Lygia Carmen de Moraes VanderleiI
María Luisa Vázquez NavarreteII
I Programa de Pós-Graduação em Avaliação
em Saúde. Instituto de Medicina Integral Prof. Fernando Figueira. Recife, PE, Brasil
II Servei d’Estudis i Prospectives en Polítiques
de Salut. Consorci de Salut i Social de Catalunya. Barcelona, Cataluña, Espanha Correspondence:
Lygia Carmen de Moraes Vanderlei Instituto de Medicina Integral Prof. Fernando Figueira (IMIP)
Diretoria de Ensino
Rua dos Coelhos, 300 Boa Vista 50070-550 Recife, PE, Brasil E-mail: [email protected] Received: 9/30/2011
Approved: 10/7/2012
Article available from: www.scielo.br/rsp
Preventable infant mortality and
barriers to access to primary care
in Recife, Northeastern Brazil
ABSTRACT
OBJECTIVE: Analyze the factors infl uencing avoidable infant mortality from the perspective of the protagonists involved.
METHODS: Qualitative study with a critical-constructivist approach, examining children’s access to health care and avoiding preventable infant mortality through health care campaigns and services in Health District I of Recife, Northeastern Brazil, between February 2007 and February 2008. The theoretical sample was designed in two stages: I) institutions providing health services to children; II) interviewees: managers (11); professionals [from the Family Health Strategy and Programme of Community Health Workers (48); and from outpatient clinics (12)]; mothers (20), with sample size defi ned by “saturation of the speeches”. Data was collected using individual semi-structured interviews and case studies of avoidable infant death. Thematic content analysis was used, generating mixed categories (emerging and scripted).
RESULTS: There were perceived to be confl icting positions between different stakeholder groups refl ecting their role in the care network. All institutional participants related infant deaths to the absence/poor dissemination of child health policies and inter-sectoral actions; professionals and mothers highlighted diffi culties in accessing health care due to insuffi cient global resources, especially the lack of doctorsinFamily Health Strategy, shifting health care to nurses. Lack ofdoctors,acutediseases rejection, and dehumanized and/or poortechnical quality carewere the mainfactors which the mothers relatedto deaths. Family Health Strategy participants from the Programme of Community Health Workers and mothers identifi ed thecondition ofsocial exclusionand maternal neglectwith deaths, but the case studyof deathrevealedthe association withlowerquality of care offered.
CONCLUSIONS: Numerous barriers to access indicate insuffi cient Brazilian Unifi ed Health System implementation and lack of resolution of the main access route, the Family Health Strategy. The results indicate the need for improvement of structural and organizational factors of supply, with emphasis on mechanisms to stimulate the recruitment of doctors for the Family Health Strategy professional training of all staff consistent with the model of care to comply with health care policies for children and avoiding preventable infant mortality.
Over the last three decades, the Brazilian government has shown great interest in reducing infant mortality through the introduction of programs, plans and projects.25,a These activities, together with a signifi
-cant decrease in fecundity over the same period, have contributed to a decline in fi gures for infant mortality. However, the number of preventable infant deaths in the country remains considerable.9,12,13
There is a strong link between preventable infant death and timely access to health care services, as preventable deaths, according to Rutstein et al19 (1976), are defi ned
as “deaths which could be partially or totally avoided by the presence of effective health care services”. The emphasis is even greater when the scene of these deaths is a regional hub city, constitutionally bound to provide universal access and comprehensive health care according to the precepts of the SUS (Brazilian Unifi ed Health System).25,a
Child health care policies, in accordance with these principles, aim to provide health care which is resolu-tory, welcoming, humane and accountable, provided by teams working together and with intersectoral cooperation, preferably offered by the Family Health Strategy (ESF) and the Program of Community Health Workers (PACS). The objective is to promote health and reduce infant mortality.b It is the duty of the health care
team to monitor the child throughout their fi rst year, to identify at birth risk factors for illness and death (low birth weight, premature birth, hypoxia, teenage mothers and mothers with low levels of schooling and family history of death before age fi ve) and decide upon the appropriate medical care.c Also taken into consideration
as risk factors are previous hospital admissions, delays in vaccination, living in risk areas, having no income and drug addiction.
In line with the national pattern, the infant mortality coeffi cient (IMC) for Recife, Northeastern Brazil, show a progressive reduction (IMC = 13 deaths/1,000 live births in 2007), similar to that seen in other, more developed, Brazilian cities such as Rio de Janeiro, São Paulo and Belo Horizonte, all located in Southeastern Brazil. However, 86% of these deaths could have been prevented by actions on the part of the health sector or partner organizations in other social sectors. This suggests the existence of barriers to access to health care services and campaigns.d
INTRODUCTION
The extensive literature which relates to infant deaths which could have been prevented through access to health care services, makes use of epidemiological or evaluative methods as the principal investigative tool. While these methods demonstrate the magnitude of the problem,9,12,13,23 they do not deepen the perspective of
the social protagonists (users, health care professionals) or contextual factors (political and characteristics of supply) which infl uence access.
The majority of qualitative studies concentrate on barriers relating to the performance of health care professionals in welcoming and connecting,21,22 or on
the maternal perspective of infant death,10,15,20 and few
analyze the infl uence of barriers to access on the ongoing occurrence of avoidable deaths, or else do not include the points of view of all the participants involved.
Access to health care refers to the possibility of obtaining health care, conveniently and easily, when they need it.1 As access is something that can only
be observed when health care services are actually used by those who need them, Aday & Andersen’s2
(1974) theoretical model analyzes factors which infl uence use of health care services, defi ning the two most important dimensions of access: potential and realized. Potential access is concerned with the characteristics of supply (availability and organiza-tion of health care services) and of the users: predis-posing factors (sociodemographic characteristics, beliefs and attitudes, level of information); enabling factors (personal and community) and health care needs. Realized access refers to actual use of health care services.2
The aim of this study was to analyze factors which infl uence preventable infant mortality, from the pers-pective of all participants involved in the phenomenon.
METHODS
This was a qualitative, descriptive-interpretive study using a critical-constructivist approach,11,14 aiming to
uncover the relationship between children’s access to health care and infant death which could be prevented by actions and health care services,using Aday & Andersen’s2 (1974) theoretical framework
to analyze access. The fi eld work, the largest part
a Frias PG, Mullachery PH, Giugliani ERJ. Políticas de saúde direcionadas às crianças brasileiras: breve histórico com enfoque na oferta de
serviços de saúde. In: Ministério da Saúde, Secretaria de Vigilância em Saúde, Departamento de Análise de Situação em Saúde. Saúde Brasil 2008: 20 anos do Sistema Único de Saúde (SUS) no Brasil. Brasília (DF); 2009. p.85-110. (Série G. Estatística e Informação em Saúde).
b Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Ações Programáticas Estratégicas. Agenda de compromissos para a
saúde integral da criança e a redução da mortalidade infantil. Brasília (DF); 2005. (Série A. Normas e Manuais Técnicos).
c Ministério da Saúde, Secretaria de Políticas de Saúde, Departamento de Atenção Básica. Saúde da Criança: acompanhamento do
crescimento e desenvolvimento infantil. Brasília (DF); 2002.
d Secretaria Municipal de Saúde do Recife, Diretoria de Vigilância à Saúde, Gerência de Epidemiologia. Perfi l epidemiológico da criança e do
of the research,e took place between February 2007
and February 2008 in Health District 1 of Recife, Northeastern Brazil, as it had the highest IMC fi gures during the period.
A two-stage theoretical sample was designed.6 The
following institutions were selected: Health District 1 Administrative Headquarters; Primary Health Care Services (nine ESF units and one Traditional Primary Care Unit [UBT], which provide health care according to the traditional model, with basic children’s health care provided by pediatricians and without being ascribed to areas); and services of medium complexity (two outpatients clinics and an Allergology Service, which offered primary health care within the traditional model, as well as specialized health care). Ninety-one interviewees were selected, aiming for the greatest possible variety of discourse in order to guarantee sample suffi ciency and saturation.6,11,14
A two-part collection strategy was used to collect data: a) individual, semi-structured interviews (scripted according to the theoretical framework) with partici-pants associated with the institutions and mother of children aged between 28 and 365 days. Ninety-one interviewees took part: 11 managers – nine district managers (M) and two unit managers (Geradm); 48 health care professionals from PACS and ESF: ten doctors (MED); 12 nurses (N); 26 Community Health Workers (ACS), 20 from ESF (PSF) and six from PACS; four outpatient clinic general managers (UB), one UBT director and seven pediatricians from outpa-tient clinics (PED); 20 mothers; b) a case study of a preventable, post-natal infant death. The areas of Health District 1 with the highest occurrence for post-natal infant death classifi ed as preventable were identifi ed; 18 events which occurred during the period in question were analyzed in order to select those which best exem-plifi ed problems with health care access culminating in a death which could have been avoided. In order to build the case, the following methods were used: examining ante-natal care cards completed by doctors and nurses in ESF units; examining medical records for mother and child appointments in maternity and pediatric hospitals; looking at notes from ACS home visits to mother and child; examining child’s growth and development and vaccination records; examining records from child’s appointments and referrals by the ESF; examining child’s death certifi cate from the Institute of Legal Medicine; individual, semi-structured interviews which health care professionals involved in child’s care and the death (ACS, doctors and nurses from ESF); and non-structured interviews with mother. Two interviews were necessary in order to establish a satisfactory relationship conducive to dialogue. The interviews took into account the mother’s wishes as
to the details revealed about the events leading to her daughter’s death and took place at a time and place convenient to her.
The interviews lasted between 30 and 60 minutes, and were recorded and transcribed and accompanied by the fi eld diary.
Thematic content analysis was carried out, with a topic deemed to be a unit of meaning, taken from the text according to criteria from the theoretic-concep-tual framework.4 Mixed categories were produced
(scripted and emerging). The quality of the data was guaranteed by triangulation between groups of inter-viewees, techniques and strategies of data collection and an external analysis.6,11
The categories and sub-categories for analyzing access where those which the social protagonists associated with infant mortality: a) Factors related to SUS policies: implementation; dissemination, infant health programs; inter-sectoral actions; b) Factors concerned with the structure of supply: availability of human and material resources; c) Factors concerned with the organization of supply and professional performance: preventive and curative care (location; professional providing care); aspects of care (welcoming/humane/technical quality); d) Factors concerned with social context: social conditions of the families and the environment; social support networks.
The research was approved by the Instituto de Medicina Integral Prof. Fernando Figueira (IMIP), Committee of Ethical Research in Humans, process nº 892, 2006. All of the participants signed consent forms.
RESULTS
The majority of the participants were women; of the ten men interviewed, two were managers, three were health care unit directors, three were ACS and two were doctors. The interviewees from the institutions had been carrying out their work for between fi ve and ten years, with the extremes represented by ACS from PACS and health care professionals from the outpatient clinics and the UBT (traditional model), who had been working there for more than 15 years, and for a doctor and ACS from ESF, where some members of the team had been there for a year. The 21 mothers interviewed were aged between 17 and 38; nine of them lived with their child’s father; 13 had not completed primary education, one had fi nished high school and two had steady employment; nine were employed informally and ten reported they were not working; monthly household income was of one minimum wage, with this being supplemented by benefi ts.
e Moraes Vanderlei LC. Mortalidad infantil evitable y acceso a la atención de la salud en Recife, Brasil en la perspectiva de los principales
For the majority of the interviewees, clear barriers to access emerged throughout the continuous care. The basic level stands out, with important differences in the level of intensity of the discourse, depending on the group from which it came. Four groups of barriers feedback into themselves, with repercussions on the avoidance of preventable infant mortality.
Infant death and SUS policies
The majority of participants from institutions related the persistence of deaths to barriers due to the SUS care model, including policies dealing with children’s health, not being properly established. However, there was disagreement among the different groups. The majority of participants from the traditional model (professionals from the UBT and the outpatient clinics) were unaware of policies aimed at infant health, emphasizing the effective absence of children’s health programs in the municipality; managers and profes-sionals from the ESF/PACS highlighted the fragility
of inter-sectoral cooperation. The mothers perceived the low problem solving capabilities of the ESF to be contributing factors. However, there were narratives about the decline in deaths being utilized by ESF/PACS, especially between members of these teams (Table 1).
Infant deaths and structural and organizational factors of supply
Almost all of the interviewees perceived the overall scarcity of resources to be prejudicial to access to preventive and curative health care. The groups had different perspectives regarding the outcome of infant death. For PACS/ESF health care professionals, infant mortality was linked to the large number of families the ESF teams were responsible for, meaning the health care professionals were overstretched. This would lead to programmed activities, such as those aimed at child health, not being carried out. All of the participants emphasized the lack of doctors in the ESF, displacing curative care onto nurses, adversely
Table 1. Opportunities and barriers to access related to SUS policies. Recife, Northeastern Brazil, 2007.
Category/participant group Quotes SUS policies incompletely established
(participants from institutions)
- [...] once there are guidelines for children, the program for at-risk children, they must actually make it happen
[...]things are not happening as they were planned to, visits monitoring
this very child[...]. (M8).
- [...] this clinic (referring to the outpatient clinic) should be for support [...] and here the demand has been more direct to the staff rather than
referred by the doctors (referring to ESF doctors) and ACS [...] there has to
be integration [...] I believe it would signifi cantly cut down on child illness
and mortality. (PED4).
Lack of awareness of child health care policies on the part of health care professionals (health care professionals in outpatient clinics/UBT)
- With regards to pediatrics, when there is not a specifi c program[...] I
believe that this still needs to be improved [...]in order for there to be
better health care, be more attentive in these cases of infant mortality[...]
or if this exists, I’m not aware of it, but this is not only my fault as I was
not informed [...]. (UB1).
Fragility of inter-sectoral activities (managers/
ESF/PACS health care professionals) - [...] when discussing avoidable deaths, the fi rst aspect to be considered is the lack of effective inter-sectoral work [...].The health care sector managed to establish partnerships with other sectors, guarantee women’s education, housing, income, generate employment.All of this is
happening, but at a slow pace. (M1).
- [...] the responsibility for infant mortality does not lie so much with
health care [...] it is also a political question, of social exclusion [...] there are other factors involved here, structural, socio-economic, political,
family, health care is limited to treating these problems. (N9).
Poor problem solving on the part of the ESF (mothers)
- I don’t know why they open at all! (referring to the USF) [...]when the
boy gets sick I don’t even bother going there, they don’t resolve anything!
(Mother 15).
- I don’t like going to appointments at the USF very much, because the doctor there often doesn’t know what’s wrong, and refers us to another clinic (referring to outpatient clinics)[...]I prefer to go straight there.
(Mother 1). Establishing ESF/PACS (ESF/PACS health care
professionals) - [...] I don’t think we’re one hundred percent there yet, but we’re getting there [...] infant mortality is falling [...] due to monitoring, the specifi c treatment we provide these children with [...] in the case of vaccination,
diarrhea, these have been controlled. (PACS3).
affecting the ability to solve problems. For health care professionals from the PACS/ESF, the lack of doctors interferes with supervision of the ACSs on their house calls, fundamental to monitoring at risk children. There was confl ict between the mothers’ discourse, which linked infant death to the constant lack of medicines, and those of participants from institutions, who viewed the availability of medication as one of
the positive points of the SUS and did not perceive any connection with the deaths (Table 2).
The great intensity with which organizational barriers emerged, and the refusal to treat serious illness in ESF units, was unanimous among the mothers, who viewed this as one of the causes of infant mortality, obliging them to make use of emergency pediatric services (Table 2).
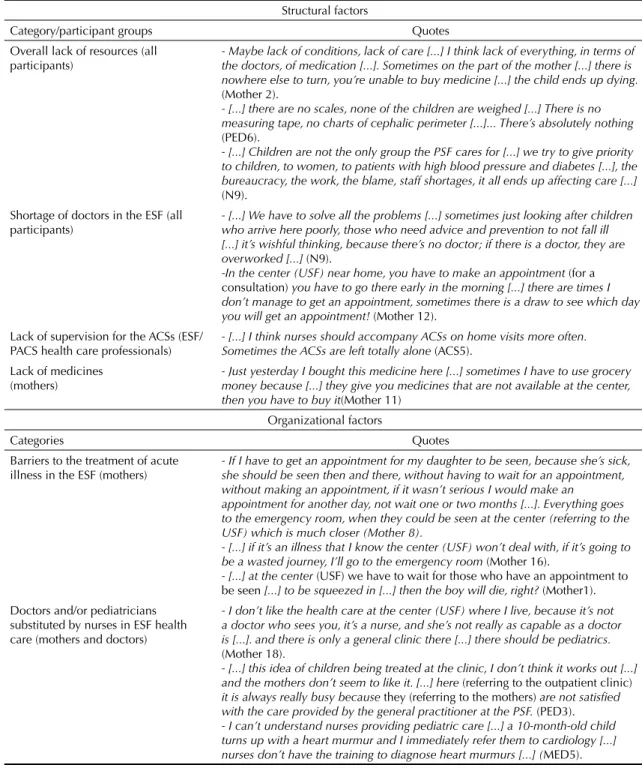
Table 2. Barriers to access related to structural and organizational factors or supply. Recife, Northeastern Brazil, 2007.
Structural factors
Category/participant groups Quotes Overall lack of resources (all
participants) - Maybe lack of conditions, lack of carethe doctors, of medication[...]. Sometimes on the part of the mother[...]I think lack of everything, in terms of [...] there is
nowhere else to turn, you’re unable to buy medicine[...]the child ends up dying.
(Mother 2).
- [...]there are no scales, none of the children are weighed[...] There is no
measuring tape, no charts of cephalic perimeter [...]... There’s absolutely nothing
(PED6).
- [...]Children are not the only group the PSF cares for[...]we try to give priority
to children, to women, to patients with high blood pressure and diabetes[...], the
bureaucracy, the work, the blame, staff shortages, it all ends up affecting care[...]
(N9). Shortage of doctors in the ESF (all
participants) - [...] We have to solve all the problemswho arrive here poorly, those who need advice and prevention to not fall ill[...] sometimes just looking after children [...] it’s wishful thinking, because there’s no doctor; if there is a doctor, they are
overworked[...] (N9).
-In the center (USF) near home, you have to make an appointment (for a
consultation) you have to go there early in the morning[...] there are times I don’t manage to get an appointment, sometimes there is a draw to see which day
you will get an appointment! (Mother 12).
Lack of supervision for the ACSs (ESF/ PACS health care professionals)
- [...] I think nurses should accompany ACSs on home visits more often.
Sometimes the ACSs are left totally alone (ACS5).
Lack of medicines
(mothers) - Just yesterday I bought this medicine heremoney because [...]they give you medicines that are not available at the center, [...] sometimes I have to use grocery
then you have to buy it(Mother 11)
Organizational factors
Categories Quotes
Barriers to the treatment of acute illness in the ESF (mothers)
- If I have to get an appointment for my daughter to be seen, because she’s sick, she should be seen then and there, without having to wait for an appointment, without making an appointment, if it wasn’t serious I would make an
appointment for another day, not wait one or two months [...]. Everything goes to the emergency room, when they could be seen at the center (referring to the USF) which is much closer (Mother 8).
- [...] if it’s an illness that I know the center (USF) won’t deal with, if it’s going to
be a wasted journey, I’ll go to the emergency room (Mother 16).
- [...] at the center (USF) we have to wait for those who have an appointment to
be seen [...] to be squeezed in[...] then theboywill die, right? (Mother1). Doctors and/or pediatricians
substituted by nurses in ESF health care (mothers and doctors)
- I don’t like the health care at the center (USF) where I live, because it’s not a doctor who sees you, it’s a nurse, and she’s not really as capable as a doctor is [...]. and there is only a general clinic there [...] there should be pediatrics.
(Mother 18).
- [...] this idea of children being treated at the clinic, I don’t think it works out [...]
and the mothers don’t seem to like it. [...] here (referring to the outpatient clinic)
it is always really busy because they (referring to the mothers) are not satisfi ed
with the care provided by the general practitioner at the PSF. (PED3).
- I can’t understand nurses providing pediatric care[...] a 10-month-old child
turns up with a heart murmur and I immediately refer them to cardiology[...]
nurses don’t have the training to diagnose heart murmurs [...](MED5).
Barriers to curative health care in the form of the ESF substituting pediatricians with general practitioners and/or nurses were reported by mothers and doctors in outpatient clinics and the ESF as contributing to deaths. In the doctors’ opinions, nurses do not have the proper professional training to provide curative health care, suggesting confl icts within the heath care team (Table 2).
Infant mortality and factors of professional performance
Almost all participants linked inadequate perfor-mance by professionals with low technical quality to preventable infant deaths. Among the interviewees from institutions, this lack of professional commit-ment was attributed to ESF health care teams being overworked, to specialists being poorly trained and to the perception of not being professionally valued. The mothers attributed infant mortality not only to poor
technical quality but to de-humanized, unwelcoming health care at all levels of care (Table 3).
Infant death and the social context
The main determinant of preventable infant morta-lity was the families’ social exclusion, high levels of poverty, unemployment, violence and drug use, accor-ding to almost the participants. The mothers talked of a lack of social support network. For the participants from the ESF/PACS, in concordance with the mothers, infant death was particularly associated with maternal characteristics, blaming the mothers for negligence towards their children (Table 4).
The case of preventable infant death
The case of preventable, post-natal infant death in an area assigned to the ESF permitted a deeper analysis
Table 3. Barriers to access related to factors of professional performance. Recife, Northeastern Brazil, 2007.
Categories/groups of participants Quotes Poor technical- scientifi c quality (all
participants) - [...] I think that these children who are still dying from diarrhea and pneumonia it is because there is no guidance and advice are lacking,
there is no team (referring to the ESF) together[...]more health care.
(N7).
- Give more attention to children [...] because in the majority of centers
(USF) and emergency rooms we go to, they don’t even look at the child [...] they give you any medicine and send you home [...] they should examine the child, see what’s wrong [...] when the child ends up back in the emergency room, they are admitted and may die [...] something that
could be avoided. (Mother 16).
- [...] they (referring to the ESF health care professionals) are simply
doing their job for the money [...] the municipality provides a lot, but
they don’t use that provision to guide families. (Geradm1).
- [...] I remember one child who presented with diarrhea and vomiting [...] the child was looked over quickly in the outpatient clinic and sent home [...] he arrived at another health center and died! What were our
failures that lead to this child dying thatvery day? (UB1).
Lack of professional commitment in ESF activities (participants from institutions)
- I suffer a lot[...]I don´t treat the children because the other categories
of the PSF keep me too busy and pediatrics ended up with no medical
care. (MED9).
- [...] I suffer over this because you can’t do what you would like to [...] I
already started a group (education and health) and I couldn’t go ahead
with it, we didn’t have the energy for it [...] due to being overworked
(N1).
- Our universities don’t train people to work from the perspective of promoting, preventing, comprehensive treatment, clinical responsibility.
(M1).
- [...] in the university they teach you that bad doctors work at the PSF, students who end up in the PSF are weak [...]because the good students
are going to be specialists.(M4).
Dehumanized unwelcoming health care (mothers)
- [...]being patient with the children, being conscientious and treating
people with courtesy because there are a lot who[...] have already
argued with the doctor here for being rude, if we ask what is wrong with the child, if it’s something serious he answers “ Who is the doctor here:
me or you?”. But I’m the mother[...]they should explain properly so that
I know what’s happening (Mother 4).
- [...] there are doctors who are not caring, who don’t even touch the
child as if it made them nauseous! (Mother 5).
of the actual obstacles to health care services and campaigns which had emerged from the interviews, and showed links between the main barriers to access to children’s health care throughout the course of their day to day access (or lack of it) to health care. Situations which emerged in the process of interaction between the various participants involved with the child from in-utero to its death were analyzed: a) barriers to access such as the mother not having ante-natal checks, social risk and ESF doctors and nurses not monitoring at risk children. This suggests that SUS child health care policies are not completely established and a lack of professional commitment on the part of the ESF; b) the sick child not receiving care the day before their death, which demonstrates the barrier to treatment of acute illness in USF; and c) the lack of references to timely medical assistance when the USF refused treat-ment. Poor technical and scientifi c quality and a lack of professional commitment on the part of the ESF were reported. The events contributed to preventable infant death which could have been avoided by actions and health care services (Table 5).
DISCUSSION
In spite of the Brazilian government’s directors’ commitment to comprehensive child health care and a signifi cant decline in infant mortality,25,a numerous
barriers to access indicate the fragility with which the SUS has been established and of the main access point: basic health care. Ultimately, this has repercus-sions on the perpetuation of preventable infant deaths. There were signifi cant differences in the perception and/or intensity of the statements, probably due to the participant’s position with regards to the phenomenon.
Lack of awareness of policies aimed at children’s health and of the health care model25,a on the part of health
care professionals, together with professionals from both levels of health care’s views that care is supplied better in the traditional model and the mothers’ percep-tions of poor problems solving capabilities in the ESF, are examples of the model’s poor consolidation. This is worrying, especially in relation to the main point of access, where the majority of activities to avoid
Table 4. Barriers to access related to factors of family context. Recife, Northeastern Brazil, 2007.
Categories/groups of participants Barriers
Poverty (all participants) - [...] I think it’s down to people’s miserable living conditions, because the majority of these deaths are from the poor social classes [...] employment is more and more diffi cult, [...] there’s not enough food, a decent living place, they live there in that swamp with all kinds of illnesses. (UB2).
Blaming the mothers, poverty, violence and lack
of social support networks (mothers) - Mothers who don’t take care [...] they make a career out of having children [...] they have a fi ve-year-old child looking after a one-year-old one [...] and there they are, playing in the rubbish, pick up
bacteria, get sick and end up dying. (Mother 16).
- [...] where I live, it’s like that, the people are settled, they’re used to the violence, children begging [...] if someone needs help, no one wants to give it [...] and sometimes, when someone seeks health care, there is not help [...]. Those are not the kind of people you can go up to and ask “Can you lend me some money to take my child to
hospital?”. Nobody helps! (Mother 13).
Blaming the mothers for negligence and drug use (ESF/PACS health care professionals and mothers)
- Unplanned pregnancies, alcoholism and drug abuse [...] they leave the children at home alone and go to the bar [...] those children die
because of neglect. (MED5).
Blaming mothers for negligence and not realizing
the seriousness of the illness (mothers) - Lack of health care is it? I don’t know [...] the mother, in my opinion, if the child has a fever you go straight to hospital, because it’s ill [...] me, when mine was ill, I go straight there, and there are lots of mothers who keep the child at home “it’s a daft little fever” and when they fi nally see that it’s something serious it’s too late and there is not
time for it to be treated and the child dies. (Mother 8).
Blaming mothers for negligence and poor quality
care (mothers) - Poor treatment is it? It’s also an emergency case [...] if the mother doesn’t also care for the child, doesn’t head straight to the doctor [...]. In an emergency like that, you still have to wait your turn [...] the child had a high fever [...] and you have to wait, right? There are a lot of
tired children there [...] lots of hospitalized children [...] (Mother 10).
- When a mother delays taking the child to the doctor, trying to treat the child at home, when they fi nally get to the hospital it’s too late
[...].The health care provided in the hospital is often poor[...] I think
it’s because of this. (Mother 12).
preventable infant death through actions and health care services take place. Infant death in areas assigned to the ESF as a result of failures in the Government Program to Reduce Infant Mortalityf highlights
barriers to implementing child health care policies. The confl icts between the current model and the traditional,
well-structured network, in which primary health care was provided by pediatricians, demonstrate the need for fresh adjustments to enable the new model to be understood and legitimized.5,22
The main criticisms of the new model which emerged from the mothers’ statements were the lack of doctors
Table 5. The course of preventable infant mortality: the diverse barriers to access. Recife, Northeastern Brazil, 2007.
Barriers in the ESF Primary Care Example Quotes Ante natal
- Lack of home visits to at-risk pregnant women by the whole ESF team to provide guidance
-[...]she did not carry out the ante natal checks during
pregnancy, nor was the child’s well being monitored. She
only cam when the child was sick (Nurse).
Post natal
- Lack of preventative actions
- RN not included in monitoring activities for at-risk children according to social criteria: unemployed mother, drug use, multiple partners, single mother, areas of social risk.
- No home visit by nurse and/or doctor.
- Child only has USF appointments when ill; lack of guidance on promoting health and avoiding infant death
-[...] she (ACS) came to the house on the day we went there
(the maternity hospital) [...] later I went to the center (USF)
and I told here (ACS) “the girl doesn’t have a crib and she’s
sleeping with me in the bed with me and the other four children, fi ve altogether counting her[...].” (Mother).
[...] I always turned up at the center without making an
appointment, I arrived at the last minute with the girl[...].
(Mother).
No responsibility taken for the child throughout the course of their health care
- Team does not continue to provide care after referral and return to specialist services.
[...] so she(ACS) comes to the house to go through her
routine; and I said “the girl is distressed and vomiting” and she said “take her to the center”. I took her to the center. The doctor saw us and sent us to the hospital, gave me a
bus ticket. (Mother).
The doctor there (the children’s hospital) sent us home
again [...] he suspected she had a stomach infection, and prescribed an antibiotic, but I didn’t want to give it to her
because it was very strong[...] she was very young[...]I
gave her saline, I asked for it at the center[...]. (Mother). Failures in access to health care during illness which
contributed to the death
- Failure to comply with policies: at risk children not receiving medical/nurse appointments for more than a month before death.
- Refusal by the USF to treat a child with acute respiratory disease the day before death occurred.
No guidance given as to other services where treatment would be provided.
- [...] then I had a problem, phlebitis, and I was off for ten
days. (Doctor).
- [...]So I tried to get in touch with the ACS and they told me
“she’s not here, she’s out”, so I asked “where is the doctor?” “The doctor has left”. I took her back home, gave her Dipirona, the fever passed, I fed her, winded her, put her to sleep, she was playing, she wasn’t poorly, she was alert, and
so we went to sleep. (Mother).
- Death due to aspirating milk triggered by respiratory disease (and/or aggravated by smoke in the household / compression by the body of another child).
- [...]so I said: “hey! She’s asleep, I’m going to get her and
feed her, my breasts were really full”[...]I went up and lit
a cigarette. Smoked it and turned around and she was still asleep[...] and I said to myself:” she’s sleeping a lot”[...] and when I went to pick her up her clothes were all wet with milk, her nose was blocked with catarrh and she was
purple[...] so I picked her up and went running into the
street (Mother). - Blame placed on the mother and on overwork caused by
the death of the child. Intra-team confl icts.
- [...] as she(the mother) is a drug user, she fell asleep on
top of the child, suffocating her, or she did not pay attention when she was feeding her, the child regurgitated the
milk and ended up aspirating it[...]. It was an unplanned
pregnancy[...] she didn’t use contraceptives, the doctor
didn’t give her a prescription, and I don’t give medicine if
the doctor hasn’t already prescribed it. (Nurse).
[...]I believe the following: that families who need more
health care should be monitored[...] more closely. [...]the
vehicle for the doctor, the nurse, are the ACSs, no? we say: “look at him, or look at her, these people need to be looked
after”[...]but we are here with a lot of other people to look
in the ESF, limited curative health care, doctors being substituted for nurses and the refusal to treat acute illness. They made it diffi cult to monitor at-risk chil-dren, the priority of the whole health care team.18,22,f The
lack of doctors interfered in work processes and in inter--personal relationships as nurses were overworked and their roles in the ESF not clearly defi ned. This increased confl icts in the teams’ work, permeating into values, attitudes and historically determined conceptions.3,17,18,21
The infant death case study revealed the ESF’s failure to monitor at risk children as one of the main deter-minants of infant death as well as indicating the link between other lapses in the health care provided, such as diffi culties in working in teams. The fact that respon-sibility for the death was avoided and blame placed on the mother refl ects serious problems in communication and professional conduct as well as probable corpo-rate issues.3,6 On the one hand, there is resistance to
hierarchical change among medical professionals in the former care model and, on the other, promotion of nurses to a level equal to that of the doctors, which generates intra-team confl icts.3,17
Barriers related to poor performance indicate the lack of quality health care in the ESF and no responsibi-lity being taken for the child throughout the course of their health care. Failing to comply with govern-ment child health care directives highlight failures in the way comprehensive child health care policies are established.f These were aspects present in the
statements of all participants and in the infant death case study.
The mothers’ unanimous vision of the health care process as dehumanized suggests that access to health care through the means of welcoming, sympathetic interpersonal relationships between patient and health care provider8,15 is not common practice, making this
a SUS operational directive which has not become incorporated in the minds of health care professionals dealing with children’s health care.7,21
Blaming the child’s death on the mother’s negli-gence was something which emerged mainly among the mothers and female ESF/PACS health care
professionals. These health care professionals empha-sized maternal factors, separating them from the context of social misery and played down inadequate access to health care. These statements implied prejudiced, probably ideological attitudes. Among the mothers, contradiction appeared in the statements, which had a note of involuntary maternal involvement, intertwined with conditions of extreme vulnerability. These data are consistent with those from the Scheper-Hughes20 study,
developed in Northeastern Brazil, but not with those of the study carried out by Nations,16 in the same area at
the same time, in which the mothers perceived failures in health care as one of the determinants of death. The results show an attitude more of resignation on the part of the mothers, towards the miserable conditions of the context which overcame the perception of obstacles to health care access.9,12,13,20,22,24 They also refl ect a position
of little solidarity, based on the impersonality of the guiding question, which referred to the deaths of the children of mothers they did not know, which contri-buted to the development of blame in their statements.
To conclude, the existence of numerous barriers to access to child health care refl ects the way the SUS, and its main access point, the ESF, have not been fi rmly established. The participants fail to perceive the link between poor quality health care services and the conti-nuing occurrence of preventable infant mortality which could be avoided by actions and health care services through child health care policies.
The structural (lack of medicines in the ESF), organi-zational (restrictions on care for acute illnesses/doctors substituted for nurses) and professional performance (poor technical quality, care that is not welcoming/ dehumanized and problems with team work) barriers prove themselves to be the main obstacles to access to primary care which takes responsibility for the child throughout the whole course of their health care.
Despite the mothers’ conditions of social exclusion being linked to infant mortality, these factors can be minimized with effi cient primary care, bearing in mind the important role played by fairer and effective social policies.
f Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Ações Programáticas Estratégicas. Agenda de compromissos para a
1. Acurcio FA, Guimarães MDC. Acessibilidade de indivíduos infectados pelo HIV aos serviços de saúde: uma revisão de literatura.
Cad Saude Publica. 1996;12(2):233-42.
DOI:10.1590/S0102-311X1996000200012
2. Aday LA, Andersen R. A framework for the study of access to medical care. Health Serv Res. 1974;9(3):202-20.
3. Araújo MFS. O enfermeiro no Programa de Saúde da Família: prática profi ssional e construção da identidade. Rev Conceitos. 2005;8(12):39-43.
4. Bardin L. Análise de conteúdo. Lisboa: Edições 70; 1979.
5. Conill EM. Ensaio histórico-conceitual sobre a Atenção Primária à Saúde: desafi os para a organização de serviços básicos e da Estratégia Saúde da Família em centros urbanos no Brasil.
Cad Saude Publica. 2008;24(Supl 1):S7-16.
DOI:10.1590/S0102-311X2008001300002
6. Delgado ME, Vargas I, Vázquez ML. El rigor en la investigación cualitativa. In: Vázquez Navarrete ML, Silva MRF, Mogollón Pérez AS, Fernández de Sanmamed MJ, Delgado Gallego ME, Vargas Lorenzo I, editores. Introducción a las técnicas cualitativas de investigación aplicadas en salud.Barcelona: Servei de Publicacions-Universitat Autònoma de Barcelona; 2006. p.83-96.
7. Deslandes SF. Análise do discurso ofi cial sobre a humanização da assistência hospitalar.
Cienc Saude Coletiva. 2004;9(1):7-14.
DOI:10.1590/S1413-81232004000100002
8. Franco TB, Bueno WS, Merhy EE. O acolhimento e os processos de trabalho em saúde: o caso de Betim, Minas Gerais, Brasil.
Cad Saude Publica. 1999;15(2):345-53.
DOI:10.1590/S0102-311X1999000200019
9. Frias PG, Lira PIC, Vidal SA, Vanderlei LC. Vigilância de óbitos infantis como indicador da efetividade do sistema de saúde: estudo em um município do interior do Nordeste brasileiro. J Pediatr (Rio J). 2002;78(6):509-16. DOI:10.1590/S0021-75572002000600012
10. Goulart LMHF, Somarriba MG, Xavier CC. A perspectiva das mães sobre o óbito infantil: uma investigação além dos números.
Cad Saude Publica. 2005;21(3):715-23.
DOI:10.1590/S0102-311X2005000300005
11. Guba EG, Lincoln YS. Effective evaluation: improving the usefulness of evaluation results through responsive and naturalistic approaches. San Francisco: Jossey-Bass; 1992. (Jossey Bass Social and Behavioral Sciences Series).
12. Jobim R, Aerts D. Mortalidade infantil evitável e fatores associados em Porto Alegre, Rio Grande
do Sul, Brasil, 2000-2003. Cad Saude Publica. 2008;24(1):179-87. DOI:10.1590/S0102-311X2008000100018
13. Malta DC, Duarte EC, Escalante JJC, Almeida MF, Sardinha LMV, Macário EM, et al. Mortes evitáveis em menores de um ano, Brasil, 1997 a 2006: contribuições para a avaliação de desempenho do Sistema Único de Saúde.
Cad Saude Publica. 2010;26(3):481-91.
DOI:10.1590/S0102-311X2010000300006
14. Minayo MCS. O desafi o do conhecimento: pesquisa qualitativa em saúde. 8.ed. São Paulo: Hucitec; 2004.
15. Nations MK, Gomes AMA. Cuidado, “cavalo batizado” e crítica da conduta profi ssional pelo paciente-cidadão hospitalizado no Nordeste brasileiro. Cad Saude Publica. 2007;23(9):2103-12. DOI:10.1590/S0102-311X2007000900018
16. Nations MK. Infant death and interpretive violence in Northeast Brazil: taking bereaved Cearense mothers’ narratives to heart.
Cad Saude Publica. 2008;24(10):239-48.
DOI:10.1590/S0102-311X2008001000005
17. Pedrosa JIS, Teles JBM. Consenso e diferenças em equipes do Programa Saúde da Família.
Rev Saude Publica. 2001;35(3):303-11.
DOI:10.1590/S0034-89102001000300014
18. Roncalli AG, Lima KC. Impacto do Programa Saúde da Família sobre indicadores de saúde da criança em municípios de grande porte da região Nordeste do Brasil. Cienc Saude Coletiva. 2006;11(3):713-24. DOI:10.1590/S0034-89102001000300014
19. Rutstein DD, Berenberg W, Chalmers TC, Child CG 3rd, Fishman AP, Perrin EB. Measuring the quality of medical care: a clinical method. N Engl J Med. 1976;294(11):582-8. DOI:10.1056/NEJM197603112941104
20. Scheper-Hughes N. Culture, scarcity and maternal thinking: maternal detachment and infant survival in a Brazilian shantytown. Ethos. 1985;13(4):291-317.
21. Schimith MD, Lima MADS. Acolhimento e vínculo em uma equipe do Programa Saúde da Família. Cad Saude Publica. 2004;20(6):487-94. DOI:10.1590/S0102-311X2004000600005
22. Souza ECF, Vilar RLA, Rocha NSPD, Uchoa AC, Rocha PM. Acesso e acolhimento na atenção básica: uma análise da percepção dos usuários e profi ssionais de saúde. Cad Saude Publica. 2008;24(Supl 1):S100-10. DOI:1):S100-10.1590/S0102-311X2008001300015
23. Tottrup C, Tersbol BP, Lindeboom W, Meyrowitsch D. Putting child mortality on a map: towards an understanding of inequity in health. Trop Med Int Health. 2009;14(6):653-62. DOI:10.1111/j.1365-3156.2009.02275.x
The authors declare that there are no confl icts of interests.
HIGHLIGHTS
The article analyzes barriers to primary health care as one of the factors associated with preventable infant mortality in Recife, PE.
The authors estimate that 86% of infant deaths could be avoided through timely, effective actions on the part of the health care services.
Managers and directors of health care units and districts, health care professionals, community health workers and mothers were interviewed. The authors selected 18 sentinel events for the study of health care access barriers
The barriers identifi ed by the interviewees were: the health care model being inadequately established, the fragility of inter-sectoral links, poor ability, on the part of the Family Health Service teams, to solve problems, scarcity of material and human resources, lack of medication, pediatricians substituted by clinicians not trained to care for children and inadequate professional performance.
The study showed concrete diffi culties related to the implementation of the child health program, limitations of the care model and scarce health resources.
Profa. Rita de Cássia Barradas Barata Scientifi c Editor 24. Vargas I, Vázquez ML, Mogollón-Pérez AS, Unger JP.
Barriers of access to care in a managed competition model: lessons from Colombia. BMC Health Serv Res. 2010;10:297. DOI:10.1186/1472-6963-10-297