w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Liver
and
spleen
biometrics
in
childhood-onset
systemic
lupus
erythematosus
patients
Andressa
Guariento
a,b,
Marco
Felipe
C.
Silva
a,
Priscilla
S.F.
Tassetano
a,
Sílvia
Maria
S.
Rocha
c,
Lúcia
M.A.
Campos
a,
Marcelo
Valente
c,
Clovis
A.
Silva
a,d,∗aPediatricRheumatologyUnit,FaculdadedeMedicina,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil bPediatricRheumatologyUnit,SantaCasadeMisericórdiadeSãoPaulo,SãoPaulo,SP,Brazil
cPediatricRadiologyUnit,FaculdadedeMedicina,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil dDepartmentofRheumatology,FaculdadedeMedicina,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received31July2014 Accepted24December2014 Availableonline16March2015
Keywords: Hepatomegaly Spleenatrophy Ultrasound Biometry
Systemiclupuserythematosus Pediatricrheumatology
a
b
s
t
r
a
c
t
Objective:Toevaluateliverandspleendimensionsinchildhood-onsetsystemiclupus ery-thematosus(c-SLE)patientsandhealthycontrols.
Methods:30c-SLEpatientsand30healthycontrolvolunteersunderwentabdominal ultra-sound. The following two liver measurements were performed in left hepatic lobe: craniocaudalandanteroposterior andthreein righthepaticlobe (RHL):posterior cran-iocaudal(PCC-RHL),anterior craniocaudalandanteroposterior.Threespleendimension measurementswerealsoevaluated:longitudinal,transverseandanteroposterior. Demo-graphic, clinical and laboratorial data, SLEDAI-2K, ECLAM, SLAM and treatment were assessed.
Results:Meancurrentagewassimilarinc-SLEandcontrols(170.31±27.81vs.164.15±39.25 months;p=0.486).ThemeanofPCC-RHLdimensionwassignificantlyhigherinc-SLE com-paredtocontrols(13.30±1.85vs.12.52±0.93,p=0.044).Therewerenodifferencesbetween theother hepaticbiometricsandsplenicparameters(p>0.05).Furtheranalysisinc-SLE patientsaccordingtoPCC-RHLdimension≥13.3cmversus<13.3cmshowedthatthemedian ofSLEDAI-2K[8(0–18)vs.2(0–8),p=0.004],ECLAM[4(0–9)vs.2(0–5),p=0.019]andSLAM [5(1–13)vs.2(0–14),p=0.016]weresignificantlyhigherinpatientswithhigherPCC-RHL dimension,likewisethefrequencieofnephritis(77%vs.29%,p=0.010).Liverenzymeswere similarinbothgroups(p>0.05).PositivecorrelationwasobservedbetweenSLEDAI-2Kand PCC-RHL(p=0.001,r=+0.595).Negativecorrelationwasevidencedbetweendiseaseduration andlongitudinaldimensionofspleen(p=0.031,r=−0.394).
Conclusion:Ourdataraisesthepossibilitythatdiseaseactivitycouldleadtoasubclinical andlocalizedhepatomegalyduringthediseasecourse.Longdiseasedurationresultedto spleenatrophyinc-SLEpatients.
©2015ElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](C.A.Silva).
http://dx.doi.org/10.1016/j.rbre.2014.12.009
Biometria
do
fígado
e
do
bac¸o
em
pacientes
com
lúpus
eritematoso
sistêmico
de
início
na
infância
Palavras-chave: Hepatomegalia Atrofiadobac¸o Ultrassonografia Biometria
Lúpuseritematososistêmico Reumatologiapediátrica
r
e
s
u
m
o
Objetivo: Avaliarasdimensõesdofígadoedobac¸oempacientescomlúpuseritematoso sistêmicodeiníciopediátrico(LESp)econtrolessaudáveis.
Métodos: 30pacientescomLES-ie30voluntáriossaudáveiscontroleforamsubmetidos a umaultrassonografiadoabdome. Foramrealizadasduas medic¸õesdofígadonolobo hepáticoesquerdo(craniocaudaleanteroposterior)etrêsnolobohepáticodireito(LHD) (craniocaudalposterior[CCP-LHD],craniocaudalanterioreanteroposterior).Foramtambém avaliadastrêsmedidasdasdimensõesdobac¸o:longitudinal,transversaleanteroposterior. Foramavaliadosdadosdemográficos,clínicoselaboratoriais,SLEDAI-2K,ECLAM,SLAMe tratamento.
Resultados:AidademédiafoisemelhantenospacientescomLES-iecontroles(170,31±27,81 vs.164,15±39,25meses;p=0,486).AmédiadadimensãoCCP-LHDfoisignificativamente maiornogrupoLES-iemcomparac¸ãoaoscontroles(13,30±1,85vs.12,52±0,93,p=0,044). Nãohouvediferenc¸asnosoutrosparâmetrosbiométricosdofígadoedobac¸o(p>0,05).Uma análiseespecificarealizadaapenasnospacientescomLESpdeacordocomadimensão CCP-LHD≥13,3cmversus<13,3cmmostrouqueamedianadoSLEDAI-2K[8(0–18)vs.2 (0–8),p=0,004],ECLAM[4(0–9)vs.2(0–5),p=0,019]eSLAM[5(1–13)vs.2(0–14),p=0,016]era significativamentemaiorempacientescommaiordimensãoCCP-LHD,domesmomodoque afrequênciadenefrite(77%vs.29%,p=0,010).Asenzimashepáticasforamsemelhantesnos doisgrupos(p>0,05).Foiobservadaumacorrelac¸ãopositivaentreoSLEDAI-2Keadimensão CCP-LHD(p=0,001,r=+0,595).Evidenciou-seumacorrelac¸ãonegativaentreadurac¸ãoda doenc¸aeadimensãolongitudinaldobac¸o(p=0,031,r=−0,394).
Conclusão: Osdadoslevantamapossibilidadedequeaatividadedadoenc¸apodelevara umahepatomegaliasubclínicaelocalizadaduranteocursodadoenc¸a.Adurac¸ãodadoenc¸a resultouematrofiadobac¸oempacientescomLES-i.
©2015ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Hepatomegaly and/or splenomegaly occur in 20–50%
childhood-onset systemic lupus erythematosus1 (c-SLE)
patients at disease onset, usually associated with disease activity.Involvementofthe reticuloendothelialsystemmay alsobeassociatedwithabnormalliverfunctiontests.2,3
Abdominalultrasound can beused to assess liver4 and
spleen measurements in children and adolescents
with-out risk of radiation.5 However, a systematic evaluation
of these visceral organ dimensions has not been
per-formedinc-SLEpopulation, particularlyduringthedisease course.
Therefore,theobjectivesofourstudyweretoevaluateliver andspleendimensionsinc-SLEpatientsandhealthycontrols andtoassesspossibleassociationsbetweenabnormalitiesin liverandspleensizeswithdemographicdata,clinicalfeatures, diseaseactivity,cumulativedamageandtreatment.
Materials
and
methods
Patientsandcontrols
FromMaytoJune2012,58c-SLEpatientswerefollowedatour PediatricRheumatologyService. All ofthe patientsfulfilled
theAmericanCollegeofRheumatologycriteriaforc-SLE.6The exclusion criteria were currentacute or chronicinfections, autoimmunehepatitis,otherconcomitantdiseasewith hep-atosplenomegaly, canceror unwillingtoparticipate.Out of them,15wereexcludedduetocurrentacuteinfections,9due tounwillingnesstoparticipateand4duetoautoimmune hep-atitis.Therefore,thecross-sectionalstudywasconductedin 30c-SLEpatients.Thecontrolgroupincluded30healthy con-trolvolunteersrecruitedfromtheprimarycareclinicnearby our tertiary hospital. The control volunteers were submit-ted toclinical evaluation, and liver and spleenbiometrics. Localethics committeeofouruniversity hospitalapproved thisstudy,andinformedconsentwasobtainedfromall par-ticipants.
Liverandspleenbiometrics
Abdominal ultrasound was carried out by an experienced
and trained, specialist(SMS) using a1–6mHz convex mul-tifrequency transducer(LOGIC E9® – GeneralElectric, USA).
The following two liver measurements were performed in
measurementswerealsoevaluated:longitudinal,transverse andanteroposterior.
Demographicdata,clinical,laboratorialandtreatment assessment
Demographic data included current age, disease duration
and gender. Weight and heightwere evaluated. Body mass
index (BMI) was defined by weight in kilograms/height in
meters2(kg/m2).Bodysurfacearea(BSAinm2)wascalculated
accordingtotheformula:(weightinkilograms0.425×heightin
centimeters0.725)×0.007184.
SLEclinicalmanifestationsweredefinedas:hepatomegaly (liveredge>2cmbelowtherightcostalmargin),splenomegaly
(palpable spleen below the left costal margin),
mucocu-taneous lesions (malar or discoid rash, oral ulcers or
photosensitivity),articular involvement(non-erosive arthri-tis), neuropsychiatric disease (seizure or psychosis), renal involvement (proteinuria≥0.5g/24h, presence of cellular casts,and/orpersistenthematuria≥10redbloodcellsperhigh power field), serositis(pleuritis or pericarditis), and hema-tologicabnormalities(hemolyticanemia,leukopeniawitha whitebloodcellcount<4000mm–3,lymphopenia<1500mm–3
on two or more occasions and thrombocytopenia with
platelet count<100,000mm–3 in the absence of drugs or
infection).
Diseaseactivity wasevaluated accordingto SLEDisease ActivityIndex2000(SLEDAI-2K),7EuropeanConsensusLupus ActivityMeasurement(ECLAM),8andSystemicLupus
Activ-ity Measure (SLAM) scores.9 Cumulative damageusing the
SLE International Collaborating Clinics/ACR Damage Index
(SLICC/ACR-DI).10
Erythrocyte sedimentation rate (ESR) was performed
by Westergreen method and C-reactive protein (CRP) by
nephelometry.Anti-double-strandedDNA(anti-dsDNA)was
detectedbyindirectimmunofluorescenceusingCrithidia lucil-iaeassubstrate.Presenceofanticardiolipinantibodies(aCL)
IgG and IgM was analyzed by enzyme-linked
immunosor-bentassay(ELISA). Lupusanticoagulant(LAC)wasdetected accordingto the guidelines ofthe InternationalSociety on ThrombosisandHemostasis.11
Data concerning the cumulative and current dosage of
prednisone,hydroxychloroquine,methotrexate,azathioprine,
intravenouscyclophosphamide,cyclosporineand
mycophe-nolatemofetilweredetermined.
Statisticalanalysis
Resultswerepresentedasthemean±standarddeviation(SD) ormedian(range)forcontinuousandnumber (%)for cate-goricalvariables.DatawerecomparedbyMann–Whitneytest incontinuousvariablestoevaluatedifferencesamongc-SLE andcontrolgroup,andamongSLEsubgroups.For categori-calvariables,differenceswereassessedbyFisher’sexacttest. Spearmanrankcorrelationcoefficientwasusedfor correla-tions between disease activity scores and liver and spleen parameters.Thelevelofsignificanceofindependentvariable wassetat5%(p<0.05).
Results
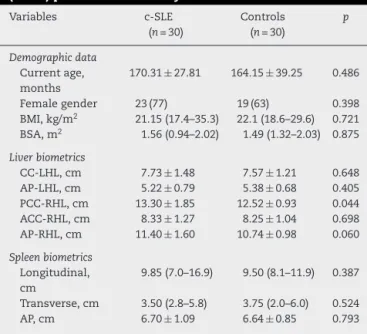
Table1includesdemographicdata,liverandspleen biomet-ricsinc-SLEpatientsandhealthycontrols.Themeancurrent agewassimilarbetweenthec-SLEandcontrols(170.31±27.81 vs. 164.15±39.25months; p=0.486),likewisethe frequency
of female gender (77% vs. 63%, p=0.398) and median of
BSA (p=0.875). The mean ofPCC-RHL dimension was
sig-nificantly higherinc-SLEcomparedtocontrols(13.30±1.85 vs.12.52±0.93,p=0.044)(Table1).Therewerenodifferences betweentheotherhepaticbiometricsandsplenicparameters (p>0.05). Noneofc-SLEandhealthy controlshadjaundice, ascites,pruritus,bleeding,liverorspleenthrombosisor sono-graphichepaticsteatosis.
Further analysis in c-SLE patients according to
PCC-RHL dimension ≥13.3cm (Table 2) (mean ofthis biometric measurementin30c-SLEpatients)versus<13.3cmshowed thatthemedianofSLEDAI-2K[8(0–18)vs.2(0–8),p=0.004], ECLAM [4 (0–9) vs. 2 (0–5), p=0.019] and SLAM [5 (1–13) vs. 2 (0–14),p=0.016] were significantly higher in patients
withhigher PCC-RHLdimension,likewisethe meanofESR
(33.7±16 vs. 22.0±13mm/h, p=0.038). The frequencies of nephritisweresignificantlyhigherinpatientswithPCC-RHL dimension≥13.3cmversus<13.3cm(77%vs.29%,p=0.010). ThemeanofBSAwasalsosignificantlyhigherintheformer group(1.56±0.23vs.1.37±0.26m2,p=0.043).Themedianof
serumliverenzymesweresimilarinbothgroups(p>0.05). Onlyonec-SLEpatienthadhepatosplenomegaly(liveredge
4cm below the right costal margin and spleen edge 4cm
Table1–Demographicdata,liverandspleenbiometrics inchildhood-onsetsystemiclupuserythematosus (c-SLE)patientsandhealthycontrols.
Variables c-SLE (n=30)
Controls (n=30)
p
Demographicdata
Currentage, months
170.31±27.81 164.15±39.25 0.486
Femalegender 23(77) 19(63) 0.398 BMI,kg/m2 21.15(17.4–35.3) 22.1(18.6–29.6) 0.721
BSA,m2 1.56(0.94–2.02) 1.49(1.32–2.03) 0.875
Liverbiometrics
CC-LHL,cm 7.73±1.48 7.57±1.21 0.648 AP-LHL,cm 5.22±0.79 5.38±0.68 0.405 PCC-RHL,cm 13.30±1.85 12.52±0.93 0.044 ACC-RHL,cm 8.33±1.27 8.25±1.04 0.698 AP-RHL,cm 11.40±1.60 10.74±0.98 0.060
Spleenbiometrics
Longitudinal, cm
9.85(7.0–16.9) 9.50(8.1–11.9) 0.387
Transverse,cm 3.50(2.8–5.8) 3.75(2.0–6.0) 0.524 AP,cm 6.70±1.09 6.64±0.85 0.793
Resultsarepresentedinmedian(range)ormean±standard devia-tionandn(%).
Table2–Demographicdata,diseaseparameters,clinicalandlaboratorialfeaturesandtreatmentinchildhood-onset systemiclupuserythematosus(cSLE)patientsaccordingtoposteriorcraniocaudalofrighthepaticlobe(PCC-RHL) dimension.
PCC-RHL≥13.3cm (n=13)
PCC-RHL<13.3cm (n=17)
p
Demographicdata
Currentage,month 173.49±23.05 167.87±31.45 0.592
Diseaseduration,month 36.0(7.2–104.4) 40.8(4.8–156.0) 0.869
BMI,kg/m2 21.1(17.4–35.3) 21.4(16.9–32.9) 0.483
BSA,m2 1.56±0.23 1.37±0.26 0.043
Femalegender 11(85) 12(71) 0.326
Diseaseparameters
SLEDAI-2K 8(0–18) 2(0–8) 0.004
ECLAM 4(0–9) 2(0–5) 0.019
SLAM 5(1–13) 2(0–14) 0.016
SLICC-ACR-DI 0(0–1) 0(0–1) 0.242
Clinicalandlaboratorialfeatures
Hepatosplenomegaly 0(0) 1(6) 1.0
Articular 2(15) 3(18) 0.633
Mucocutaneous 6(46) 6(35) 0.547
Hematological 5(38) 4(23) 0.314
Serositis 1(8) 1(6) 0.687
Neuropsychiatric 2(15) 0(0) 0.179
Nephritis 10(77) 5(29) 0.010
ESR,mm/h 33.7±16 22.0±13 0.038
CRP,mg/dL 7.4(0.1–20.8) 0.8(0.1–12.9) 0.094
AST,IU/L 20(11–55) 21(11–63) 0.322
ALT,IU/L 31(11–47) 33(7–61) 0.622
Anti-dsDNA 3(23) 0(0) 0.070
IgMACL 3(23) 1(6) 0.204
IgGACL 3(23) 2(12) 0.367
LAC 0(0) 2(12) 0.313
Treatment
Currentprednisone 12(92) 12(71) 0.156
Dose,mg/day 20(10–50) 15(3–30) 0.089
Cumulativedose,g 24.85(7.1–54.5) 19.72(6.1–451.3) 0.477
Currentazathioprine 4(31) 7(41) 0.421
Currentmycophenolatemofetil 7(54) 4(23) 0.093
Currentmethotrexate 2(15) 2(12) 0.591
Currenthydroxychloroquine 11(85) 17(100) 0.179
Resultsarepresentedinmedian(range)ormean±standarddeviationandn(%).
BMI,bodymassindex;BSA,bodysurfacearea;SLEDAI-2K,SystemicLupusErythematosusDiseaseActivityIndex2000;ECLAM,European ConsensusLupusActivityMeasurement;SLAM,SystemicLupusActivityMeasure;SLICC/ACR-DI,SystemicLupusInternational Collaborat-ingClinics/ACRDamageIndex;AST,alanineaminotransferase;ALT,aspartateaminotransferase;ACL,anticardiolipinantibody;LAC,lupus anticoagulant.
below the left costal margin), however the PCC-RHL was <13.3cm.
CorrelationswereevidencedbetweenSLEDAI-2Kand PCC-RHL (p=0.001, r=+0.595), SLEDAI-2K and CC-LHL (p=0.015, r=+0.440),SLEDAI-2KandACC-RHL(p=0.017,r=+0.431),and SLEDAI-2Kand AP-RHL dimensions(p=0.029, r=+0.399), as wellasobservedbetweenSLEDAI-2Kandlongitudinalspleen dimension(p=0.042,r=+0.373).Also,itwasfoundapositive correlationbetweenSLAMandPCC-RHL(p=0.020,r=+0.422), SLAMandCC-LHL(p=0.047,r=+0.365),ECLAMandPCC-RHL (p=0.018,r=+0.430),ECLAMandCC-LHL(p=0.008,r=+0.475), as well as found between ECLAMand longitudinal spleen dimension(p=0.047,r=+0.365).
Negative correlation was evidenced between disease duration and longitudinal dimension of spleen (p=0.031, r=−0.394).
Discussion
Toour knowledge,this wasthe first studythat specifically addressedliverandspleenbiometricsinpediatriclupus popu-lation,andshowedsubclinicalhepatomegalyinpatientswith diseaseactivityassociatedwithBSA.Moreover,longperiodof diseaseduration mayberelatedtosplenicatrophyinc-SLE patient.
concomitantchronicdiseaseswithhepatosplenomegalyare importantsincetheseabnormalitiesmayalsoinfluencethe dimensions.However,themainlimitationsofthisstudywere thesmallnumber ofpatients, thelackoflaboratoryexams evaluationincontrolgroupand thelackofassessementof splenicfunction,sincec-SLEpatientscouldpresentfunctional asplenia.14
Hepatomegaly is acommon finding atdisease onset in
c-SLE patients and adult SLE.2,3,15 During disease course, liverenlargementinlupuspatients,eitherchildrenoradults, maybeassociatedwithhepaticcongestion,fattyinfiltration, autoimmuneandviralhepatitis,metabolicdisorders, throm-bosisorhepatotoxicdrugsusage.2,15,16
Ourpatients had localized right-liverhypertrophy asso-ciatedwith disease activity, suggesting the same systemic
pathogenesismechanism.Thesepatientshadmildand
sub-clinical liverenlargementprobablydue tolivercongestion, liverchronicinflammationandhypervascularization.Ofnote,
this enlargement was associated with severe disease and
correlatedwithvariousclinicalandlaboratorydisease param-eters.Indeed,theautopsyregistrydataofthe livershowed that hepatic congestion, liver chronicinflammationand/or liverarteritiswereobservedin77%ofadultandc-SLEpatients andmaybereflectinglupusactivity.15Positivecorrelationwas alsofoundbetweendiseaseactivityparametersand longitu-dinalspleendimension,despitetheabsence ofclinicaland
sonographysplenomegaly.
Damagetohepatocytecellseemsnottoberelevantherein, sincenoneofourpatientshadelevatedlevelsofliverenzymes. Moreover,corticosteroiduse,aknowncauseofhepatomegaly andfattyliverdisease,mayhavenotcontributedto enlarge-mentofthisorganinthepresentstudy.2,15
BothpediatricandadultSLEpatientsmaypresentsplenic atrophy.14,17Importantly,ourchildrenandadolescentlupus patients with long disease duration presented spleen size reduction, thus indicating splenic atrophy during the dis-easecourse.Apreviousstudy evaluatingadultSLEpatients foundthatsplenicatrophyhad nocorrelationwithdisease duration.17However,themechanismsofspleenatrophyand functionalaspleniaarestillnotclearinpediatricandadultSLE populationsandfurtherstudieswillbenecessary.
Inconclusion,ourdataraisesthepossibilitythatdisease activitycouldleadtosubclinicalandlocalizedhepatomegaly. We hypothesize that liver is a potential target organ for activelupusduringthediseasecourse.Longdiseaseduration resultedtospleenatrophyinc-SLEpatients.
Funding
ThisstudywassupportedbygrantsfromFundac¸ãodeAmparo àPesquisadoEstadodeSãoPaulo (FAPESP2011/12471-2to CAS),ConselhoNacionaldeDesenvolvimentoCientíficoe Tec-nológico(CNPQ302724/2011-7toCAS),FedericoFoundation(to CAS),andNúcleodeApoioàPesquisa“SaúdedaCrianc¸aedo Adolescente”ofUSP(NAP-CriAd)toCAS.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgement
OurgratitudetoUlyssesDoria-Filhoforthestatisticalanalysis.
r
e
f
e
r
e
n
c
e
s
1.SilvaCA,AvcinT,BrunnerHI.Taxonomyforsystemiclupus erythematosuswithonsetbeforeadulthood.ArthritisCare Res(Hoboken).2012;64:1787–93.
2.DeenME,PortaG,FiorotFJ,CamposLM,SallumAM,SilvaCA. Autoimmunehepatitisandjuvenilesystemiclupus
erythematosus.Lupus.2009;18:747–51.
3.CamposLM,OmoriCH,LotitoAP,JesusAA,PortaG,SilvaCA. Acutepancreatitisinjuvenilesystemiclupuserythematosus: amanifestationofmacrophageactivationsyndrome?Lupus. 2010;19:1654–8.
4.LucenaSM,OliveiraIR,WidmanA,ChammasMC,OliveiraLA, CerriGG.Sonographicbiometricsoftheliverinchildren: proposalofanewmethod.RadiolBras.2003;36:63–70.
5.Konus¸OL,OzdemirA,AkkayaA,Erbas¸G,CelikH,Is¸ikS. Normalliver,spleen,andkidneydimensionsinneonates, infants,andchildren:evaluationwithsonography.AmJ Roentgenol.1998;171:1693–8.
6.HochbergMC.UpdatingtheAmericanCollegeof Rheumatologyrevisedcriteriafortheclassificationof systemiclupuserythematosus.ArthritisRheum. 1997;40:1725.
7.GladmanDD,Iba ˜nezD,UrowitzMB.Systemiclupus erythematosusdiseaseactivityindex2000.JRheumatol. 2002;29:288–91.
8.BrunnerHI,SilvermanED,BombardierC,FeldmanBM. EuropeanConsensusLupusActivityMeasurementis sensitivetochangeindiseaseactivityinchildhood-onset systemiclupuserythematosus.ArthritisRheum.2003;49: 335–41.
9.BrunnerHI,FeldmanBM,BombardierC,SilvermanED. SensitivityoftheSystemicLupusErythematosusDisease ActivityIndex,BritishIslesLupusAssessmentGroupIndex, andSystemicLupusActivityMeasureintheevaluationof clinicalchangeinchildhood-onsetsystemiclupus erythematosus.ArthritisRheum.1999;42:1354–60.
10.GladmanD,GinzlerE,GoldsmithC,FortinP,LiangM,Urowitz M,etal.Thedevelopmentandinitialvalidationofthe SystemicLupusInternationalCollaboratingClinics/American CollegeofRheumatologydamageindexforsystemiclupus erythematosus.ArthritisRheum.1996;39:363–9.
11.BrandtJT,TriplettDA,AlvingB,ScharrerI.Criteriaforthe diagnosisoflupusanticoagulants:anupdate.Onbehalfofthe SubcommitteeonLupusAnticoagulant/Antiphospholipid AntibodyoftheScientificandStandardisationCommitteeof theISTH.ThrombHaemost.1995;74:1185–90.
12.JesusAA,JacobCM,SilvaCA,DornaM,PastorinoAC, Carneiro-SampaioM.Commonvariableimmunodeficiency associatedwithhepatosplenicT-celllymphomamimicking juvenilesystemiclupuserythematosus.ClinDevImmunol. 2011;2011:428703.
13.AikawaNE,JesusAA,LiphausBL,SilvaCA,Carneiro-Sampaio M,VianaVS,etal.Organ-specificautoantibodiesand autoimmunediseasesinjuvenilesystemiclupus
erythematosusandjuveniledermatomyositispatients.Clin ExpRheumatol.2012;30:126–31.
15.MatsumotoT,YoshimineT,ShimouchiK,ShiotuH,Kuwabara N,FukudaY,etal.Theliverinsystemiclupuserythematosus: pathologicanalysisof52casesandreviewofJapanese AutopsyRegistryData.HumPathol.1992;23:1151–8.
16.RavelliA,CariaMC,MalattiaC,TemporiniF,CavalleroA, SiliniEM,etal.Uncommoncausesofliverdiseaseinjuvenile
systemiclupuserythematosus.ClinExpRheumatol. 2001;19:474.