ISSN 2317-6431 https://doi.org/10.1590/2317-6431-2018-2061
Vocal behavior and working conditions of teachers after
speech therapy for treatment of behavioral dysphonia
Comportamento vocal e condições de trabalho de professores após
fonoterapia para tratamento de disfonia comportamental
Bárbara de Faria Morais Nogueira1, Adriane Mesquita de Medeiros1
ABSTRACT
Purpose: Check the vocal habits and changes in the working environment of teachers with functional dysphonia before and after participation in the Comprehensive Vocal Rehabilitation Program. Methods: Cross-sectional study using medical records of municipal teachers (step 1), and questionnaires after speech therapy (step 2). The 25 participants underwent speech therapy for functional dysphonia and answered the questionnaire over a period of at least six months after concluding the treatment. Data were collected through the retrospective analyses of the patients medical records, and by questionnaire via the internet. We performed a descriptive analysis and
McNemar, Wilcoxon and Test-t tests considering a significance level of
5%. Results: When comparing the time before and after the speech therapy, we found that teachers noticed a worsening in ventilation, temperature and noise originated with in the school. Teachers have increased the use of the microphone. They increased the practice of vocal warm-up and cool-down
after the speech therapy. There was no statistical significance between the groups in the parameters of the Protocol of the Profile of Participation and
activities. Conclusion: The vocal behavior and the work environment changed after the intervention. The use of vocal warm-up and cool-down after speech therapy increased, indicating that teachers are more aware about
the benefits of vocal exercises. The use of the microphone has increased,
but the amount of water consumed during the day is lower than expected.
Keywords: Dysphonia; Speech therapy; Faculty; Working conditions; Quality of life
RESUMO
Objetivo: Verificar as mudanças de hábitos vocais e na percepção do ambiente de trabalho dos professores com disfonia comportamental, após
participação no Programa Integral de Reabilitação Vocal. Métodos: Estudo
transversal realizado com prontuários de professores municipais (etapa 1) e com aplicação de questionário após alta fonoaudiológica (etapa 2).
Os 25 professores participantes realizaram fonoterapia para disfonia
comportamental e responderam ao questionário, no período mínimo de
seis meses após alta fonoaudiológica. A coleta de dados foi feita por
meio da análise retrospectiva dos prontuários dos pacientes e por envio de questionário via internet. Foi realizada análise descritiva e os testes McNemar, Wilcoxon e teste t, considerando nível de significância de 5%.
Resultados: Comparando o momento pré e pós-fonoterapia, verificou-se
que os professores perceberam piora na ventilação, temperatura e ruído originado dentro da escola, redução no relato de ruído originado na sala de aula e fora da escola, além de terem intensificado a utilização do microfone. Houve aumento da prática de aquecimento e desaquecimento vocal no momento após a fonoterapia. Não houve significância estatística entre os grupos nos parâmetros do protocolo Perfil de Participação e Atividades
Vocais. Conclusão: Ocorreram mudanças no comportamento vocal e na
percepção do ambiente de trabalho, após a reabilitação fonoaudiológica. O relato de realização do aquecimento e desaquecimento da voz, após
fonoterapia, aumentou, indicando que os professores mostraram-se mais
conscientes sobre os benefícios dos exercícios vocais. O uso do microfone foi mais frequente, porém, a quantidade de água ingerida durante o dia foi
aquém do esperado.
Palavras-chave: Disfonia; Fonoterapia; Docentes; Condições de trabalho; Qualidade de vida
Study carried out at Curso de Fonoaudiologia, Universidade Federal de Minas Gerais – UFMG – Belo Horizonte (MG), Brasil.
1 Departamento de Fonoaudiologia da Faculdade de Medicina, Universidade Federal de Minas Gerais – UFMG – Belo Horizonte (MG), Brasil.
Conflict of interests: No.
Contribution of authors: BFMN worked on the collection, analysis, interpretation of data and writing of the article; AMM worked on designing, analyzing, interpreting data and writing the article.
Funding: None.
Corresponding author: Bárbara de Faria Morais Nogueira. E-mail: barbaradffaria@gmail.com
INTRODUCTION
Voice disorders among teachers are of multicausal origin and related to individual, environmental and organizational factors, which can aggravate and/or trigger a vocal problem(1,2).
Behavioral dysphonia is highly prevalent in voice professionals, such as teachers(3).
Teachers often teach in inadequate conditions, for many hours a day, to a large number of students and in unfavorable environmental conditions(4). The aim of this study was to
verified the quality of life of teachers and found that the harmful working conditions, such as presence of competitive noise and inadequate acoustics in classrooms are associated with vocal complaints(5). These factors, added to the lack of vocal
preparation, such as inadequate vocal adjustments and little awareness about voice care, collaborate for these professionals to present high prevalence of vocal signs and symptoms and voice alterations(6).
Given the occupational challenges they face for effective performance in their workday, teachers need to use their voice for a long time, without adequate rest, to raise their voice to overcome loud noise in the school environment and in the classroom, maintaining healthy habits, such as adequate hydration and feeding, among other challenges(7). A study(8) has
indicated that the main complaints of vocal problems reported by teachers were related to sore throat, hoarseness, temporary voice loss and the medical diagnosis of nodules in vocal folds.
Vocal rehabilitation can occur by combining the indirect approach, which involves change in cognition, behavior and environment in which the patient uses his voice, with the direct approach, which includes vocal techniques aimed at achieving balanced muscle adjustment. The indirect approach occurs in almost a third of the therapy session. Stress management and coaching strategies, relaxation techniques, advice on the use of voice, vocal education and evaluation of environmental aspects that may be related to vocal overload can be used(3).
Thus, adherence to treatment is important for achieving therapeutic success and for avoiding recurrence of the voice problem. According to an investigation(9), adherence to treatment
is fundamental as it will prevent laryngeal changes that develop into dysphonic conditions, consequently resulting in work leaves.
In research(10) that used the Comprehensive Vocal Rehabilitation
Program (PIRV) in teachers with behavioral dysphonia, it was observed that, after the program, there was improvement in clinical aspects and vocal self-perception. Another study, using the same program, showed that participants had good adherence and satisfaction with this means of intervention(11). It is known
that phonoaudiological intervention for dysphonia points to positive long-term effects on the voice quality of teachers who have been discharged from speech therapy(7).
The aim of the present study was to verify changes in vocal habits and in the perception of the working environment of teachers with behavioral dysphonia after the minimum period of six months of discharge from PIRV.
METHODOLOGY
This is an observational cross-sectional study approved by the Research Ethics Committee - COF - UFMG, under protocol number 1.160.687. The research followed the norms of Resolution CNS 446/2011 of the National Health Council.
Participants were submitted to speech therapy for functional dysphonia, and after discharged from speech therapy, accepted to participate in the study for a period of at least six months. Teachers were assisted in the extension project “Professional Voice Improvement”, which aims to promote assistance to the demand of teachers with behavioral dysphonia and uses the Comprehensive Vocal Rehabilitation Program (PIRV) described in literature(12) as intervention proposal. After medical
and phonoaudiological assessment, teachers of the municipal education network are referred to the Speech-Language Outpatient Clinic of a federal public university. More information about the project can be found in a previously published study(11).
The treatment offered in the university service consists of eight sessions. The first session is used to promote the therapist / patient relationship, to perform anamnesis through questionnaire containing personal data, vocal and health behavior, questions about the work, performance of perceptive-auditory and acoustic evaluations of the voice and the application of protocols, including the Voice Activity and Participation Profile - VAPP, which is an instrument used to assess the impact of voice on quality of life(13,14). This protocol is easy to apply and
provides a better description of the degree of functional disability related to the use of voice, and the higher the result, the greater the difficulty imposed and restriction in the participation of vocal activities(15). PIRV is initiated in the second session.
From the second to the seventh session, vocal orientations, vocal psychodynamics and vocal training are carried out through exercises that include five aspects: body-voice, glottal source, resonance, pneumophonoarticulatory coordination and communicative attitude(12). At the eighth and final sessions,
teachers are re-evaluated through perceptual-auditory and acoustic assessment of voice, VAPP reapplication and also received guidance on vocal warm-up and vocal relaxation exercises. Interventions are carried out in homogeneous groups composed of a maximum of three participants. However, in order for the teacher to participate in the program, it is mandatory to present the medical report of the laryngeal examination to confirm the presence of functional dysphonia.
Inclusion criteria were: to be a teacher, to have no laryngeal lesion, to have vocal symptoms, to have speech-language pathology treatment discharge for at least six months, to be referred by the municipal occupational health service, to work at any level of education and work shift, and to agree in participating in the research. Exclusion criteria were: teachers with another type of speech, voice or language disorder, sung voice professionals and professionals with history of diagnosis of neurological problems or recent acute laryngeal conditions.
Of the total of 34 teachers attended by PIRV in the period of three academic semesters, 25 accepted to participate in the study. Non-participation was due to the impossibility of telephone contact, or because they accepted, received the questionnaire, but did not respond.
applied at least six months after speech-language intervention. It is emphasized that the questionnaire used in the project is standardized for application in all teachers. In the second stage of the research, the same questionnaire was sent back to participants.
In both phases, the questionnaire contained information regarding age, gender (female and male), teaching cycle (one cycle and two cycles or more), work shifts (one shift and two shifts), profession time (up to 11 years and 12 years or more) and VAPP (self-perception of the vocal problem, effects of dysphonia on the teaching activity, daily communication, social communication and emotion, as well as additional scores on the Activity Limitation Score (PLA) and the Participation Restriction Score (PRP)(13,14).
Regarding working environment conditions, variables ventilation (satisfactory and reasonable / poor), temperature (satisfactory and reasonable / poor), noise originated in the classroom, and outside the school (neglectable / reasonable and high / unbearable), use of microphone and chalkboard (always / often, sometimes and never). Regarding vocal behavior and health condition, variables hydration during classes (yes and no), water intake per day (more than three liters / two and three liters, less than two liters and never), physical activity on days per week (three or more and none / one or two), intense voice use beyond the teaching activity (yes and no), upper airway infection (never / rarely and sometimes / frequently), diagnosis of gastroesophageal reflux (yes / no) and performance of vocal warm-up and vocal relaxation exercises (always / often, sometimes and never).
For this research, the events of interest were the comparison of vocal behavior, work environment perception and pre- and post-speech therapy VAPP. After analyzing medical records and questionnaires, information was entered into a database in the Microsoft Office Excel software. Analyses were performed on IBM - SPSS Statistic Base software, version 19.
For the compilation of results, descriptive analysis of the categorical variables was performed through frequency distribution and the numerical synthesis of quantitative variables.
The measures of association between pre- and post-speech therapy categorical variables were performed using the McNemar test. The measures of association between pre- and post-speech therapy quantitative variables were performed using the Wilcoxon test and t-test. In all tests, 5% significance level was adopted.
RESULTS
The research was carried out with 25 teachers, the majority being female (92%), teaching in one teaching cycle (56%), in two work shifts (76%), with profession time of 11 years or more (56%) (Table 1). The mean age of teachers was 38 years (standard deviation = 8.16).
Comparing the pre- and post-speech therapy moments, it was verified that teachers observed a worsening in ventilation, temperature and noise originated in the school. There was a decrease in noise reported in classroom and outside the school. Regarding the use of the microphone, teachers intensified the use of this resource and the use of the chalkboard remained unchanged (Table 2).
Regarding vocal behavior and health condition, at the post-speech therapy moment, most teachers reported hydration during class (84%), intense voice use beyond the teaching activity (92%) and presence of upper airway infection (56%).
In relation to the amount of water consumed during the day (64%), the intake of less than 2 liters was predominant and 16% of teachers practiced physical activity on 3 or more days per week. Approximately 1/3 of teachers (32%) reported diagnosis of gastroesophageal reflux. The performance of vocal warm-up and vocal relaxation exercises (87%) by teachers increased at the time after speech therapy (Table 3).
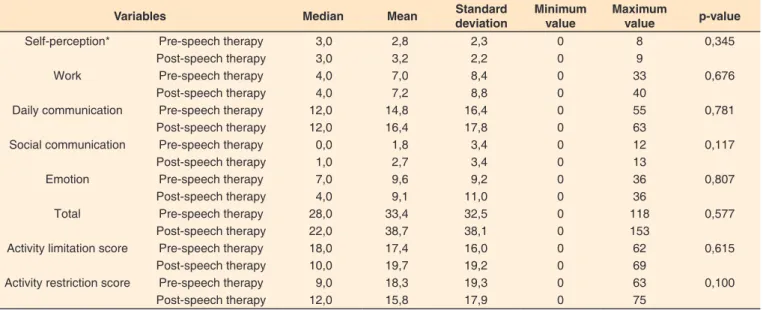
There was no difference between pre- and post-speech therapy moments, as well as in the VAPP parameters of self-perception, work, daily and social communication and emotion, as well as additional scores on the Activity Limitation Score and the Participation Restriction Score (Table 4).
Table 1. Characteristics of the work of teachers with behavioral dys-phonia at the time of speech therapy discharge
Work characteristics n %
Number of teaching cycle
One 14 56
Two or more 11 44
Number of work shift
One 06 24
Two 19 76
Profession time (years)
Up to 11 11 44
11 or more 14 56
Table 2. Frequency distribution and association analysis of teacher’s perception of pre- and post- speech therapy work environment (minimum interval of six months)
Perception of the work environment
Pre Post
p-value
n % n %
Ventilation
Satisfactory 13,0 52,0 8,0 32,0 0,180
Fair / poor 12,0 48,0 17,0 68,0
Temperature
Satisfactory 10,0 40,0 5,0 20,0 0,267
Fair / poor 15,0 60,0 20,0 80,0
Noise originated in the classroom*
Negligible / Reasonable 8,0 33,0 11,0 44,0 0,508 High / Unbearable 16,0 67,0 14,0 56,0 Noise originated in the school*
Negligible / Reasonable 14,0 58,3 12,0 48,0 0,687 High / Unbearable 10,0 41,7 13,0 52,0 Noise originated outside the school*
Negligible / Reasonable 19,0 79,2 23,0 92,0 0,125 High / Unbearable 5,0 20,8 2,0 8,0 Microphone use*
Always / frequently / sometimes 5,0 20,8 10,0 41,7 0,219
Never 19,0 79,2 14,0 58,3
Chalkboard*
Always / frequently / sometimes 9,0 39,1 10,0 40,0 1,000
Never 14,0 60,9 15,0 60,0
McNemar Test.
DISCUSSION
Adequate working environment conditions and vocal care are essential for maintaining vocal health. In the present study, it was verified that ventilation, temperature and school noise were perceived by teachers as worse after the end of the speech therapy for behavioral dysphonia. This worsening may be related to the structural conditions of the work environment, or to the
greater awareness of teachers regarding environmental factors detrimental to voice after the speech-language intervention. Teachers in poor working environments, with presence of noise and inadequate classroom infrastructure, for example, are more vulnerable to vocal symptoms(16). However, even with
better vocal behaviors and greater vocal resistance achieved in speech-language rehabilitation with more adequate phonological adjustments, teachers may remain at risk of developing behavioral dysphonia.
Table 4. Comparison of the means of the pre- and post-speech therapy Voice Activity and Participation Profile parameters (minimum 6 months)
Variables Median Mean Standard
deviation
Minimum value
Maximum
value p-value
Self-perception* Pre-speech therapy 3,0 2,8 2,3 0 8 0,345
Post-speech therapy 3,0 3,2 2,2 0 9
Work Pre-speech therapy 4,0 7,0 8,4 0 33 0,676
Post-speech therapy 4,0 7,2 8,8 0 40
Daily communication Pre-speech therapy 12,0 14,8 16,4 0 55 0,781
Post-speech therapy 12,0 16,4 17,8 0 63
Social communication Pre-speech therapy 0,0 1,8 3,4 0 12 0,117
Post-speech therapy 1,0 2,7 3,4 0 13
Emotion Pre-speech therapy 7,0 9,6 9,2 0 36 0,807
Post-speech therapy 4,0 9,1 11,0 0 36
Total Pre-speech therapy 28,0 33,4 32,5 0 118 0,577
Post-speech therapy 22,0 38,7 38,1 0 153
Activity limitation score Pre-speech therapy 18,0 17,4 16,0 0 62 0,615
Post-speech therapy 10,0 19,7 19,2 0 69
Activity restriction score Pre-speech therapy 9,0 18,3 19,3 0 63 0,100
Post-speech therapy 12,0 15,8 17,9 0 75
*Test t. Wilcoxon test
Table 3. Frequency distribution and analysis of association of vocal behavior and pre- and post- speech therapy health conditions (minimum interval of six months)
Life habits characteristics Pre Post p-value
n % n %
Hydration during classes
Yes 22 88,0 21,0 84,0 1,000
No 3,0 12,0 4,0 16,0
Amount of water consumed per day (in liters)
More than three / two and three 11,0 44,0 9,0 36,0 0,625
Less than two / never 14,0 56,0 16,0 64,0
Practice of physical activity (days per week)
Three or more 9,0 36,0 4,0 16,0 0,063
Never / one or two 16,0 64,0 21,0 84,0
Intense use of voice beyond teaching
Yes 23,0 92,0 23,0 92,0 1,000
No 2,0 8,0 2,0 8,0
Upper airway infection
Never / rarely 7,0 28,0 11,0 44,0 0,219
Sometimes / frequently 18,0 72,0 14,0 56,0
Diagnosis of gastroesophageal reflux
Never / rarely 17,0 68,0 17 68,0 1,000
Sometimes / frequently 8,0 32,0 8,0 32,0
Performance of vocal warm-up and vocal relaxation exercises*
Always / frequently / sometimes 9,0 36,0 21,0 87,5 <0,001**
Never 16,0 64,0 3,0 12,5
The results showed that there was a decrease in the noise originated in classroom at the post-speech therapy moment, but with no difference between groups. The teacher’s awareness of vocal exhaustion generated by noise may allow the use of strategies to avoid voice hypersolicitation in classroom. Among the strategies described in literature to reduce noise in classroom, the decrease in the number of students per classroom, diversification of classes and students’ awareness stand out(17).
This study showed an increase in the use of microphones by teachers. The use of this device has been shown to be an efficient strategy for vocal comfort and longevity of the voice professional and is an alternative way for voice professionals with vocal alterations(18). Moreover, the use of a sound amplifier,
when well oriented, suggests benefits due to the reduction of vocal effort(19). Studies have encouraged the incorporation of
the microphone as a prophylactic measure, that is, an individual protection equipment for the teacher(19,20).
Hydration and the performance of vocal warm-up and vocal relaxation exercises showed beneficial adhesions to the speech-language pathology, according to some investigations(21,22).
Hydration efficacy for good vocal production is considered one of the important factors in the reduction of vocal complaints and, consequently, in the improvement of vocal production(7,23).
Most teachers in the present study reported hydration during class; however, they reported drinking less than two liters of water per day. Hydration is beneficial for improving vocal quality and the intake of two liters of water per day is widely reported in vocal health promotion and rehabilitation actions(24,25), but without
proven scientific evidence. Thus, hydration difficulty with regard to quantity needs to be analyzed with caution. Individual and environmental aspects should be considered, as it is not known whether teachers performed hydration supplementation through the ingestion of other liquids, felt the need to drink more or less liquid, if water was available in the work environment, if they avoided continuous use while they were teaching, so that they did not have to leave the classroom, and what the weather was like at the time of the research.
Among the factors analyzed, the increase in the performance of vocal warm-up and relaxation exercises, comparing the pre- and post-speech therapy moments, did not occur at random. The results showed that teachers started to perform warm-up and relaxation exercises more frequently after learning about the importance of these exercises for vocal health, receiving guidance during speech therapy. It is known that the warm-up of vocal fold muscles through breathing and voice exercises before intense activity avoids vocal fatigue that can cause lesions in the long term(26).
In relation to the practice of physical activity, few teachers mentioned performing it three or more days a week. An investigation(27) has shown that teachers who do not practice
physical activity are more likely to have vocal disorders compared to those who exercise three or more times a week. There is little scientific evidence for a better understanding of such a voice benefit.
In a study(28) aimed at developing the Brazilian version of
the Vocal Activity and Participation Profile (VAPP) protocol, it was shown that, after speech therapy, there is reduction in most VAPP scores, mainly in participants with organofunctional dysphonia. The results of the present study showed that the mean values found in most aspects of VAPP were lower than the previously mentioned study, a fact that may be related to sample characteristics, exclusively composed of teachers, with
no lesions in vocal folds, and with low impact of voice on quality of life. Regarding the low impact of voice on quality of life at the beginning of treatment, it is expected that, after speech therapy discharge, this result shows little difference in the VAPP scores, as observed in this investigation. In a study(7),
it was verified that speech therapy for dysphonia has positive effects in the long term, in the analysis of the VAPP of teachers who were discharged, and negative for those who abandoned treatment, in a follow-up time of two years, on average.
Although the results of the study demonstrated that speech-language rehabilitation contributes to the adoption of adequate vocal behaviors for vocal health maintenance, the convenience sample does not allow these results to be generalized to the teacher population. It was verified that, despite the restricted number of sessions (eight), the PIRV method showed that teachers adopted microphone use and vocal warm-up and relaxation exercises.
The increase of scientific evidence with this occupational group; however, strengthens the establishment of measures for vocal health maintenance. It is necessary to carry out periodic vocal health promotion and disease prevention programs in order to reinforce such guidelines. In research focused on vocal health actions, it was observed that teachers create expectations for the meetings in order to learn vocal exercises, aiming to reduce laryngeal symptoms(29). The research also emphasized
the importance of performing these practices, so that they can be incorporated into the daily life of these professionals. In addition, the result of exercise can be immediate through the change of vocal quality, which can bring a feeling of well-being. Significant changes in vocal behavior become limited, especially when the teacher acts in environmental and work organization conditions considered unhealthy.
The poor conditions of the teachers’ work organization, which may be responsible, more than environmental conditions, for their vocal illness, were not included in this study. It is also important to carry out multi-center studies with larger number of participants.
CONCLUSION
There were changes in vocal behavior and in the perception of the work environment after speech therapy discharge from rehabilitation for behavioral dysphonia. The performance of vocal warm-up and relaxation exercises after speech therapy increased, indicating that teachers are more aware of the benefits of vocal exercises. Microphone use was more frequent; however, the amount of water consumed during the day was lower than recommendations.
REFERENCES
1. Simões-Zenari M, Bitar ML, Nemr NK. The effect of noise on the voice
of preschool institution educators. Rev Saude Publica. 2012;46(4):657-64. PMid:22715003.
2. Xavier IALN, Santos ACO, Silva DM. Vocal health of teacher:
3. Behlau M. The 2016 G. Paul Moore Lecture: lessons in voice rehabilitation: journal of voice and clinical practice. J Voice. 2018;8:2-13. PMid:29567050.
4. Zambon F, Moreti F, Vargas ACT, Behlau M. Eficiência e valores de corte do Perfil de Participação e Atividades Vocais para não
professores e professores. CoDAS. 2015;27(6):598-603. http://dx.doi. org/10.1590/2317-1782/20152015028. PMid:26691625.
5. Casella JGC, Afonso MLM. Qualidade de vida docente: relação entre alterações psicoemocionais e disfonias. Rev Pedagógica.
2018;20(43):168-82. http://dx.doi.org/10.22196/rp.v20i43.3844.
6. Behlau M, Zambon F, Guerrieri AC, Roy N. Epidemiology of voice
disorders in teachers and nonteachers in Brazil: prevalence and adverse effects. J Voice. 2012;26(5):9-18. http://dx.doi.org/10.1016/j. jvoice.2011.09.010. PMid:22516316.
7. Ferreira LP, Latorre MRDO, Giannini SPP, Ghirardi ACAM, Karmann DF, Silva EE. Influence of abusive vocal habits, hydration, mastication,
and sleep in the occurrence of vocal symptoms in teachers. J Voice. 2010;24(1):86-92. http://dx.doi.org/10.1016/j.jvoice.2008.06.001. PMid:19135852.
8. Araújo TMD, Martins FC. Condições de trabalho docente e saúde na
Bahia: estudos epidemiológicos. Educ Soc. 2009;30(107):427-49. http://dx.doi.org/10.1590/S0101-73302009000200007.
9. Gama ACC, Bicalho VS, Valentim AF, Bassi IB, Teixeira LC, Assunção AA. Adesão a orientações fonoaudiológicas após a alta do tratamento
vocal em professores: estudo prospectivo. Rev CEFAC. 2012;14(4):714-20. http://dx.doi.org/10.1590/S1516-18462011005000105.
10. Cavalcanti NR, Souza BO, Gama ACC, Medeiros AM. Efeito
do programa integral de reabilitação vocal em professoras com
disfonia comportamental. CoDAS. 2018;30(4):170-82. http://dx.doi. org/10.1590/2317-1782/20182017182. PMid:30088521.
11. Souza BO, Tono IBG, Souza EVS, Silva SP, Nogueira BFM, Ribeiro K, et al. Adesão e satisfação de professores participantes do Programa Integral de Reabilitação Vocal. Distúrb Comun. 2017;29(2):284-91.
http://dx.doi.org/10.23925/2176-2724.2017v29i2p284-291.
12. Behlau M, Pontes P, Vieira VP, Yamasaki R, Madazio G. Apresentação do Programa Integral de Reabilitação Vocal para o tratamento das
disfonias comportamentais. CoDAS. 2013;25(5):492-6. http://dx.doi. org/10.1590/S2317-17822013000500015. PMid:24408556.
13. Ferreira JM, Campos NF, Bassi IB, Santos MAR, Teixeira LC, Gama
ACC. Analysis of aspects of quality of life in teachers’ voice after discharged: longitudinal study. CoDAS. 2013;25(5):486-91. http:// dx.doi.org/10.1590/S2317-17822013000500014. PMid:24408555.
14. Góes TRV, Ferracciu CCS, Silva DRO. Association between the adherence to voice therapy and voice activity profile in patients with behavioral dysphony. CoDAS. 2016;28(5):595-601. PMid:27812672.
15. Kleemola L, Helminen M, Rorarius E, Sihvo M, Isotalo E. Twelve-month
clinical follow-up study of voice patients´ recovery using the Voice Activity and Participation Profile (VAPP). J Voice. 2011;25(5):245-54. PMid:21050712.
16. Phadke KV, Abo-Hasseba A, Svec JG, Geneid A. Influence of
noise resulting from the location and conditions of classrooms and schools in upper egypt on teachers’ voices. J Voice. 2018. No prelo. PMid:29731381.
17. Libardi A, Gonçalves CGO, Vieira TPG, Silverio KCA, Rossi D, Penteado RZ. O ruído em sala de aula e a percepção dos professores
de uma escola de ensino fundamental de Piracicaba. Distúrb Comun. 2006;18(2):167-78.
18. Roy N, Weinrich B, Gray SD, Tanner K, Toledo SW, Dove H, et al.
Voice amplification versus vocal hygiene instruction for teachers with voice disorders: a treatment outcomes study. J Speech Lang Hear Res. 2002;45(4):625-38. http://dx.doi.org/10.1044/1092-4388(2002/050). PMid:12199394.
19. Teixeira LC, Behlau M. Comparison between vocal function exercises and voice amplification. J Voice. 2015;29(6):718-26. http://dx.doi. org/10.1016/j.jvoice.2014.12.012. PMid:26296853.
20. Gomes NR, Medeiros AM, Teixeira LC. Self-perception of working conditions by primary school teachers. Rev CEFAC. 2016;18(1):167-73. http://dx.doi.org/10.1590/1982-021620161819515.
21. Santos SMM, Medeiros JSA, Gama ACC, Teixeira LC, Medeiros AM. Voice impact in the social communication and emotion of teachers before and after speech therapy. Rev CEFAC. 2016;18(2):470-80. http://dx.doi.org/10.1590/1982-0216201618211015.
22. Siqueira MA, Bastilha GR, Lima JPM, Cielo CA. Hidratação vocal em
profissionais e futuros profissionais da voz. Rev CEFAC. 2016;18(4):908-14. http://dx.doi.org/10.1590/1982-0216201618417415.
23. Medeiros AM, Assunção AA, Barreto SM. Alterações vocais e cuidados
de saúde entre professoras. Rev CEFAC. 2012;14(4):697-704. http:// dx.doi.org/10.1590/S1516-18462011005000146.
24. Hermes EGC, Bastos PRHO. Prevalence of teacher’s voice symptoms in municipal network education in Campo Grande - MS. Rev CEFAC. 2015;17(5):1541-55. http://dx.doi.org/10.1590/1982-021620151751215.
25. Aydos B, Hanayama EM. Técnicas de aquecimento vocal utilizadas por professores de teatro. Rev CEFAC. 2004;6(1):83-8.
26. Assunção AA, Medeiros AM, Barreto SM, Gama AC. Does regular
practice of physical activity reduce the risk of dysphonia? Prev Med. 2009;49(6):487-9. http://dx.doi.org/10.1016/j.ypmed.2009.09.006. PMid:19778552.
27. Ricarte A, Oliveira G, Behlau M. Validação do protocolo Perfil de Participação e Atividades Vocais no Brasil. CoDAS. 2013;25(3):242-9.
http://dx.doi.org/10.1590/S2317-17822013000300009. PMid:24408335.
28. Ferreira LP, Alves IAV, Esteves AAO, Biserra MP. Alterações vocais e
cuidados de saúde entre professoras. Distúrb Comun. 2012;24(3):379-87.
29. Silverio KCA, Gonçalves CGO, Penteado RZ, Vieira TPG, Libardi A, Rossi D. Ações em saúde vocal: proposta de melhoria do perfil vocal de professores. Pró-Fono Revista de Atualização Científica.