d m or b id it y r at es. Th u s, it cau ses p h y sical an d
em ot ion al h ar m s, as w ell as h av in g t o leav e w or k
an d so ci al l i f e. I n ad d i t i o n , i t co n si d er ab l y r ai ses
t r eat m ent cost s and incr eases hospit al st ay. Despit e
b ein g t h e m ost com m on su r g er y com p licat ion , SSI
should be avoided and it s occurrence should be wit hin
t he lev els accept ed by com pet ent or gans ( 1- 2).
Accor ding t o t he Healt h Minist r y, Rule 2.616/
9 8( 3), ev er y hospit al m ust hav e r ules and guidelines
f o r h o s p i t a l i n f e c t i o n c o n t r o l a n d p r e v e n t i o n ,
o r g a n i z e d t h r o u g h H o s p i t a l I n f e c t i o n Co n t r o l
Pr og r am s ( HI CP) , d ev elop ed b y Hosp it al I n f ect ion
Cont r ol Com m issions ( HI CC) . Hence, it is t he HI CC’s
r espon sibilit y t o per f or m epidem iologic su r v eillan ce
f o r e v e r y p a t i e n t , e s p e c i a l l y t h o s e w i t h h i g h e r
in f ect ion r isk s, su ch as su r gical pat ien t s. I t is also
s u g g e s t e d t h a t s u r v e i l l a n c e b e d o n e t h r o u g h
pr ospect iv e m et hods, such as t he act iv e, sy st em at ic,
and cont inuous sear ch for hospit al infect ions and t heir
dissem inat ion ( 1- 5).
I n t his cont ext , it is observed t hat , regarding
SSI in m ost inst it ut ions, sur gical pat ient sur v eillance
o c c u r s o n l y d u r i n g h o s p i t a l i z a t i o n , d e s p i t e t h e
r ecom m en d at ion of t h e Cen t er f or Disease Con t r ol
a n d Pr e v e n t i o n ( CD CP) , i n A t l a n t a . Th e CD CP
em phasizes t hat t hese pat ient s, due t o specific fact ors
inher ent t o sur ger y and t heir condit ion, should hav e
t h ei r su r v ei l l an ce ex t en d ed t o t h e p o st - d i sch ar g e
p er iod ( 1 ). St u d ies t h at p er f or m ed su r g ical p at ien t
follow - up aft er discharge est im at e t hat 12 t o 84% of
t h e S S I a p p e a r s a f t e r d i s c h a r g e . Th i s c a u s e s
u n d e r r e p o r t e d r a t e s , s i n c e s u r v e i l l a n c e o c c u r s
ex clusiv ely dur ing hospit alizat ion( 1- 2, 4- 8).
Th e r e a r e s e v e r a l r e c o m m e n d e d p o s t
-dischar ge sur v eillance m et hods for sur gical pat ient s.
Therefore, it is m andat ory t hat each inst it ut ion adopt
w h a t b e st f i t s i t s r e a l i t y ( i n f r a st r u ct u r e , h u m a n
r esou r ces, ph y sical ar ea, et c) ; n o in st it u t ion sh ou ld
go w it hout sur v eillance.
I n v i e w o f t h i s i s s u e ’ s e p i d e m i o l o g i c a l
r elev an ce an d t h e im p or t an ce of p er f or m in g p or t
-d i sch ar g e su r g i cal p at i en t su r v ei l l an ce, t h i s st u -d y
aim ed t o d et er m in e t h e su r g ical sit e in f ect ion r at e
during hospit alizat ion and t he im pact of post - discharge
r epor t ing t hr ough differ ent m et hods.
CASES AND METHOD
An epidem iological, descr ipt iv e, ex plor at or y
st udy was conduct ed, com paring surgical sit e infect ion
r at es dur ing hospit alizat ion and t he im pact of post
-disch ar ge r epor t s t h r ou gh differ en t m et h ods at t w o
t each in g h osp it als. Bot h ar e t er t iar y car e h osp it als
located in the city of Sao Paulo, Brazil, and were referred
to in the study as Hospital “A” and Hospital “ B”.
Eligible part icipant s were all pat ient s adm it t ed
f or d ig est iv e sy st em su r g er y f r om Au g u st 2 0 0 1 t o
Ma r ch 2 0 0 2 . Th e N a t i o n a l N o so c o m i a l I n f e c t i o n
Su r v eillan ce Sy st em ( NNI S) r ecom m en dat ion s w er e
u sed t o det er m in e t h e in clu sion cr it er ia, w h ich ar e:
being an NNI S pat ient : defined as pat ient s who st ayed
i n t h e h o sp i t a l o v er n i g h t , t h a t i s, a d m i ssi o n a n d
d i s c h a r g e t a k e p l a c e o n d i f f e r e n t d a y s ; h a v i n g
u n d er g on e an NNI S su r g ical p r oced u r e: d ef in ed as
t hose in which a single pat ient ’s ent rance t o t he surgery
u n it is r eg ist er ed , an d t h e su r g eon m ak es at least
one incision in t he pat ient ’s skin or m ucous m em brane,
and closes t he incision befor e t he pat ient leav es t he
oper at ing r oom ( 1).
D u r i n g h o s p i t a l i z a t i o n , t w o n u r s i n g
u n der gr adu at es per for m ed daily act iv e sear ch es for
surgical sit e infect ions in t he pat ient s included in t he
st udy and hospit alized in t he digest ive syst em surgery
unit s. The t w o st udent s w er e pr ev iously t r ained and
r e c e i v e d a p p r o p r i a t e s u p e r v i s i o n f r o m t h e l e a d
r esear cher. Pat ient for m s, in addit ion t o m edical and
n u r sin g r ecor d s, w er e t h e p r im ar y sou r ce f or d at a
collect ion. Direct surgical incision evaluat ion was done
w h en n eeded.
Dat a con cer n in g p at ien t id en t if icat ion w er e
c o l l e c t e d , s u c h a s g e n d e r a n d a g e , a s w e l l a s
inform at ion about t he SSI , place of diagnosis ( during
hospit alizat ion of aft er discharge) , t he int erval bet ween
su r ger y dat e an d SSI r epor t an d SSI locat ion ( t h at
SSI was diagnosed using t he CDCP guideline
for surgical sit e infect ion prevent ion and cont rol, which
proposes t hat purulent secret ions should be considered
t he gold st andar d for SSI r epor t , as long as it does
not charact erize a local react ion t o st it ches. Moreover,
it also r ecom m en ds t h at , af t er bein g r epor t ed, t h e
SSI sh ou ld b e classif ied accor d in g t o it s locat ion:
superficial ( affect s only t he skin or subcut aneous cell
t issu e) , deep ( in v olv es deep st r u ct u r es of m u scu lar
w all, f ascia an d lay er ) , an d or g an / cav it y ( in v olv es
anat om ic st ruct ures, which were open or m anipulat ed
d u r in g su r g er y ) ( 1 ); t h is st u d y com p lied w it h t h ese
cr it er ia.
Post - d isch ar g e su r v eillan ce w as p er f or m ed
t h r ou g h t elep h on e con t act an d r et u r n v isit s t o t h e
ou t pat ien t clin ic, du e t o t h e differ en ce bet w een t h e
t w o inst it ut ions under st udy. That is, one inst it ut ion
had a single out pat ient clinic wit h fixed days and hours
for pat ient ret urn visit s t o rem ove st it ches and undergo
m edical ev aluat ion. At t he ot her inst it ut ion, pat ient s
were inst ruct ed by t he surgeon t o ret urn t o t he clinic
o r o t h e r l o ca t i o n s ( b a si c h e a l t h u n i t s, e t c) , a n d
a p p o i n t m e n t t i m e s d i d n o t d e p e n d o n i n st i t u t i o n
con t r ol.
Hosp it al A d et er m in ed t h at p ost - d isch ar g e
f o l l o w - u p w o u l d b e p er f o r m ed t h r o u g h t el ep h o n e
cal l s, b et w een t h e 7t h an d 1 4t h d ay, d u e t o so m e
d i f f i cu l t i e s r e g a r d i n g p h y si ca l st r u ct u r e a n d t h e
d i f f e r e n t a ssi st a n t p h y si ci a n s’ w o r k h o u r s a t t h e
out pat ient clinic( 9). Telephone calls w er e m ade using
a sp e ci f i c p r i n t e d g u i d e l i n e , w h i ch i n cl u d e d t h e
quest ions t o be ask ed t o t he pat ient . At t his m om ent ,
sp ecial car e w as t ak en t o av oid an sw er in d u ct ion .
Th e i n s t r u m e n t u s e d w a s f o u n d e d o n o b j e c t i v e
quest ions t hat y ielded pr ecise answ er s r egar ding t he
s u r g i c a l i n c i s i o n , s u c h a s : h y p e r t h e r m i a , h e a t ,
r edness, dehiscence, pus on t he sur gical incision and,
w h en p r esen t , i n d i v i d u al s w er e ask ed t o d escr i b e
t h e secr et ion in d et ail - it s asp ect , color, locat ion ,
quant it y and/ or need for m edical r et ur n due t o any
ev en t r elat ed w it h t h e su r g er y an d / or an t ib iot ics.
Af t er t h e con t act , each case w as d iscu ssed am on g
t h e st u d y g r o u p a n d , w h e n n e ce ssa r y, w i t h t h e
a s s i s t a n t t e a m , w i t h a v i e w t o o b t a i n i n g
h om ogen eou s cr it er ia t o r epor t cases or n ot .
Pa t i en t s w h o , f o r so m e r ea so n , w er e n o t
hom e or were not locat ed on t he first call, were called
again at a previously scheduled t im e, during t he sam e
w eek , so as t o gu ar an t ee t h at t h e h igh est possible
num ber of pat ient w as r eached.
At Hospital B, post-discharge patient control was
perform ed through outpatient return visits sim ultaneous t o t h e m ed i cal r et u r n , so as t o av o i d ad d i t i o n al
transportation costs for patients. Returns occurred between the 7th and 14th day after the surgery, or after longer periods
in cases of longer hospital stays. Patients were seen by a st udy gr oup m em ber, w ho evaluat ed t he pat ient and
checked t he surgical incision sit e for hyperem ia, heat , redness, dehiscence, secretion on incision and, if present,
its aspect, color, location and quantity.
Wit h a view t o avoid SSI overreport ing, during
hospit alizat ion, each report was com pared t o t hose of
t he out pat ient clinic, t hrough periodical pat ient report v er if icat ion s, so t h at t h er e w er e n o in com p let e or
lacking dat a, nor double report form s. I n ot her words, it was guarant eed t hat t here were no duplicat e report s
of diagnoses reached at t he hospit al, out pat ient clinic or on t he t elephone. I n order t o com ply wit h t he st udy
m et hod, which det erm ines t hat pat ient follow- up should include up t o t he t hir t eent h day aft er t he sur ger y, a
second t elephone cont act was est ablished wit h pat ient s fr om bot h in st it u t ion s bet w een t h e t w en t y - fir st an d
t hirt iet h day, so as t o com plet e t his st age.
The r esear ch pr oj ect w as appr ov ed by bot h I n s t i t u t i o n a l Re v i e w B o a r d s i n v o l v e d . Pa t i e n t s
provided inform ed consent for t he follow- up, including int ra- hospit al post - surgery, out pat ient clinic visit s and/
or post er ior t elephone cont act .
D a t a a n a l y s i s a n d s t a t i s t i c a l t e s t s w e r e
per for m ed using Ex cel 2000R, Epi- info ( v er sion 6.04) an d t h e St at ist ical Pr od u ct s an d Ser v ice Solu t ion s
( S PS S ) f o r W i n d o w s ( v e r s i o n 1 0 . 0 : S PS S , I n c .
Chicago, I I I ) . Univariat e, sim ple descript ive ( absolut e) and percent age analyses were used t o com pare groups
and SSI r at es dur ing and aft er dischar ge.
RESULTS
The sam ple from Hospit als A and B consist ed
of 252 ( 41.4% ) and 357 ( 58.6% ) patients, respectively, subj ect ed t o digest ive syst em surgeries regarding t he
following procedures: herniorrhaphy, cholecyst ect om y,
lapar ot om y, and colect om y. St udy par t icipant s w er e, on t he av er age, 48 y ear s old, r anging fr om 1 t o 91
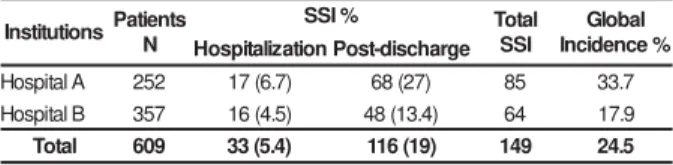
y ear s. As t o gender, 53% of t he pat ient s w er e m en. Regarding SSI diagnosed during hospitalization, Hospital
A present ed a rat e of 6.7% ( 17/ 252) , against 4.5% at Hospital B ( 16/ 357) . As to SSI detected after discharge,
t he rat e for Hospit al A was 27% ( 68/ 252) , and 13.4%
Table 1 - Dist ribut ion of pat ient s subj ect ed t o digest ive
sy st em sur ger ies at hospit als A and B, accor ding t o
Su r g i c a l Si t e I n f e c t i o n ( SSI ) r e p o r t - d u r i n g
h o s p i t a l i z a t i o n a n d p o s t - d i s c h a r g e - a n d g l o b a l
incidence at bot h inst it ut ions, Sao Paulo, SP, 2001- 2002
m aj orit y of infect ions det ect ed aft er discharge ( > 90% )
also belonged t o t he sam e cat egor y.
DI SCUSSI ON
Hospit al in f ect ion con t r ol pr ogr am s t h at do
n o t i n cl u d e p o st - d i sch a r g e f o l l o w - u p f o r su r g i ca l
pat ient s gener at e under r epor t ed r at es. St udies show
t hat 12 t o 84% of all SSI becom e evident aft er hospit al
discharge. This confirm s t he im port ance and necessit y
of t his t y pe of sy st em ized follow - up, em phasized by
t he cur r ent t end of shor t er hospit al st ay s. Mor eov er,
i t i s m a n d a t o r y t o o b t a i n a c c u r a t e r a t e s , t h u s
per m it t ing int er - hospit al com par isons( 1- 2, 4, 7- 8).
The SSI r at e det ect ed dur ing hospit alizat ion
in b ot h g r ou p s w as low er t h an t h at r ef er en ced in
Br azilian st udies. The 13% aver age hospit al infect ion
r at e in Br azil( 2 , 1 0 - 1 1 ) t r an slat es a cer t ain t r an q u ilit y
regarding t he percent ages found in t his st udy. However,
since it is acknowledged t hat m ost st udies do not cover
surgical pat ient follow- up aft er discharge, special care
should be t aken when int erpret ing t he dat a.
Su r gical pat ien t f ollow - u p r at es ( ou t pat ien t
clinic and t elephone) r eached 90% in Hospit al A and
96.9% in Hospit al B. Besides t he t wo inst it ut ions having
sim ilar rat es, it was observed t hat global pat ient loss
dur ing follow - up did not ex ceed 10% . This is highly
sa t i sf a ct o r y, co n si d e r i n g p a r a m e t e r s f r o m o t h e r
st udies, which report ed t hat bet ween 64 and 89% of
pat ient s r et ur ned for post - dischar ge visit s ( 4, 8).
Re g a r d i n g t h e m e t h o d s u s e d f o r p o s t
-dischar ge sur v eillance, it is obser v ed t hat out pat ient
clin ic r et u r n s h av e b een con sid er ed t h e r ef er en ce
m et h od , w h ose m ain ad v an t ag e is t h e f act t h at it
proposes t hat every SSI should be not ified, regardless
o f i t s l o ca t i o n . Th i s i s d e t e r m i n e d b a se d o n t h e
obser v ed difficu lt y becau se, w h en ph y sician s r epor t
SSI at t heir offices/ out pat ient clinics, super ficial SSI
g o u n n o t i ced an d ar e n o t r ep o r t ed . Th i s h ap p en s
b e c a u s e s u p e r f i c i a l S S I u s u a l l y d o n o t r e q u i r e
a n t i m i cr o b i a l t h e r a p y, b e si d e s b e i n g si m p l e a n d
generally solved by applying local heat ( 1, 6, 12).
On t h e ot h er h an d , t h is t y p e of f ollow - u p
( ou t pat ien t clin ic r et u r n ) , per f or m ed ex clu siv ely by
t he Hospit al I nfect ion Cont r ol Com m ission st aff, has
been associat ed wit h higher reliabilit y and good ret urn
r at es. This occur s despit e t he fact t hat t his m odalit y
im plies differ ent iat ed phy sical and hum an r esour ces,
which is not always possible for m ost inst it ut ions ( 12). s n o it u ti t s n
I PaNitents SSI% TSoStaIl IncGidleonbcael% n o it a z il a ti p s o
H Post-discharge A l a t i p s o
H 252 17(6.7) 68(27) 85 33.7
B l a t i p s o
H 357 16(4.5) 48(13.4) 64 17.9
l a t o
T 609 33(5.4) 116(19) 149 24.5
Post - dischar ge sur v eillance r ev ealed a global
SSI rat e of 33.7% and 17.9% for hospit als A and B,
and an im port ant im pact on t he infect ion rat e of 5.02
and 3.98 t im es for hospit als A and B, respect ively. I t
is sur pr ising t hat , if post - dischar ge sur v eillance had
not been per for m ed, t he global SSI r at e w ould hav e
been ser iou sly u n der r epor t ed.
Table 2 - SSI occur r ence int er val at hospit als A and
B, according t o t he diagnosis m om ent , Sao Paulo, SP,
2 0 0 1 - 2 0 0 2
n o i t u t i t s n
I A B
y r e g r u s -t s o P ) s y a d ( l a v r e t n i n o it a z il a ti p s o
H Post-dischargeHosptiailzaitonPost-discharge
n % n % n % n %
7
< 7 41 27 40 8 50 9 19
4 1 < a 7
> 8 47 21 31 4 25 29 60
1 2 < a 4 1
> 0 0 12 18 2 12.5 6 13
0 3 a 1 2
> 2 12 8 11 2 12.5 4 8
l a t o
T 17 100 68 100 16 100 48 100
Percent age of diagnosed SSI according t o post - surgery int erval ( days)
Dur ing pat ient s’ st ay at Hospit al A, 4 1 % of
i n f ect i o n s w er e d et ect ed b ef o r e t h e 7t h d a y a f t er
su r g e r y. At H o sp i t a l B, d e t e ct i o n r e a ch e d 5 0 % .
Regarding post - discharge det ect ion, in hospit als A and
B, t he highest infect ion r at es w er e found befor e t he
14t h day aft er sur ger y ; 81% and 79% , r espect ively.
Tab le 3 - Dist r ib u t ion of su r g ical sit e in f ect ion s at
hospit als A and B, according t o t ot al classificat ion and
r epor t ed sit e. Sao Paulo, SP, 2001- 2002
l a t i p s o
H A B
e t i S n o i t c e f n
I HosptiailzaitonPost-dischargeHosptiailzaitonPost-discharge
n % n % n % n %
l a i c if r e p u
S 10 59 67 98.5 14 87.5 44 92
p e e
D 6 35 1 1.5 2 12.5 2 4
y t i v a c / n a g r
O 1 6 - - - - 2 4
l a t o
T 17 100 68 100 16 100 48 100
Regar ding infect ion classificat ion, super ficial
The t elephone cont act s perform ed in Hospit al
A could be consider ed an easy, low cost m et hod. I t
t ends t o be used when pat ient s are not able t o ret urn
t o t h e h o sp i t a l ’ s o u t p a t i e n t cl i n i c. Th e m e t h o d ’ s
sen sit iv it y cou ld be a lim it at ion , du e t o in for m at ion
bias. However, since cont act s were m ade by a specific
t rained professional in t his st udy, who asked obj ect ive
clear quest ions, it is believed t hat t he inform at ion bias
has been m inim ized( 12).
I n or der t o per f or m su r gical pat ien t f ollow
-u p af t er h ospit al disch ar ge, t h e CDCP r ecom m en ds
a n i d e a l p e r i o d o f u p t o 3 0 d a y s a f t e r su r g e r y.
How ev er, sev eral st udies hav e st at ed t hat m ost SSI
could be ident ified bet ween t he 15t h and t he 21st day,
w it h aver ages above 80% befor e t he 15t h day6- 8.
I n t h e p r e s e n t s t u d y, e v e n t h e 7t h d a y
r e v e a l e d a p e r ce n t a g e o f 4 1 % a n d 5 0 % o f SSI
diagnosed dur ing pat ient hospit alizat ion at Hospit als
A a n d B, r e sp e ct i v e l y. I n a d d i t i o n , f r o m h o sp i t a l
discharge t o t he 14t h day aft er surgery, t his percent age
was higher, reaching 81% for Hospit al A and 79% for
Hospit al B. This finding, accor ding t o som e aut hor s,
j u st i f i es t h at p o st - d i sch ar g e f o l l o w u p o f su r g i cal
pat ient s could be reduced t o 15 days ( 4, 7- 8).
Re g a r d i n g s p e c i f i c S S I s i t e s , t h e m o s t
fr equent w er e t he super ficial, bot h int r a- hospit al and
a f t e r d i s c h a r g e . As m e n t i o n e d b e f o r e , t h e v a s t
m a j o r i t y o f S S I d i a g n o s e d a f t e r d i s c h a r g e i s
super ficial( 4, 8), ex act ly due t o t he possibilit y of ear ly
disch ar ge an d sh or t er h ospit al st ay. How ever, w h en
follow- up is perform ed by professionals who were not
t r ained accor ding t o t he specific m et hod for hospit al
in f ect ion d iag n osis, t h is in f ect ion cat eg or y is of t en
ignor ed, since it neit her poses any lim it at ions t o t he
pat ient nor requires re- hospit alizat ion, and, especially,
it is easy t o solv e f r om a clin ical per spect iv e. Th is
causes under r epor t s t o t he hospit al infect ion cont r ol
ser v i ce.
CONCLUSI ON
Th is st u dy f ou n d 6 . 7 % an d 4 . 5 % r at es f or
sur v eillance lim it ed t o t he hospit alizat ion per iod. For
global r at es in clu din g post - disch ar ge SSI follow - u p,
incidence rat es were 27% and 13.4% for Hospit als A
and B, r espect iv ely. Hence, it is obser ved t her e w as
an im por t ant im pact on infect ion r at es, of 5. 02 and
3.98 t im es for t he st udy inst it ut ions.
Dur ing post - dischar ge sur v eillance, a higher
SSI rat e was observed for Hospit al A, which perform ed
pat ient follow - up t hr ough ov er t he t elephone.
Bot h groups showed prevalence for superficial
SSI , bot h dur ing hospit alizat ion and aft er dischar ge.
Hence, t his st udy confirm s t he im port ance of
p e r f o r m i n g s u r g i c a l p a t i e n t f o l l o w - u p d u r i n g
hospit alizat ion as well as aft er discharge as a way t o
g u a r a n t ee r el i a b l e SSI r a t es. Th i s w o u l d m a k e i t
f e a s i b l e t o i m p l e m e n t p r e v e n t i o n a n d c o n t r o l
m e a su r e s, si n ce e p i d e m i o l o g i ca l co m p r e h e n si o n
r equir es k now ledge r egar ding infect ion r isk s as w ell
as det er m inant or associat ed fact or s.
ACKNOW LEDGEMENT
The aut hors t hank Professor Robert I quiapaza
for his r elev ant suggest ions and r ecom m endat ions.
REFERENCES
1. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR.
Gu i d el i n e f o r p r ev en t i o n o f su r g i cal si t e i n f ect i o n . I n f ect
Con t r ol Hosp Ep id em iol 1 9 9 9 ; 4 ( 2 0 ) : 2 4 7 - 7 9 .
2 . Fe r r a z EM, Fe r r a z AA, Ba ce l a r TS, Al b u q u e r q u e HST,
Vasconcelos MDM, Leão CS. Cont role de infecção em cirurgia
g er al - r esu lt ad o d e u m est u d o p r osp ect iv o d e 2 3 an os e
4 2 . 2 7 4 cir u r g ias. Rev Colég io Br as Cir 2 0 0 1 ; 1 ( 2 8 ) : 1 7 - 2 5 .
3. Minist ério da Saúde ( BR) . Port aria núm ero 2.616, de 12 de
m aio de 1998. Resolve expedir na form a de anexos I , I I , I I I ,
I V e V,diret rizes e norm as para a prevenção e o cont role de
i n f ecçõ es h o sp i t al ar es, f i can d o r ev o g ad a a Po r t ar i a 9 3 0 .
D i á r i o O f i c i a l d a U n i ã o , B r a s íl i a ( D F) , 1 3 d e m a i o d e
1 9 9 8 . p . 1 3 3 - 5 .
4. Oliveira AC, Soares JL, Garcia CA, Scat ena PD, Osvaldo L,
Ciosak SI . Seguim ento pós-alta do paciente cirúrgico: um a análise
da im port ância da sub- not ificação da incidência da infecção do
sít io cirúrgico. Rev Min Enferm agem 2003; 7( 1) : 48- 51.
5. Oliveira AC, Ciosak SI . I nfecção de sítio cirúrgico no seguim ento
pós-alta: im pacto na incidência e avaliação dos m étodos utilizados.
Rev Esc Enferm agem USP 2004; 38: 379- 85.
6. Oliveira AC, Martins MA, Martinho GH, Clem ente WT, Lacerda
RA. Est udo com par at iv o do diagnóst ico da infecção do sít io
cirúrgico durante e após a internação. Rev Saúde Pública 2002;
3 6 ( 6 ) : 7 1 7 - 2 2 .
7. Rodriguez MD, Ortega AG, Arenas MS, Llorca J. Epidem iology
of surgical- sit e infect ions diagnosed aft er hospit al discharge: a
prospect ive cohort st udy. I nfect Cont rol Hosp Epidem iol 2001;
8. St ock ley JM, Allen RM, Thom linson DF, Const ant ine CE. A
dist r ict gener al hospit al’s m et hod of post - oper at iv e infect ion
su r v eillan ce in clu d in g p ost - d isch ar g e f ollow - u p , d ev elop ed
ov er a fiv e- y ear per iod. J Hosp I nfect 2001; 49: 48- 54.
9 . Whit by M, McLaw s ML, Collopy B, Look e DFL, Doidge S,
Hender son B et al. Post - dischar ge sur v eillance: can pat ient s
r eliab ly d iag n ose su r g ical w ou n d in f ect ion s? J Hosp I n f ect
2 0 0 2 ; 5 2 : 1 5 5 - 6 0 .
10. Poveda VB, Galvão MC, Hayashida M. Análise dos fat ores
d e r i sco r e l a ci o n a d o s à i n ci d ê n ci a d e i n f e cçã o d o si t i o
cir ú r g ico em g ast r ocir u r g ias. Rev Esc En f er m ag em 2 0 0 3 ;
3 7 : 8 1 - 9 .
1 1 . Med eir os AC, Air es Net o T, Dan t as Filh o AM, Pin t o Jr
FEL, Uch ô a RAC, Ca r v a l h o MR. I n f e cçã o h o sp i t a l a r e m
pacient es cir úr gicos de hospit al univ er sit ár io. Act a Cir Br as
2 0 0 3 ; 1 8 ( Su p p l 1 ) : 1 5 - 8 .
12. Noy D, Cr eedy D. Post dischar ge sur veillance of sur gical
sit e infect ions: a m ult i- m et hod appr oach t o dat a collect ion.
Am J I n f ect Con t r ol 2 0 0 2 ; 3 0 : 4 1 7 - 2 4 .