w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Is
there
a
relationship
between
gouty
arthritis
and
Mediterranean
fever
gene
mutations?
Ismail
Sari
a,b,∗,
Ismail
Simsek
b,
Yusuf
Tunca
c,
Bunyamin
Kisacik
b,d,
Hakan
Erdem
b,
Salih
Pay
b,
Hasan
Fatih
Cay
b,
Davut
Gul
c,
Ayhan
Dinc
baDepartmentofRheumatology,SchoolofMedicine,DokuzEylulUniversity,Izmir,Turkey
bDepartmentofRheumatology,GulhaneMilitaryMedicalAcademy,Ankara,Turkey
cDepartmentofMedicalGenetics,GulhaneMilitaryMedicalAcademy,Ankara,Turkey
dDepartmentofRheumatology,SchoolofMedicine,GaziantepUniversity,Gaziantep,Turkey
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received25August2014 Accepted19October2014 Availableonline3January2015
Keywords:
Goutyarthritis MEFVprotein
FamilialMediterraneanfever
a
b
s
t
r
a
c
t
Objective:GoutyarthritisandfamilialMediterraneanfeversharesomeclinicaland patho-logicalfeaturessuchasbeingclassifiedasauto-inflammatorydisease,associationwith inflammasome,short-livedintermittentarthritis,andgoodresponsetocolchicineand anti-interleukin-1treatments.AsMediterraneanfevergeneisthecausativefactoroffamilial Mediterraneanfever,weaimedtoinvestigatetheprevalenceofMediterraneanfevergene mutationsandtheireffectondiseasemanifestationsinTurkishgoutyarthritispatients.
Methods:Ninety-sevenpatientsdiagnosedwithprimarygoutyarthritis(93Mand4F,54 [37–84]years)and100healthycontrols(94Mand6F,57 [37–86]years)wereincludedin thestudy.AllsubjectsweregenotypedfortheMediterraneanfevergenevariations.Number ofgoutattacks,diureticuse,historyofnephrolithiasisandpresenceoftophuswerealso recorded.
Results:ThecarriagerateofMediterraneanfevermutationsforpatientsandcontrolswas 22.7%(n=22)and24%(n=24),respectively.Thecomparisonofthepatientandcontrolgroups yieldednosignificantdifferenceintermsoftheMediterraneanfevermutations’carriagerate (p=0.87).TheallelicfrequenciesoftheMediterraneanfevermutationsinpatientswere11.9% (n=23)and14%(n=28)incontrols(p=0.55).ThepresenceofMediterraneanfevervariants didnotshowanyassociationwithclinicalfeaturesofgoutyarthritis.Thesubgroupanalysis ofpatientsrevealedthatgoutyarthritispatientswithmutationshadsimilarfrequencies oftophus,historyofnephrolithiasisandpodagracomparedtotheoneswithoutmutations (p>0.05).
Conclusions: ThisstudydoesnotprovidesupportforamajorroleofMediterraneanfever mutationsinTurkishgoutyarthritispatients.
©2014ElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](I.Sari).
http://dx.doi.org/10.1016/j.rbre.2014.10.008
Existe
uma
relac¸ão
entre
a
artrite
gotosa
e
as
mutac¸ões
genéticas
da
febre
familiar
do
Mediterrâneo?
Palavras-chave:
Artritegotosa ProteínaMEFV
FebrefamiliardoMediterrâneo
r
e
s
u
m
o
Objetivo: AartritegostosaeafebrefamiliardoMediterrâneo(FFM)compartilhamalgumas característicasclínicasepatológicas,comoserclassificadacomoumadoenc¸aautoimune inflamatória,terassociac¸ãocomoinflamassoma,manifestarartriteintermitentedecurta durac¸ãoeboarespostaatratamentoscomcolchicinaeanti-interleucina-1.Comoogeneda febrefamiliardoMediterrâneo(MEFV)éofatorcausadordaFFM,esteestudotevecomo obje-tivoinvestigaraprevalênciademutac¸õesdogeneMEFVeseuefeitosobreasmanifestac¸ões dadoenc¸aempacientesturcoscomartritegotosa.
Métodos:Foramincluídosnoestudo97pacientescomdiagnósticodeartritegotosaprimária (93Me4F;54[37-84]anos)e100controlessaudáveis(94Me6F;57[37-86]anos).Todosos indivíduosforamsubmetidosàanálisedogenótipoàprocuradevariac¸õesnoMEFV.Também foiregistradoonúmerodecrisesdegota,ousodediuréticoseahistóriadenefrolitíasee presenc¸adetofos.
Resultados: Afrequênciadeportadores demutac¸õesnoMEFVempacientesecontroles foide22,7%(n=22)e24%(n=24),respectivamente. Acomparac¸ãoentreospacientese oscontrolesnãoproduziudiferenc¸aestatisticamentesignificativaemtermosde frequên-ciadeportadoresdemutac¸õesnoMEFV(p=0,87).Asfrequênciasalélicasdemutac¸õesno
MEFVnospacientesforamde11,9%(n=23)e14%(n=28)noscontroles(p=0,55).Apresenc¸a devariantesdoMEFVnãomostrouqualquerassociac¸ãocomascaracterísticasclínicasda artritegotosa.Aanáliseporsubgruposdepacientesrevelouqueaquelescomartritegotosa commutac¸õestinhamfrequênciassemelhantesdetofo,históriadenefrolitíaseepodogra emcomparac¸ãocomosindivíduossemmutac¸ões(p>0,05).
Conclusões:Asmutac¸õesnogeneMEFVnãoexercemumpapelrelevanteempacientesturcos comartritegotosa.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Goutyarthritisisoneofthemostfrequentlyobserved inflam-matory arthritis in the world. Although its epidemiology showssignificant ethnicalvariations,itisaffectingatleast 1–2%ofmeninthewesternworld.1Goutyarthritishassome classical clinical findings such as acute painful attacks of arthritisinthejoints(especiallythefirstmetatarsaljointofthe foot),mono-articularinvolvementandintermittentpattern.2 Itiscausedbythedepositionofmonosodium urate mono-hydrate(MSU)crystalsinthe joints.MSUcrystals inducea varietyofinflammatorycytokinesparticularlyinterleukin-1 (IL-1).3 Inaddition,recent reportsrevealedamajorrole for inflammasomeactivityinthedevelopmentofgoutattacks.3 Ontheotherhand,familialMediterraneanfever(FMF)isthe mostcommonlyseenperiodicfeversyndrome.4FMFiscaused bythe mutations(singlesubstitutions)intheMEditerranean FeVer(MEFV)geneattheshortarmofthe16thchromosome.4 This gene encodes a protein called pyrin. Under normal circumstances, pyrin limits the activation of the NLRP3-inflammasome.Itispresumedthatthemutatedpyrinprotein inFMF istheoretically notableto suppress the inflamma-some,andthustheinflammatoryresponsedevelops.5Both goutyarthritisandFMFsharesomeclinicalandpathogenic mechanismssuch asshort-livedand intermittent arthritis, associationwithinflammasomeandresponsetocolchicine andanti-IL-1therapies.3,6Tothebestofourknowledge,there
has beenno previousstudy about the associationbetween
MEFVgenemutationsandgoutyarthritis.Inthisstudy,we aimedtoinvestigatetheprevalenceofMEFVgenemutations and theireffectondiseasemanifestationsinTurkishgouty arthritispatients.
Methods
Samplesizecalculation
Thesamplesizewascalculatedbyusingtheresultsofprevious studiesthatinvestigatedthefrequencyofMEFVmutationsin patientswithinflammatoryrheumaticdiseasesandhealthy controls.7,8Accordingtotheanalysis,basedon˛=0.05anda
powerof80%,atleast89subjectswereneededpergroup.
Patientsandcontrols
Thecontrol groupincluded 100 unrelatedhealthy subjects without any history ofchronic diseases and was recruited fromtheblooddonorsandrelativesofhospitalstaff.Thestudy wasapprovedbytheEthicsCommitteeandinformedconsent wasobtainedfromalltheparticipants.
MEFVgenemutationanalysis
A total of 197 specimens collected were analyzed for the mutations of the MEFV gene. Genomic DNA from whole blood samples was isolated with QIAamp DNA blood Mini Kit (Qiagen, Hilden, Germany) according to the manufacturer’s instructions. Both exon 2 and exon 10 of the MEFV gene were amplified by polymerase chain reaction (PCR) using the following primers: 5′ -GTGGGACAGCTTCATCATTTTG-3′and5′-CCTTCTCTCTGCGTT TGCTC-3′(exon2),5′-TTACTGGGAGGTGGAGGTTG-3′,and5′ -GAGG AGCTGTGTTCTTCCC-TC-3′ (exon 10). PCR products were purified using a QIAquick PCR Purification Kit (Qia-gen).PurifiedPCRampliconswerebidirectionallyfluorescence sequenced using ABI BigDye Terminator version 1.1 Cycle SequencingKit(AppliedBiosystems)andrunonaABI3100 automatedsequencer(AppliedBiosystems).
Statisticalanalysis
Resultswereexpressedasmean±standarddeviation(SD)and proportionsaspercentages.Achi-squaretestorFisher’sexact test was used, when appropriate, to assess the difference intheprevalenceofMEFVvariantsbetweengouty arthritis patientsandhealthycontrols.Spearman’srhotestwasused todescribecorrelations.Allpvalueswere2-tailed,and confi-denceintervals(CIs)weresetat95%.p-valueslessthan0.05 wereconsideredsignificant.Thestatisticalanalysiswas car-riedout by usingStatistical Packagefor theSocial Science (SPSS),version13.0(SPSSInc.,Chicago,IL,USA).
Results
There were 97 gouty arthritispatients (93 male [M]and 4 female[F], 54 [37–84]years) and100 healthycontrols(94M and6F,57[37–86]years).Thesexandagedistributionswere notdifferentbetweenthegroups(pvaluesare0.75and0.09, respectively). The median number of gout attacks of the patientswere2(1–40);10.8%ofthepatientshadtophus,21.5% hadrenalstonehistory,23.7%ofthepatientswerereceiving diureticsand18.3%hadahistoryofalcoholintake.
Therewere22patientsand24healthycontrolsthatwere carryingatleastonemutatedMEFVallele.Exon2mutations observedinthisstudywereE148Q,R202Q,E230K,T267Iand T177I.Thedetectedexon10mutationswere M694V,M680I, V726A,R761H,A744S andK695R. Distributionofthe muta-tionsinthepatientsandhealthycontrolsaresummarizedin
Table1.ThecarriagerateofMEFVmutationsforpatientsand
controlswere22.7%and24%,respectively.Thecomparisonof thepatientandcontrolgroupsyieldednosignificant differ-enceinterms oftheMEFVmutationscarriagerate(p=0.87; 95%CI=0.57–1.57).Thesub-groupanalysisrevealed that31 (15.7%) subjects were carrying exon 2 and 16 (8.1%) were
Table1–DistributionoftheMEFVgenemutationsinthe goutyarthritisandhealthycontrolgroups.
Goutyarthritis patients,n=97
Healthycontrols,
n=100
M694V/M694V 1
M694V/WT 4 2
M694V/R202Q 1
E148Q/E148Q 2
E148Q/WT 9 14
V726A/WT 1
R761H/WT 1 1
M680I/WT 1
A744S/WT 1 1
K695R/WT 1 1
R202Q/WT 2
R202Q/E230K 1
T267I/WT 1
T177I/WT 1
WT,wildtype.
carryingatleastoneexon10mutations.Thegoutyarthritis patientsandcontrolsdidnotshowanysignificanceregarding thecarriagerateofexon2(12[12.4%]vs.19[19%];p=0.24;95% CI=0.33–1.27,respectively)andexon10(10[10.3%]vs.6[6%]; p=0.31;95%CI=0.65–4.55,respectively)mutations(Table2).
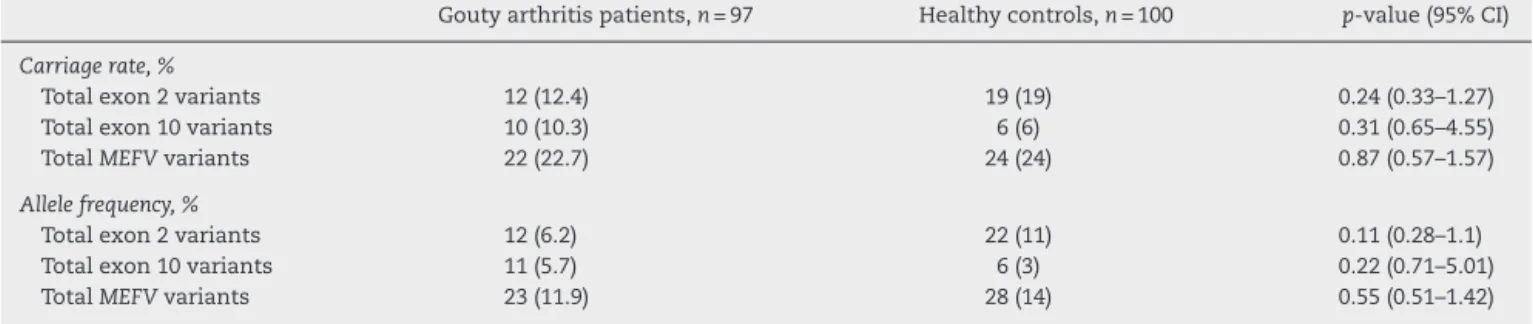
TheallelicfrequenciesoftheMEFVmutationsinpatients were11.9%(n=23)and14%(n=28)incontrols.Theallele fre-quencies did notshow any significancewhen the patients andcontrolswerecompared(p=0.55;95%CI=0.51–1.42).Total exon2andexon10mutationswereobservedin34(8.6%)and 17(4.3%)subjectsrespectively.Thegoutyarthritispatientsand controlsdidnotshowanysignificanceregardingthe distribu-tionofexon2(12[6.2%]vs.22[11%];p=0.11;95%CI=0.28–1.1, respectively)andexon10(11[5.7%]vs.6[3%]);p=0.22;95% CI=0.71–5.01,respectively)mutations(Table2).
WhenweanalyzedE148Qseparately,neithercarriagerate norallelicfrequenciesweredifferentbetweengouty arthri-tis patients andhealthy controls(p=0.2;95% CI=0.23–1.28;
p=0.11; 95% CI=0.21–1.12, respectively). Similarly, M694V mutations were notdiffered significantlybetween patients andcontrols(carriageratep=0.49;95%CI=0.41–7.56andallele frequencyp=0.33;95%CI=0.52–8.5).
Thesubgroupanalysisofgoutyarthritispatientsregarding theirMEFVgenemutationstatusrevealedthatgouty arthri-tispatientswithmutationshadsimilarfrequenciesoftophus (11.3% vs. 9.1%, respectively, p=1),history of nephrolithia-sis(22.5%vs.18.2%,respectively,p=0.77)andpodagra(42.3%
vs.45.5,respectively,p=0.81)comparedtotheoneswithout mutations.Inadditionthenumberofgoutattackswerealso similarbetweenthepatientswithandwithoutmutations(2 [1–8]vs.2[1–40],respectively,p=0.38).
The presence of MEFV mutations and the presence of tophus,historyofnephrolithiasis,diureticusageandnumber ofattacksdidnotshowanycorrelation(p=0.61;0.73;0.81and 0.38,respectively).
Discussion
Table2–AllelefrequenciesandcarriageratesofMEFVvariantsinpatientswithgoutyarthritisascomparedwithhealthy controls.
Goutyarthritispatients,n=97 Healthycontrols,n=100 p-value(95%CI)
Carriagerate,%
Totalexon2variants 12(12.4) 19(19) 0.24(0.33–1.27)
Totalexon10variants 10(10.3) 6(6) 0.31(0.65–4.55)
TotalMEFVvariants 22(22.7) 24(24) 0.87(0.57–1.57)
Allelefrequency,%
Totalexon2variants 12(6.2) 22(11) 0.11(0.28–1.1)
Totalexon10variants 11(5.7) 6(3) 0.22(0.71–5.01)
TotalMEFVvariants 23(11.9) 28(14) 0.55(0.51–1.42)
betweenthegoutyarthritispatientsandhealthycontrols. Fur-thermorethe presenceofMEFVvariantsdidnot showany associationwithclinicalfeaturesofgoutyarthritis.In addi-tion, the severity ofthe gout did not show any difference betweenthepatientswithandwithoutMEFVmutations.
Goutyarthritisisoneofthecommonestformsof inflam-matoryarthropathyintheelderly population.MSUcrystals triggertheinflammatorycascade,whichultimatelyresultin painandinflammation.Inrecentyearsseveralreportsshowed an association between NLRP3 inflammasome and gouty arthritis.3ItishypothesizedthatMSUcrystalsincrease NLRP3-induced IL-1 and dysregulatedproduction ofthecytokine plays an important role in the clinical features of gout.3 Recently gout isclassified asa formof auto-inflammatory diseases.11
FMFisahereditaryauto-inflammatorydisorder character-izedbyacuteattacksoffeverandserosalinflammation.Itis prevalentamongcertainethnicgroupssuchasJews, Arme-nians,Turks,andArabs.4FMFiscausedbymutationsinthe MEFVgene,whichencodesthepyrinprotein.Mutantpyrinis associatedwithuncontrolledinflammatorycascade,probably bydysregulatedinflammasomefunctionandexcessiveIL-1
production.5
Inrecentyearsthereisaconsiderableinterestregarding
MEFV gene mutations and its association with different inflammatorydiseases.InthisrespectMEFVmutationsfound to be increased in ankylosing spondylitis,12 juvenile idio-pathicarthritis,13inflammatoryboweldisease,8palindromic rheumatism,14Behcet’sdisease,7 polyarteritisnodosa15 and Schoenlein–Henochpurpura.16Furthermoreitwasshownthat thesemutationswere associatedwithsevere disease prog-nosisinotherinflammatorysyndromessuchasrheumatoid arthritis.17
BecauseofthesimilaritiesbetweengoutandFMF (auto-inflammatorydisease,short-livedintermittentarthritis,and good response to colchicine and anti-IL-1 treatments) we haveundertaken this study to findout whether thereis a relationwithMEFVmutations,causativegeneofFMF,ingouty patients.Werevealedthatcarriagerateandallelicfrequencies werenotdifferentbetweenthepatientandcontrolgroups.In literature,acaseofaJapanesepatientwithatypicalsymptoms ofgoutyarthritiswasreportedtocarryheterozygousE148Q mutation.18Tothe bestofourknowledgethereisnoother reportregardingtheassociationofMEFVandgout.Itisknown that certain MEFVmutations have severe clinical outcome suchastheassociationofamyloidosiswithM694Vgenotype inFMF.19Onthe otherhand,somereportsemphasizedthe
over-representation of E148Q in several inflammatory disorders.14 Inoursub-groupanalysisneitherM694Valone nortotalexon10mutationsweredifferentinthestudygroup. SimilarlyE148Qaloneandtotalexon2mutationswerealso not different between the patient and control groups. We alsodidnotshowanyassociationwithMEFVmutationsand disease phenotype such as nephrolithiasis and tophus. In additionoursubgroupanalysisrevealedthatthenumberof attacks, presenceof tophus, history ofnephrolithiasis and podagra were notdifferent betweenthe patients with and withoutmutations.Basedonthelatterfinding,someonemay suggestthatthepresenceofmutationsinthegoutyarthritis patientsmaynothaveaneffectondiseaseseverity.
Thisstudyhassomelimitationssuchassmallsamplesize oftotal197casesandcross-sectionalcollectionofdata.In con-clusion,despitetheselimitations,theresultspresentedinthis studydonotprovidesupportforamajorroleofMEFV muta-tions inTurkishgoutyarthritispatients.Furtherreplication studiesindifferentpopulationswithlargernumberofpatients areneededtoconfirmourresults.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BirlikM,GurlerO,AkarS,SariI,OnenF,AkkocN.The
prevalenceofgoutinanurbanareaofIzmir,Turkey:a
population-basedepidemiologicalstudy.IntJClinPract.
2014;68:775–82.
2.Perez-RuizF,CastilloE,ChinchillaSP,Herrero-BeitesAM.
Clinicalmanifestationsanddiagnosisofgout.RheumDisClin
NorthAm.2014;40:193–206.
3.PopeRM,TschoppJ.Theroleofinterleukin-1andthe
inflammasomeingout:implicationsfortherapy.Arthritis
Rheum.2007;56:3183–8.
4.SariI,BirlikM,KasifogluT.FamilialMediterraneanfever:an
updatedreview.EurJRheumatol.2014;1:21–33.
5.SamuelsJ,OzenS.FamilialMediterraneanfeverandtheother
autoinflammatorysyndromes:evaluationofthepatientwith
recurrentfever.CurrOpinRheumatol.2006;18:108–17.
6.OzenS,BilginerY,AktayAyazN,CalguneriM.
Anti-interleukin1treatmentforpatientswithfamilial
Mediterraneanfeverresistanttocolchicine.JRheumatol.
2011;38:516–8.
7.AtagunduzP,ErgunT,DireskeneliH.MEFVmutationsare
vascularinvolvement.ClinExpRheumatol.2003;214Suppl. 30:S35–7.
8. GiaglisS,MimidisK,PapadopoulosV,ThomopoulosK,
SidiropoulosP,RafailS,etal.Increasedfrequencyof
mutationsinthegeneresponsibleforfamilialMediterranean
fever(MEFV)inacohortofpatientswithulcerativecolitis:
evidenceforapotentialdisease-modifyingeffect?DigDisSci.
2006;51:687–92.
9. WallaceSL,RobinsonH,MasiAT,DeckerJL,McCartyDJ,YuTF.
Preliminarycriteriafortheclassificationoftheacutearthritis
ofprimarygout.ArthritisRheum.1977;20:895–900.
10.PrasM.FamilialMediterraneanfever:fromtheclinical
syndrometothecloningofthepyringene.ScandJ
Rheumatol.1998;27:92–7.
11.PunziL,ScanuA,RamondaR,OlivieroF.Goutas
autoinflammatorydisease:newmechanismsformore
appropriatedtreatmenttargets.AutoimmunRev.
2012;12:66–71.
12.AkkocN,SariI,AkarS,BinicierO,ThomasMG,WealeME,
etal.IncreasedprevalenceofM694Vinpatientswith
ankylosingspondylitis:additionalevidenceforalinkwith
familialmediterraneanfever.ArthritisRheum.
2010;62:3059–63.
13.AyazNA,OzenS,BilginerY,ErguvenM,TaskiranE,YilmazE,
etal.MEFVmutationsinsystemiconsetjuvenileidiopathic
arthritis.Rheumatology(Oxford).2009;48:23–5.
14.CaneteJD,ArosteguiJI,QueiroR,GratacosJ,HernandezMV,
LarrosaM,etal.AnunexpectedlyhighfrequencyofMEFV
mutationsinpatientswithanti-citrullinatedprotein
antibody-negativepalindromicrheumatism.ArthritisRheum.
2007;56:2784–8.
15.OzenS,Ben-ChetritE,BakkalogluA,GurH,TinaztepeK,
CalguneriM,etal.Polyarteritisnodosainpatientswith
FamilialMediterraneanFever(FMF):aconcomitantdiseaseor
afeatureofFMF?SeminArthritisRheum.2001;30:
281–7.
16.OzdoganH,ArisoyN,KasapcapurO,SeverL,CaliskanS,
TuzunerN,etal.VasculitisinfamilialMediterraneanfever.J
Rheumatol.1997;24:323–7.
17.KocaSS,EtemEO,IsikB,YuceH,OzgenM,DagMS,etal.
PrevalenceandsignificanceofMEFVgenemutationsina
cohortofpatientswithrheumatoidarthritis.JointBone
Spine.2010;77:32–5.
18.NonakaF,MigitaK,HaramuraT,SumiyoshiR,KawakamiA,
EguchiK.Colchicine-responsiveprotractedgoutyarthritis
withsystemicinflammatoryreactions.ModRheumatol.
2014;24:540–3.
19.KasifogluT,BilgeSY,SariI,SolmazD,SenelS,EmmungilH,
etal.AmyloidosisanditsrelatedfactorsinTurkishpatients
withfamilialMediterraneanfever:amulticentrestudy.