www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
CASE
REPORT
Subtotal
arytenoidectomy
for
the
treatment
of
laryngeal
stridor
in
multiple
system
atrophy:
phonatory
and
swallowing
results
夽
Aritenoidectomia
subtotal
para
o
tratamento
de
estridor
laríngeo
na
atrofia
de
múltiplos
sistemas:
resultados
na
fonac
¸ão
e
deglutic
¸ão
Francesco
Stomeo
a,∗,
Vittorio
Rispoli
b,
Mariachiara
Sensi
b,
Antonio
Pastore
a,
Nicola
Malagutti
a,
Stefano
Pelucchi
aaSpecialisticSurgeryDepartment,PhonosurgeryUnit,ArcispedaleS.Anna,Cona,Italy bNeuroscienceDepartment,MovementDisorderUnit,ArcispedaleS.Anna,Cona,Italy
Received27March2015;accepted31March2015 Availableonline9September2015
Introduction
Multiplesystematrophy(MSA),accordingtosecond
consen-sus on MSA, is a neurological disorder characterized by
a combination of autonomic failure and parkinsonism, or
cerebellar ataxia, or both.1 Among MSA manifestations,
diurnal and nocturnal inspiratory stridor associated with
sleepapnoeamay help in clinical diagnosis, and itsmost
accepted explanationis vocal folds abductor dysfunction.
Apossiblecomplicationof thissituationissudden
noctur-naldeath.Asdescribedintheliterature,theuseofC-PAP
andtracheotomyarethemostcommontreatmentproposed
forthetherapyofthelaryngealdisfunction.2Alternatively
laterofixationofthevocalfoldaccordingtoEjnell3orlaser
arytenoidectomyhavebeenproposed.Herewepresentthe
夽
Pleasecitethisarticleas:StomeoF,RispoliV,SensiM,Pastore A,MalaguttiN,PelucchiS.Subtotalarytenoidectomyforthe treat-mentoflaryngealstridorinmultiplesystematrophy:phonatoryand swallowingresults.BrazJOtorhinolaryngol.2016;82:116---20.
∗Correspondingauthor.
E-mail:[email protected](F.Stomeo).
caseofnocturnalinspiratorystridorinaMSApatienttreated
with CO2 laser subtotal aritenoidectomy, with particular
attentiononphonatoryandswallowingoutcome.
Case
report
We report the case of a 60-year-old man with a
5-year history of rigid-akinetic syndrome, unbalance, mild
orthostatichypotensionandRembehaviourdisorder.Since
2yearshepresented cornage,markedwearinessand
dys-pneaduringnightanddaytimeatrest. Pneumologicaland
cardiological investigations were made without any clear
diagnosis;cognitivetestsdidnotshowanyimpairment.The
diagnosis of possible MSA-P was therefore made. During
follow-up no more clinical feature was added, in
partic-ular the patient presented mild and slow worsening of
motorandnon-motorsymptoms.Heremainedindependent
in activity daily living (ADL) and in activity
instrumen-tal daily living (IADL). The most life-threatening feature
wasthe two-yearhistory ofsnoring andsleepapnea with
referred nocturnal stridor and occasional stridor during
wakefulness.InFebruary2013,anendoscopicevaluationof
larynxshowedareducedvocalfoldabductionduring
inspi-ration with reduction of the breathing space. Vocal folds
http://dx.doi.org/10.1016/j.bjorl.2015.03.016
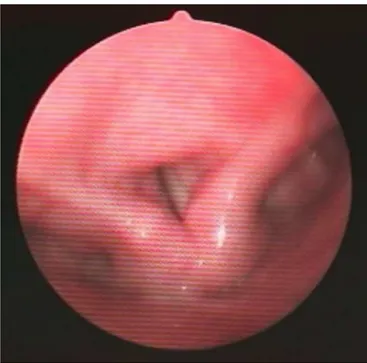
Figure1 Theendoscopyexecutedduringsleepevidencesthe paradoxicalmovementofadductionduringinspiration.
adduction was normal with no alteration of voice.
Alaryngealelectromyographywasperformed bothon
thy-roarytenoid and cricoarytenoidal muscles: no denervation
activity,butanalterationofmaximumrecruitment during
phonation and deep breathing was observed.
Polysomno-graphy highlighted an OSA syndrome of mild grade, an
apnea-hypopnoea index (AHI) of 9.2 with lowest SpO2 at
88%.Swallowevaluatedwithanamnesisandwithendoscopic
andradiologicaldynamic studyof swallowingwasnormal.
APropofol-inducedSleepEndoscopy(PDSE)wasperformed
using a low dose of propofol (0.01mg/kg) followed by a
titrationofpropofol(3mg/kg/hr).Theendoscopyrevealed
a paradoxical movement of adduction during inspiration
(Fig.1)withamarkedinspiratorystridor,whileexpiratory
abductionmovementofthevocalfoldswasconserved.
A surgical treatment of the glottis was considered
becausethepatientrefusedthehypothesisofC-PAPandany
futuretracheotomy.Perceptualevaluationofvoice
accord-ingtoGIRBASscale,4 evidenced amildalterationof voice
(G1R0B1A0S0);thespectrographicexaminationcarriedout
usingCSL model 4500 B(Kay Elemetrics Corp.) by means
ofanarrowbandfilteroftheprolongedvowels‘‘a’’andof
theItalianword‘‘aiuole’’wasclassifiedinthesecondclass,
accordingtoYanagihara classification;finally,an
examina-tion of voice using the Multi-Dimensional Voice Program
(MDVP)by Kay elemetricsshowed alterationof frequency
perturbation(Jitt --- 1.564;RAP --- 0.924; vF0--- 2.366), as
wellasamplitudeperturbations(ShdB---0.562;Shim---6.246;
vAm---17.635)withamildalterationofnoisetoharmonic
ratio(NHR=0.156)(Fig.2).Maximumphonatorytime(MPT)
was11seconds.Self-evaluationofvoicewithvoicehandicap
index(VHI)5 wassubmittedtopatientinordertomeasure
physical, emotional and functional complaints of
dyspho-nia; preoperatory score was of 5 (mild alteration). Then
Single token
Threshold
DSH
DUV
Jita
Jitt
RAP
PPQ
sPPQ
vFo
ShdB
Shim
APQ vAm
NHR VTI
SPI FTRI
sAPQ DVB
Figure3 Thecontrolendoscopyexecutedattwomonthsfrom surgeryshowsthegoodincreaseoftheglotticrespiratoryspace.
subtotal arytenoidectomy was performed using CO2 laser
at 6-10 watt in continuous mode according to Remacle
technique,6 withthe resectionof arytenoid body andthe
preservationofasmallposteriorshellofthiscartilage.The
two-months control endoscopy (Fig. 3) evidenced a good
increaseoftheglotticrespiratoryspace.Post-surgical
per-ceptualevaluationofvoiceremainedgood(G1R0B2A0S0
---mild alteration), the spectrographic examination (Fig. 4)
showed a mild worsening of NHR and a dyplophonia. At
MDVP evaluation, all the above mentioned values were
slightly worsened (Fig. 5), but no modification of voice
qualitywasperceived bythe patientand hispost-surgical
VHI had a score of 8 (mild alteration). MPT remained
unchanged (11seconds). Swallowing evaluated with PAS
(penetration/aspirationscale)evidenced nosignsof
pene-tration/aspiration.Nocturnalstridoranddyspneadefinitely
improved.Aftertwoyears,patient’sconditionisstablewith
noalterationsinbreathingandswallowing.
Discussion
Multiple system atrophy (MSA) is an adult-onset sporadic
andrapidlyprogressiveneurodegenerativedisorder,
charac-terized byautonomic failureassociated withparkinsonian
featuresand/orcerebellarataxiaandawidevarietyofother
clinical findings that rarely presents with predominance
of respiratorydisorders(respiratoryfailureorstridor).1 In
literature,fewcasesofMSAwithprolongeddurationof
dis-ease (more than 15 years)have been reported,7 but it is
notclearwhichsymptomatonset,betweendysautonomia
andparkinsonism,correlateswithslowerprogression.7The
initial multisystem involvement or the shortlatency from
one-system-disease tomultiple-system-disease stagehave
beenidentifiedasbadpredictorfordiseaseprogressionand
survival.7Inourpatientmotoranddisautonomicsymptoms
startedsimultaneously,whereasstridorappearedlater.
Dur-ingthefirst5-yearfollow-up,thedopaminergictreatment
wasnot necessary, due toslightmotor involvement.
Stri-dor is defined asa harsh, strained inspiratory soundwith
a pitch at 260-330Hz higher than snoring. It occurs
dur-inginspiration,reflectinganupperairwayobstruction due
to partial or complete vocal cord abduction impairment.
Stridor,that is considereda redflag ofMSA,has a
preva-lenceof34-41%inMSAandrepresentstheopeningfeature
in 4% of cases. It is considered a life-threatening
condi-tion,leadingtosubacuteepisodesof dramaticrespiratory
failureanddeath.7Twotheoriestrytoexplainits
etiopatho-genesis: the first, ‘‘respiratory center damage’’ theory,
attributestheMSAneurodegenerativeprocesstoabnormal
outputs fromtherespiratorynetworkthat inducea
selec-tive paralysis of the abductor with relative preservation
of adductor functions. The second one, ‘‘reflex theory’’,
hypothesizesaparadoxicalactivationofthelaryngeal
clo-sure reflex, that normally protects subglottic space from
strongnegativepressure;MSA-stridorwouldresultnotonly
fromapassiveglottisnarrowing,attributedbothtoabductor
paralysisandBernoullieffect,butaccordingtoreflextheory,
4000
3000
2000
1000
0
8.0 9.0 10.0
Time (sec)
F
requency (Hz)
Single token
Threshold
DSH
DUV
Jita
Jitt
RAP
PPQ
sPPQ
vFo
ShdB
Shim
APQ vAm
NHR VTI
SPI FTRI
sAPQ DVB
Figure5 Themultidimensionalvoiceprogramevidencesthepostoperatorymildworseningoftheperturbationsinfrequencyand amplitude.
from an active narrowing of vocal fold. Hyper-activation
oflaryngealclosurereflexistriggeredbyincreasingdropof
pressureduringvoluntaryinspiration.In MSApatients,the
glotticspaceisreducedbypassiveforces,therefore
laryn-gealclosurereflexbuildsupaviciouscyclethatpromotes
an activevocalcordsnarrowing and,thenstridor.In fact,
oncevoluntaryinspirationandnegativeairwayspressureare
erased(throughtracheostomyorCPAP),stridordisappears.2
Stridorandlaryngealdysfunctiondevelopduringthecourse
of disease: in thefirst stages, during wakefulness, only a
slightly impaired vocal cordabductionor flicker or ataxic
movements ofthe vocal cords, and periodicor persistent
involuntary adductions or abductions of the vocal cords
may be present2; in intermediate and late stages, the
restricted glottis and abductor paralysis develop causing
daytimestridor.2 Stridorassociated witha decreased
sur-vivalistheonlyindependentpredictivesurvivalfactor,but
itisnottheonlyonecauseofsuddendeathinparkinsonian
syndromes.CPAP andtracheotomyincreasesurvivalrates,
althoughtherearesomereportsofsuddendeathevenafter
these treatments, probably due to central sleep apnoea.
Lasertreatment oftheposteriorglottisinadduction
bilat-eralvocalfoldpalsycanbeanappropriatewaytosolvethe
respiratoryproblembecause,preservesthephonatory
func-tion,penalizing the posterior glottiswhose main function
istherespiratoryoneandwhoseinfluence isnot
determi-nantonvoicequality.8Amongthelasertechniques,Remacle
sub-totalaritenoidectomy,whileincreasingtheglottic
respi-ratoryspace,ensuresagoodphonatoryoutcome,andwith
agoodfixationofthearytenoidregion,minimizestheriskof
aspiration.We believethat,in selectedcasesof MSAwith
subtotalglottic pattern of restriction,9 if respiratory
stri-dorispresent duringwakefulness andthepatientdoesn’t
toleratethe C-PAP and refuses apossible tracheotomy, it
is possible to perform a CO2 laser subtotal
arytenoidec-tomy to restore an adequate airflow through the glottis.
To our knowledge, in the literature only two authors9,10
haveinvestigatedthesurgicaloptionsforthetreatmentof
glottic obstructionsin MSApatients, but theyproposed a
completeremovalofarytenoidcartilagewithpartial
sacri-ficeofthyroarytenoidmuscleortheEjnelltechnique3;their
evaluationof voicequalityafter waslimited,in one case
toGirbasscale,and,intheother one,tolimited
parame-tersofvoice.Ourevaluationbasedonself-perception(VHI),
perceptiveevaluation of voice quality(GIRBAS scale), on
spectralanalysisofphonatoryresultsaswellonevaluation
of deglutition,shows that Remacle technique is effective
andensuresonlyamildworseningofvoicequality,whilea
lowerimpactonswallowingisguaranteedcomparedtothe
previousproposals.
Conclusion
We recommend laser subtotal arytenoidectomy in MSA
patients affected by nocturnal stridor due to a
paradoxi-caladduction inspiratorymovement, but selection of the
alterationsinthenormalprocessofdeglutitionarepresent
surgical procedures altering the glottic plane must be
avoided.
Funding
This researchreceivednospecific grantfrom anyfunding
agencyinthepublic,commercialornot-for-profitsectors.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.GilmanS, Wenning GK, LowPA, BrooksDJ, MathiasCJ, Tro-janowskiJQ,etal.Secondconsensusstatementonthediagnosis ofmultiplesystematrophy.Neurology.2008;26:670---6.
2.ShibaK,IsonoS,NakazawaK.Paradoxicalvocalcordmotion:a reviewfocusedonmultiplesystematrophy.AurisNasusLarynx. 2007;34:443---52.
3.EjnellH,ManssonI,HallénO,BakeB,StenborgR,LindströmJ. Asimpleoperationforbilateralvocalcordparalysis. Laryngo-scope.1984;94:954---8.
4.HiranoM.Clinicalexaminationofvoice.In:ArnoldGE,Winckel F, Wyke BD, editors. Disorders of Human Communication. Springer-Verlag:NewYork;1981.p.81---4.
5.Stomeo F,Tosin E, Morolli F, Bianchini C,Ciorba A, Pastore A, et al. Comparison of subjective and objective tools in transoral laser cordectomy for early glottic cancer: impor-tanceofvoicehandicapindex.IntJImmunopatholPharmacol. 2013;26:445---51.
6.Remacle M, Lawson G, Mayné A, Jamart J. Subtotalcarbon dioxide laser arytenoidectomy by endoscopic approach for treatmentofbilateralcordimmobilityinadduction.AnnOtol RhinolLaryngol.1996;105:438---45.
7.WatanabeH,SaitoY,TeraoS,AndoT,KachiT,MukaiE,etal. Pro-gressionandprognosisinmultiplesystematrophy:ananalysis of230Japanesepatients.Brain.2002;125:1070---83.
8.LawsonG,RemacleM,HamoirM,JamartJ.Posterior cordec-tomy and subtotal arytenoidectomy for the treatment of bilateral vocal fold immobility: functional results. J Voice. 1996;10:314---9.
9.ChitoseS,KikuchiA,IkezonoK,UmenoH,NakashimaT.Effectof laserarytenoidectomyonrespiratorystridorcausedbymultiple systematrophy.JClinSleepMed.2012;8:713---5.