BrazJOtorhinolaryngol.2017;83(5):602---604
www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
CASE
REPORT
Thyroid
compressive
mass,
a
metastasis
of
femur
chondrosarcoma
after
14
years:
case
report
and
literature
review
夽
Tumor
compressivo
tireoidiano,
uma
metástase
de
condrossarcoma
femoral
após
14
anos:
relato
de
caso
e
revisão
da
literatura
Franc
¸ois
Simon
a,∗,
Marion
Classe
b,
Pierre
Vironneau
a,
Michel
Wassef
b,
Philippe
Herman
a,
Nicolas
Le
Clerc
aaParisDiderotUniversity,HôpitalLariboisière,DepartmentofOtorhinolaryngology,AP-HP,Paris,France bParisDiderotUniversity,AP-HP,HôpitalLariboisière,DepartmentofPathology,Paris,France
Received13August2015;accepted16September2015 Availableonline18December2015
Introduction
Intrathyroidmetastasesrepresentonetothreepercentof thyroid cancers1---3; however, intrathyroid chondrosarcoma
metastasesareveryrareindeed,asthereare,toour knowl-edge,only fourother cases reported in the literature.4---6
Thiscasestandsout,asthethyroidmassappeared14years afterthetreatmentoftheinitialchondrosarcoma,without anyotherlocalofdistantrecurrence.
Case
report
AmalepatientofMoroccandescent,62yearsofage,came toour department in 2014 for a large mass centered on
夽 Pleasecitethisarticleas:SimonF,ClasseM,VironneauP,Wassef M,HermanP,LeClercN.Thyroidcompressivemass,ametastasis offemurchondrosarcomaafter14years:casereportandliterature review.BrazJOtorhinolaryngol.2017;83:602---4.
∗Correspondingauthor.
E-mail:[email protected](F.Simon).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileirade OtorrinolaringologiaeCirurgiaCérvico-Facial.
therightthyroidlobe.Medicalhistoryincludedhighblood pressure,obesityandtype2diabetes,withseverechronic kidney failure.He hadalsobeen operated successfully 14 yearsagoinourhospitalforachondrosarcomaoftheright femur.Acloseclinical,yearlyfollow-uphad,todate,shown nolocalordistantrecurrence,andthepatienthadno func-tionaldeficit.Atthetime,thepatienthadconsultedinthe orthopedicdepartmentofourhospitalforpainintheupper leg,whichhadbeenincreasingforoverayear.Abiopsyin January2000diagnosedachondrosarcoma.Thepatientwas operatedtwomonthslater,andalargeexcisionofthefemur and the surroundingmuscles (includingthe biopsy needle path)wasperformed.Thetumormeasured60mm×40mm
andwascenteredonthegreattrochanterandfemurneck. TheanalysisfoundagradeIIchondrosarcomawithcortical bonelysis(Fig.1),withwideresectionmargins.Therewas nofurtherradiotherapyorchemotherapy.
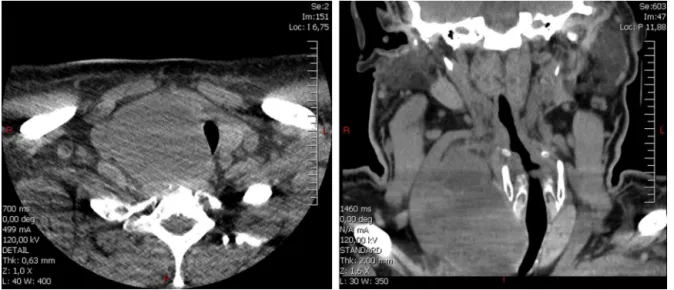
The patient came toour department in June 2014 for a thyroid mass which had been growing over the past few months and was becoming compressive. The patient presented mild dysphagia and dyspnea. The endoscopic examination revealed adeviated trachea, but goodvocal cord function. The CT-scan (Fig. 2) showed a large mass in theright thyroid lobewithan importanttracheal devi-ation, without any adenopathy. An ultrasound found a
http://dx.doi.org/10.1016/j.bjorl.2015.09.008
Thyroidmetastasisoffemurchondrosarcoma 603
Figure1 Comparisonofhistologyoftheinitialchondrosarcoma(right)andthyroidmetastasis14yearslater(leftandcenter). Bothlesionswereconfirmedtobeidenticalbyalaboratoryspecializedinsarcoma(OscarLambretinLille,France).Left:thyroid metastasis,HESstaining×2.5;myxoidtumorinfiltratingthethyroidtissueanddissociatingthyroidvesicles.Center:vascularinvasion
inthethyroidmetastasis;HESstaining×10;clusterofdedifferentiatedchondrocytesinamyxoidstroma,coveredbyanendothelial
layerinavessellumen.Right:femurchondrosarcoma,HESstaining×2.5;showingmassiveboneresorptionbyamyxoidandchondroid
tumor.
Figure2 CT-scanofthethyroidmass.Duetothepatient’schronickidneyfailure,intravenouscontrastcouldnotbeused.Note theimportanttrachealcompressiononthetransverseplane(left)andimportanttrachealandvesseldeviationonthecoronalplane (right).Themassmeasured90mm×54mm×68mm.
heterogenic mass measuring 90mm×54mm×68mm US
guidedfine-needleaspirationwasnotconclusive(veryfew cells). Thyroidblood testswere normal (TSH,T3, T4 and antibodies),andthepatientdidnotpresentanyhormonal disorders.
Duetothecompressivesymptomsandlackofdiagnosis, a total thyroidectomy wasperformed three months later. Otherthanthesize,themainoperativedifficultywas sep-aratingthe massfrom thecarotid artery,to whichit was veryadherent.Additionally,acysticmassintheright lobe wasopen laterally,andthe muscles coveringithad tobe included in the resection. The right recurrent nerve was locatedininflammatorytissueinbetweenthemassandthe trachea and was difficult to dissect. Perioperative frozen sectionswerenon-conclusive. The patientwasdischarged afterfivedays,andtheimmediatefollow-upshowedpartial right recurrent nerve palsywithout any functional conse-quence.
Analysisofthemassinourhospitalshowedacystic myx-oid tumor measuringover 40mm, identical to the femur lesion treated 14 years earlier. It also showed vascular
invasionand infiltration of thelateral aspect of the right thyroid lobe. A probable chondrosarcoma metastasis was diagnosed(Fig.1).Thehistologyslidesofthyroidandfemur lesionswere sent to a sarcoma reference center (Center OscarLambret, Lille,France),and thediagnosis was con-firmed.
The case was then discussed in a sarcoma specialized board. No further treatment was decided regarding the thyroid metastasis, as the surgical excision was deemed complete.However,asecondmetastasis(10cm)intheright lungwasdiscovered,promptingfurtherpulmonarysurgery (lobectomy).Inthefollowingmonths,asecond pulmonary metastasisandaninoperablecervicalrecurrencewere dis-covered.Thepatientdiedthreemonthslaterafterpalliative chemotherapy.
Discussion
604 SimonFetal.
examinations have revealed that asymptomatic thyroid metastasisaremuchmorecommon,inupto24percentof cases.2Studiesshowthatintrathyroidmetastasesaremostly
duetokidneyorotherwiselungandbreastcancer.1---3Inmost
cases,thethyroidmetastasesareassociatedwithmultifocal metastases,withaverylowsurvivalrate.Thyroidectomyis usuallyperformedtopreventlocalcomplications (compres-siveorinvasive)andtohelpdiagnosetheprimarycancer.1---3
As in this case, metastases to the thyroid are known to sometimesoccur decadesafter theprimary cancer.1---4 We
haveonlyfoundintheliteraturethreecasesof chondrosar-comametastasizing tothe thyroid,emphasizing howrare thiscondition is.In allcases,the patientsrapidly diedof multiplemetastases.4,5
Chondrosarcoma has a high level of local recurrence, andthecommontreatment issurgerywithalarge enbloc excision,astheyareusuallyresistanttoradiotherapyand chemotherapy.7,8 Follow-up must be over a long period,
as metastases are known to appear over a decade after theprimarylesion.7---10 AlthoughgradeIIIlesionsoftenhave
metastasis,gradeIneverdo,andgradeIIonlydoin10 per-centofcases;therefore,lowgradetumorshaveanexcellent survivalrateafterlargeresection.9
Treatment of chondrosarcomas in the head and neck differs, as they are usually low grade with a low risk of metastasis.9,10 Furthermore,likeinthis case,ascomplete
resectionwithmarginsisrarely possible(especiallyinthe skullbase),adjuvantradiotherapyisoftenperformedafter surgery.7,10
Inthiscase, adjuvantradiotherapywasconsidereddue tothemuscleinvasionandadherencetothecarotidartery andtheabsenceofresectionofthefine-needleaspiration path,whichisusuallyperformedinchondrosarcoma.Infact, thecervicalsurgerywasdeemedsufficient,andthepriority wasshiftedtothelung.Retrospectively,amoreaggressive stanceonthecervicallocationshouldhavebeenchosen.
Conclusion
Wereportaveryrarecaseofchondrosarcomametastasisto thethyroidgland.Asinthefewothercasesreportedinthe literature,itappearedmanyyearsaftertheprimarycancer. Thyroidmetastasesofchondrosarcomaorothercancersare generallyassociatedwithothermetastaticlesionsand,asin theothercasereports,thepatientrapidlydiedofmultiple metastases.Thisemphasizesthefactthatchondrosarcoma
patients,evenwhensuccessfullytreatedinthepast,must alwaysbetreatedcautiouslywhenpresentingamass.Also, othermetastaticsites,especiallythelung,mustbeactively sought.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgement
Theauthorswouldliketoexpresstheirsinceregratitudeto Yves-Marie Robin ofthe Oscar Lambret Centerin Lillefor confirmingthehistopathologicaldiagnosis.
References
1.MirallieE,RigaudJ,MathonnetM,GibelinH,RegenetN,Hamy A,etal.Managementandprognosisofmetastasestothethyroid gland.JAmCollSurg.2005;200:203---7.
2.WoodK,ViniL,HarmerC.Metastasestothethyroidgland:the RoyalMarsdenexperience.EurJSurgOncol.2004;30:583---8. 3.CalzolariF,SartoriPV, TalaricoC,ParmeggianiD,Beretta E,
Pezzullo L, et al. Surgical treatment of intrathyroid metas-tases:preliminaryresultsofamulticentricstudy.Anticancer Res.2008;28:2885---8.
4.BakxPA,vandenInghHF,BaggenRG,VeenHF,OosterhuisWJ. Anunusualmetastasisofachondrosarcomainthethyroidgland. EurJSurg.1993;159:643---4.
5.DarouassiY, Touati MM, Chihani M, Nadour K, Boussouga M, Ammar H, et al. Chondrosarcoma metastasis in the thyroid gland:acasereport.JMedCaseRep.2014;8:157.
6.OrtizS,TortosaF,SobrinhoSimoesM.Anextraordinarycaseof mesenchymalchondrosarcomametastasisinthethyroid.Endocr Pathol.2015;26:33---6.
7.Coca-PelazA,RodrigoJP,TriantafyllouA,HuntJL, Fernandez-MirandaJC,StrojanP,etal.Chondrosarcomasoftheheadand neck.EurArchOtorhinolaryngol.2014;271:2601---9.
8.GoedhartLM,PloegmakersJJ,KroonHM,ZwartkruisEC,Jutte PC. The presentation, treatment and outcome of periosteal chondrosarcoma in the Netherlands. Bone Joint J. 2014;96-b:823---8.
9.EvansHL,AyalaAG,RomsdahlMM.Prognosticfactorsin chon-drosarcomaofbone:aclinicopathologicanalysiswithemphasis onhistologicgrading.Cancer.1977;40:818---31.