ISSN 2321-1822
Original Article
EFFECTS OF STOTT’S PILATES VERSU S YOGIC EXERCISE IN
FIBROM YALGIA PATIENTS: A PILOT STUDY
Ashika Tanna *
1, Soumik Basu
2, Kajal Anadkat
3.
* 1 M .P.T. Ort hopaedics, YTTC, Assistant Professor, School of Physiot herapy, R.K.Universit y, Tramba,
Gujarat , India.
2 M .P.T. in Sport s Sciences, Assistant professor, Depart ment of Physiot herapy, Padmashree Dr.
D.Y.Pat il M edical College and Research Inst it ute, Pimpri, Pune, India.
3 M .P.T. M usculoskelet al and Sport s Science, Assist ant Professor, School of Physiot herapy,
R.K.Universit y, Tramba, Gujarat , India.
Background: Fibrom yalgiaSyndrom e (FM S) can be defined as a r heum at ological condit ion char act erised by chr onic w idespread pain. A reduced pain t hreshold as w ell as hyperalgesia and allodynia. It is a nonart icular painful condit ion w it h generalised t ender point s.
Purpose:The aim of t his random ised st udy w as t o com pare t he effect s of St ott ’s Pilat es versus Yogic exercise on pain, t ender ness, pr essur e t hr eshold , depr essi on & f at igue in Fibr om yalgia p at ient s, w hich is ch r oni c m usculoskelet al disorder.
M et hodology:Fem ale and m ale (n=20) w ho had a diagnosis of fibr om yalgia syndr om e (FM S) according t o t he Am er ican College of Rheum at ology cr it eria w ere select ed from Dr. D.Y.Pat il hospital, Physiot herapy depart m ent O.P.D. The part icipant s w ere random ly assigned int o 2 groups. In group A, a Pilat es exercise program of 1 hour w as given by a cert ified t rainer t o 10 part icipant s 6 days a w eek for 4 w eeks. In group B, Yoga program of 1 hour w as given by cert ified inst ruct or t o10 part icipant s 6 days a w eek f or 4 w eeks. In bot h groups, pre- (1st day) and post t reat m ent (4t h w eek) evaluat ion w as perform ed by VAS (Visual Analogue Scale), TPI (Tender Point Index), AS
(Algom et ric Score), BDI (Beck Depression Invent ory) and FSS (Fat igue Severit y Scale).
Results:Tw ent y part icipant s com plet ed t he st udy. In Group A significant difference w ere obser ved for VAS, TPI, BDI & FSS (st at ist ically p<0.05) and in Group B significant difference w ere observed for VAS, TPI, AS, BDI & FSS (st at ist ically p<0.05). But bet w een group com parison result w as not suppor t s t he w it hin group dif ferences (st at ist ically p>0.05).
Conclusion: Hence, w e suggest Pilat es exercise and Yoga bot h are equally effect ive in t reat ing fibromyalgia pat ient s.
KEY W ORDS:Fibromyalgia, Pressure Algom et er, St ott ’s Pi lat es, Yoga.
ABSTRACT
INTRODUCTION
Address for correspondence: Dr. Ashika Tanna, M .P.T. Ort hopaedics, YTTC, Assistant Professor, School of Physiot herapy, R.K.Universit y, Tramba, Gujarat , India. Contact No. +91-9978469090 E-M ail: [email protected] / [email protected]
Int J Physiother Res 2015, Vol 3(5):1250-57. ISSN 2321-1822 DOI: ht t p:/ / dx.doi.org/10.16965/ ijpr.2015.186
Quick Response code
Access this Article online
International Journal of Physiotherapy and Research ISSN 2321- 1822
w w w.ijm hr.org/ ijpr.htm l
DOI: 10.16965/ ijpr.2015.186
Received: 22-09-2015 Peer Review : 22-09-2015 Revised: None
Accept ed: 01-10-2015 Published (O): 11-10-2015 Published (P): 11-10-2015
and allodynia. It is an idiopat hic, nonart icular pain syndrom e pr esent ing w it h generalised t end er p o i nt s. It is a m u l t i sy st em an d m ult ifact orial disease charact erised by sleep d i st u r ban ce, f at i gue, h ead ach e, m o r ni n g Fi bromyalgia Syndrom e (FM S) is a com m on
ISSN 2321-1822
fostering more efficient movement patt erns. This is similar in principle t o t he dynamic st abilization exercises w idely used in t he t reat m ent and prevent ion of m usculoskeletal low back pain (LBP), w hich advocat es promot ing efficiency of deep st abilizers and decreasing cont ract ion of muscles count erproduct ive t o t he act ivit y [3].
St ot t Pilat es is a version of t he Pilat es met hod of physical exercise. It was developed by Lindsay and M oira M err it hew. The m ost signif icant difference bet w een St ot t Pilat es and Joseph Pilates’s (w hich was original met hod of t he early 1900s) is t hat , w here t he original met hod uses a st raight spine during exercise, St ot t Pilat es focuses on maint aining t he nat ural curvat ure of t he spine.
“ Yoga” derives from t he Sanskrit w ord ‘yukt i’ m ean i n g “ u ni o n ,” aim i n g t o un i f y sp ir i t (consciousness) w it h super spirit (God). Yoga is one of t he six systems of Indian Vedic philosophy (Darshan). M aharishi Pat anjali, right ly know n as t he “ Fat her of Yoga,” com piled and ref ined various aspect s of yoga syst em at ically in his “ Yo ga Su t ras” (ap ho r i sm s), w h er ei n h e ad vo cat ed t h e ei gh t -f o ld p at h kn o w n as “Ashtanga Yoga” for an all-around development of hum an personalit y. These include - Yam a [m oral codes], Niyam a [self-purificat ion and st udy], Asana [post ur e], Pranayam a [breat h cont rol], Prat yahara [sense cont rol], Dharana [ concent r at ion] , Dhyana [ m edit at ion] , and Sam adhi [ super cont em plat ion] . These ar e f o r m u l at ed o n t h e basi s o f m u l t if ar io u s p sy ch ol o gical u n d er st an d i ng o f h u m an personalit y [4,5].
The st rongest evidence in bot h qualit y and quant it y suggest s yoga has a posit ive impact on hormone regulat ion. Salivary levels of cortisol have been measured and not ably decreased in FM S pat ient s in numerous review s and t rials [6-9]. Yoga leads t o increased cort isol is associated w it h decreasing perceived st ress, decreasing anxiet y, increasing feelings of w ell-being and
improving pain management [10,11]and higher
levels of melat onin t o improve imm unit y and sleep qualit y [12,13] are ot her pot ent ial effect s of yoga pract ice. Alt hough individual asana and pr an ay am pr act ices can select i vely af f ect sympathetic or parasympathetic nervous system, t he overall effect of yoga pract ice is t o bring a st iffness, parest hesias, anxiet y, depression and
some ot her psychological sympt oms [1,2].In the
most of cases of fibromyalgia, t he causes are unknow n. Physical injuries, emot ional t rauma, or viral infect ions may t rigger t he disorder, but no one t r igger has pr oven t o be a cause of prim ar y fibrom yalgia. The et iology and bio pat hophysiological mechanisms of FM S are not com plet ely underst ood st ill. It is a com plex disorder w it h considerable variat ions in clinical sympt oms among patient s. Several mechanisms such as peripheral & cent ral hypersensit ivit y at spinal or brainst em level, brain chemical and hormonal abnormalit ies, muscle abnormalit ies, alt ered pain percept ion and somat osensat ion have been hypot hesised in various studies [3,4]. Treat m ent is usually sympt omat ic because of l ack of u nd er st an di n g o f et i o lo gy an d pat hogenesis. A range of pharmacological and non-pharm acological m anagem ent is usef ul according t o evidence based guidelines and review s.
Exercise programs w ere report ed t o be helpful i n FM S p at i en t s i n sever al st ud i es. Such exercises includes st ret ching, st rengt hening, flexibilit y, aerobic exercises, yoga, tai chi etc..
Pilat es is a part icular exercise approach t hat w as founded by Joseph Pilat es (1880–1967) and w as init ially pract iced by at hlet es and dancers. Pilat es t raining is int ended t o improve general body flexibility and healt h by emphasizing “ core” (t runcal) st rengt h, post ure, and coordinat ion of breat hing w it h movement . Pilat es exercises are designed t o put part icipant s in a posit ion t hat m inim izes unnecessary m uscle recruit m ent , w hich could pot ent ially lead t o early fat igue, decreased stabilit y, and impaired recovery.
ISSN 2321-1822 st at e of parasympat hetic dominance. Sympathe-t ic acSympathe-t iviSympathe-t y decreased afSympathe-t er yoga based guided relaxat ion. Vijayalakshmi et al (2004) st udied t hat aft er 4 w eeks of supervised yoga t raining, t here w as optimizat ion of sympat het ic response and rest orat ion of aut onomic regulat ory reflex mechanisms.
EEG st udies show t hat yoga and m edit at ion pr act ice lead t o increase in alpha r hyt hm , int er-hemispheric coherence & homogeneit y in t he br ain. On t he night follow ing yoga, t he percent age of slow w ave sleep w as significant ly h i gh er, w h er eas t h e p er cen t age of r ap i d eye-m ov em en t sl eep an d t h e n u m b er o f awakenings per hour w ere less. Follow ing t his, t he self rat ing of sleep based on visual analog scales show ed an increase in t he feeling t hat t he sleep w as refreshing, an increase in feeling “ good” in t he morning, an overall increase in sleep durat ion [14].
M ATERIALS AND M ETHODS
Participants: A t ot al of 20 subject s w ho fulfill t he ACR 1990 Crit eria, w ere part icipat ed in t his st udy. Subject s w ere recruited from Dr. D. Y. Pat il Orthopedic depart ment, Physiot herapy OPD. All subject s met t he follow ing inclusion crit eria: (1) Pain >3m ont hs (2) 11 t ender point s out of 18point s over anat om ical sit es (3) Pressure t hreshold <3kg/ cm2 (4) Bot h male and female pat ient s w it hin t he age group of 20-50 years. Subjects w ere excluded w it h follow ing exclusion crit eria: (1) cardiac disease (2) vascular disease (3) spine pat hology (4) joint pat hology. All subject s w ere required t o sign t he w r it t en informed consent document approved by t he et hical committee at Dr. D. Y. Pat il Vidyapeet h, Pimpri, Pune, India.
Study Design: This st udy w as an RCT, w as complet ed in a month period. Recruitment began on 20t h of Sept ember 2012, and t he st udy w as completed by 3rd of November 2012. Tw ent y subjects w ere randomly allocated to t w o groups by t he invest igat or w ho w as involved in dat a collect ion, t r eat m ent im plicat ion, and dat a an al y sis. 26 Fib r o m y al gia sub j ect s w er e t arget ed, out of w hich 20 w ere included for t he st udy purpose. Subject s in group A received Pilat es exercises.
While, subject in group B received Yoga; bot h
t he groups received t his prot ocol for a period of one mont h, w it h a frequency of 6 t imes in a w eek. Baseline assessm ent s w ere done aft er randomizat ion, at t he st art of t he prot ocol 1st day and at t he end of 4 w eeks. For each subject , all assessment sessions w ere performed at t he same t ime of day.
Assessment: VAS (Visual analogue scale), TPI (Tender point index), AS (Algomet ric score), BDI (Beck depression invent ory) and FSS (Fat igue severit y scale) assessed at baseline & at t he end of 4 w eeks.
Rehabilitation programme: The rehabilit at ion program consist ed of 24 sessions, each session w as 1 hour long, 6 t imes w eekly for 4 w eeks. All t reat ment sessions occurred at t he same t ime o f d ay o n t h e sam e 6 day s o f t h e w eek t h ro u gho u t t h e st u dy. In t er v en t i o n w as conduct ed individually and not in a group format. Th e p h ysi cal t her api st w as i n v ol v ed i n p er f o r m i n g t h e i n t er v ent i o n as w el l as conduct ing t he assessment s. Pilat es exercises given t o group A pat ient s. There w ere 10 set s of exercises of w hich few t rial sessions w ere given before st art ing t he t reat ment prot ocol for core muscle act ivat ion. Subjects w ere given w arm up (general mobilit y exercises) for 7-8m in, t hen pilat es exercises w ere given, each for 5 reps and t hen cool dow n (st r et ching exer cises) w ere given for 7-8 min.
Yoga given t o group B pat ient s and t here w ere 10 alt ernat ing supine, prone and sit t ing poses chosen. Subject s w ere given w arm up (general mobilit y exercises) for 7-8min, t hen yoga poses w ere given, each for 5 reps and t hen cool dow n (st ret ching exercises) w ere given for 7-8 min. There is evidence in t he lit erat ure t o support each of t he com ponen t s cont ained in t he intervent ion.
Outcome measures:
V isual Analogue Scale (VAS) [15]: M echanical version of a VAS (a t ool w it h a 10-cm ruler and a m arker t hat t he pat ient m oves t o t he point indicat ing his or her int ensit y of pain) used by pat ient s.
Scoring: 0 = No pain; 10 = Severe pain
ISSN 2321-1822
GROUP A - STOTT’S PILATES EXERCISE
GROUP B - YOGA
Bilat er al leg lift in supine Bridging w it h sw iss ball Neck ext ension w it h fore-arm supp pr one
Heel slides w it h sw iss ball
Shoulder & t r unk r oll w it h sw iss ball
Shoulder & t runk f lexion w it h ball
Alt ernat e arm lift ing w it h sw iss ball
Knee ext ension w it h sw iss b al l
Row ing on sw iss ball Chest hold & arm lift ing in supine
Paschim ot t anasana Yogam udrasana
Dand asan a Bhu jangasana
Naukasana Dh anur asana
Ut t anpadasana Ut t hit hast ha M er udan
d-asan a Set ubandhasana
ISSN 2321-1822 especially face, for response, Use t he follow ing scale t o quant ify each response:
Not painful = 0
Felt painful, no physical response = 1
Felt painful, w ince or w it hdraw al = 2
Felt painful, exaggerat ed w it hdraw al = 3
Area t oo painful t o allow pressure = 4
Add t he t enderness severit ies for all 18 sit es: The sum is t he Tender Point Index (TPI)
The expect ed range for normal cont rols = 0-5
The expect ed range for fibromyalgia = 11-72
Algometric Score (AS) [17]: The foot pad of an algometer is placed vert ically on t he skin of area t o be tested and consistent ly at a rate of 1kg/ sec. The subject is advised t o say “ now ” w hen t he pressure makes t he expected t ransit ion from pressure t o pain. Im mediat ely t he exam iner w it hdraw t he inst rum ent and read from t he gau ge t h e m axim u m am o un t of p r essur e achieved. Each of anat om ical t ender point s should t hen be examined and t he sum of values obt ained from t he 18 ACR Crit eria designat ed t ender point s is divided by 18 t o obt ain AS. AS w ill be inversely proport ional t o t he TPI.
Beck Depression Inventory (BDI) [18]: It is a w idely ut ilized 21-it em self-report scale in bot h clinical and research st udies (Beck et al.,1996).
Int erpret ation of BDI:
1-10 - These ups and dow n ar e consider ed normal
11-16 - mild mood depression
17-20 - borderline clinical depression
21-30 - moderat e depression
31-40 - severe depression
>40 - ext reme depression
Fatigue Severity Scale (FSS) [19]: There are 9 quest ions in FSS. Pat ient s are inst ruct ed t o choose a number from 1 to 7 t hat indicat es t heir degree of agreement wit h each statement where 1 indicat es st rongly disagree and 7, st rongly agree. [ Kr upp et al, Ar ch Neur ol 1989] The scoring is done by calculat ing t he aver age response t o t he quest ions (adding up all t he answ ers and dividing by nine).
Statistical Analysis: Differences in dat a w ere analysed by using Prim er soft w are under t he
supervision of biostat ist ician st aff. For w it hin group im provement in Visual Analogue Scale (VAS), Tender Point Index (TPI), Algomet ric Score (AS), Beck Depression Invent ory (BDI) & Fat igue Severit y Scale (FSS), Paired t -t est w as used.
Bet w een group improvement in Visual Analogue Scale(VAS), Tender Point Index (TPI), Algomet ric Score (AS), Beck Depression Invent ory (BDI) & Fatigue Severity Scale (FSS), Unpaired t -t est w as used.
RESULTS AND TABLES
The finding of present st udy clinically support s our alt ernat ive hypot hesis w hich w as St ot t 's Pilates exercises(Group A) is more effective t han Yoga (Group B) in fibromyalgia pat ient s. Our result reveal significant improvement s in VAS, TPI, AS, BDI & FSS in bot h groups. No significant differences bet w een groups w ere found in VAS, TPI, AS, BDI & FSS. The w it hin group analysis did not support t he bet w een group difference.
Table 1: Pre-t reat m ent dat a for bot h groups.
Group A Group B
M ean SD M ean SD
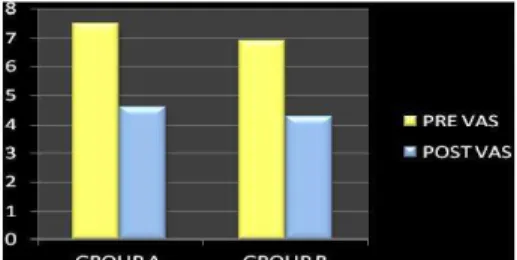
VAS 7.5 0.849 6.9 0.948
TPI 34.7 8.994 29.5 4.483
AS 20.04 2.223 17.37 5.633
BDI 10.4 2.066 12.3 0.7379
FSS 4.718 0.6749 4.14 0.4904
Table 2: Post t reat m ent data for bot h groups. Group A Group B
M ean SD p M ean SD p
VAS 4.6 2.011 0.001 4.3 0.948 0.000
TPI 18.5 5.148 0.000 16.1 4.483 0.000
AS 24.88 6.179 0.058 22.36 5.633 0.000
BDI 6.9 1.197 0.000 6.1 0.7379 0.000
FSS 3.272 0.6158 0.000 2.862 0.4904 0.000
Graphs represent ing dist ribut ion of bet w een group comparison of VAS, TPI, AS, BDI and FSS score respect ively.
ISSN 2321-1822
Graph 2: Pr e an d po st t r eat m en t m ean dif f er en ce com parison of VAS in bot h groups.
Graph 3: Pre and Post t reat m ent com parison of TPI in Group A and B.
Graph 4: Pre And Post Treat m ent M ean Dif ference Com parison Of TPI In Bot h Groups.
Graph 5: Pre and Post t reat m ent com parison of AS in Group A and B.
Graph 6: Pr e an d po st t r eat m en t m ean dif f er en ce com parison of AS in bot h groups.
Graph 7: Pre and Post t reat m ent com parison of BDI in Group A and B
Graph 8: Pr e an d po st t r eat m en t m ean dif f er en ce com parison of BDI in bot h groups.
Graph 9: Pre and Post t reat m ent com parison of FSS in Group A and B.
Graph 10: Pr e and post t r eat m ent m ean dif f er ence com parison of FSS in bot h groups.
DISCUSSION
Our st udy show s t hat bot h t he t reat ment had effect on improving VAS, TPI, AS, BDI & FSS but st at ist ically t here w as no difference exist ed bet w een bot h t he groups at t he end of 4 w eeks.
ISSN 2321-1822
We believe t hat furt her research w it h m ore part icipant s and longer follow up periods could help t o assess t he t herapeut ic value of t hese exercises. The frequency, durat ion of exercises in bot h t he groups can be alt er t o check t he ef fect iveness of t r eat m ent . Ot her out com e measure can be added t o see t he effect on ADL, st rengt h and endurance.
effect of exercise are not clearly underst ood [20]. Alt hough it is a widely accept ed hypot hesis t hat activat ion of the endogenous opioid system during exercise plays a key role in t he analgesic response mechanism, several researchers have also suggest ed a m ult iple analgesic syst em including non opioid mechanisms mediat ed by ot her subst ances such as grow t h hormone and cor t icot rophin [ 20,21]. Analgesic ef f ect of exercise may also help t o break t he vicious cycle of pain-im m obilit y-pain by encouraging t he pat ient s t o part icipat e in t he exercise programs. Exercise m ay also increase t he w ell-being of pat ient s by prevent ing muscular hypoxia w hich is commonly seen in FM S pat ient s [22].
St u dy h as sho w n t h at FM S pat i en t s h av e m uscular asym m et r y and ant algic post ural problems (Jones, et al) show ed t hat FM S may affect peripheral and/ or cent ral mechanisms of post ural cont rol leading t o significant ly impaired balance. The efficacy of Pilat es exercise on fibromyalgia in t his st udy can explain by, Pilates involves close kinet ic chain exercises, w hich provide t he com pressive and decompressive forces necessary t o fost er nut rit ion t o t he joint s and cart ilage t o reduce risk of degenerat ive changes and also helps t o reduce chronic axial musculoskeletal pain [23].
Several Scient ific st udies on yoga demonst rat e t hat yoga im proves dext er it y, st rengt h and m u scu l oskelet al co o rd i n at i o n o f t h e pract it ioners. Post ures assum ed during yoga pract ice are mainly isomet ric exercises w hich provide opt im ally m aint ained st ret ch t o t he muscles. Series of asanas involve assumpt ion of t he pose f ollow ed by count erpose i.e. it involves co-ordinat ed act ion of synergist ic and ant agonist ic muscles w hich brings increased st ead i ness, st ren gt h , st am i na, f l exi b i l it y, endurance, anaerobic pow er, bet t er neuro-muscular coordinat ion and improved ort hostatic t olerance [14].
St udy limit at ion w as t hat it w as conduct ed w it h small size of Fibromyalgia pat ient s, hence t here i s l i m it ed gen er al izab il i t y o f f i n di n gs t o p o pu l at i o n o f peo p le w it h Fi b r om y algi a Syndrome as a w hole. Inst ead of receiving bout of exercises and yoga for a short er period, t hey may need t o cont inue t he programme for several more mont hs for bet t er improvement .
CONCLUSION
Here, it can show ed t hat Stot t 's Pilat es exercises and Yoga bot h are equally effect ive in t reat ing Fibromyalgia pat ient s st at ist ically but , clinically St ot t 's Pilat es exercises (Group A) show ing bet -ter improvement t han Yoga (Group B).
ABBREVIATIONS
FM S - Fibromyalgia Syndrome VAS - Visual Analogue Scale AS - Algomet ric Score TPI - Tender point Index FSS - Fat igue Severit y Scale BDI - Beck Depression Invent ory
ACKNOW LEDGEM ENT
I w ould like t o t hank Principal Dr. Tushar Palekar and my guide Dr. Sent hil K. & all staff of Depart m ent of Physiot herapy, Padm ashree Dr. D. Y. Pat il Vidyapeet h (Pim pri-Pune), subject s of Fibrom yalgia f or support , suggest ion s, co-oper at ion, keeping spir it s high and successf ul at t em pt t hroughout t he st udy.
Ther e w as no f unding pr ovided by any inst it ut e or com panies t o purchase pressure algom et er, for dat a analysis as w ell as t o do various inst ruct or course for t he sam e st udy.
Conflicts of interest: None
REFERENCES
[ 1] . Am er ican Fam ily Physician, Am Fam Physician, 2007, Jul 15; 76(2):247-254.
[2]. Schw einhardt P. Fi bromyalgia: a disorder of t he brain? Neuroscient ist . 2008;14:415-421.
[3]. M yof ascial pain and Fibrom yalgia Syndr om es, A clinical guide t o diagnosis and M anagem ent , Pet er E Baldry, Forew ard by Brian Hazlem an, Chap.16 Clinical charact erist ics and bio pat hophysiological m ech an i sm s o f f i b r o m y al gi a sy n d r o m e , M uham m ad B. Yunus, Fat m a Inanici, 351-371. [4] . Shri K. M ishra, Par am pr eet Singh, St even J. Bunch,
ISSN 2321-1822
[ 16] .Po ll y E. Bi ju r, Phd , Wen dy Si l ver, M a, E. Joh n Gallagher, M D, Reliabilit y of t he Visual Analog Scale f o r m easu r e m en t o f Acu t e Pai n , Acad e m i c Em ergency M edicine, Decem ber 2001;8(12): 1-5. [ 17] . Phi lipp O. Valko, M D; Claudio L. Basset t i, M D;
Konrad E. Bloch, M D; Ulrike Held, PhD; Chr ist ian R. Bau m an n , M D, De p ar t m e n t o f N e u r o l o gy, Pulm onary Division, and Hort on Cent re for Pat ient -Orient ed Research, Universit y Hospit al of Zurich, Zur ich, Sw i t zer l an d, Val id at io n o f t h e Fat i gu e Sever i t y Scale i n a Sw i ss Co ho r t ,SLEEP, , Ju ne 2008;31(11).
[18]. Donald D. Price, Pat r icia A. M cGrat h, Am ir Rafii and Barbara Buckingham , The Validat ion of Visual An al o gue Scal es as Rat i o Scal e M easur es f o r Chr onic and Exper im ent al Pain, Pain, 1983;17:45-56.
[19]. Dozois, David J. A.; Dobson, Keit h S.; Ahnberg, Jam ie L , A p sych o m e t r i c e v al u at i o n o f t h e Beck Depression Invent ory–II, Psychological Assessm ent , June 1998;10(2):83-89.
[20]. Ram say C, M oreland J, Ho M , Joyce S, Walker S, Pu l l ar T. An o b ser ver -b l i n d ed co m p ar i so n o f su per vised an d un sup er vi sed aer obic exer ci se regim ens in fibrom yalgia. Rheum at ology 2000;39: 501-5.
[21]. Kjaer M . Regulat ion of horm onal and m et abolic responses during exercise in hum ans. Exerc Sport Sci Rev 1992;20:161-84.
[22]. Kolt yn KF. Analgesia follow ing exercise. A review. Sport s M ed 2000;29:85-98.
[23]. Lale At lan, M D, Nim et Koekm ez, PhD, Eff ect s of p i l at es t r ai n i n g o n p r o p l e w i t h f i b r o m y al gi a syndrom e, Arch Phys M ed Rehabil 2009;90:1983-8.
[5] . Shridharan K, Pat il SK, Kum aria M L, Selvam ur t hy W, Joseph NT, Nayar HS, et al. St ud y o f so m e p h ysi o l o gi cal an d b i och em i cal p ar am et er s i n subject s undergoing yogic t raining. Indian J M ed Res. 1981;74:120–4. [PubM ed]
[6] . Field T. Yoga clinical research review. Com plem ent Ther Clin. 2011;Pract 17:1-8.
[7] . Innes KE, Bourguignon C, Taylor AG. Risk indices associat ed w it h t he insulin resist ance syndrom e, car diovascular disease, and possible pr ot ect ion w it h yoga: A syst em at ic review. J Am Board Fam Pract . 2005;18:491-519.
[8]. Vera FM , M anzaneque JM , M aldonado EF, Carranque GA, Rodr iguez FM , et al. Subject ive sleep qualit y an d h o r m o n al m o du l at i o n in l on g-t er m yo ga pr act it ioners. BiolPsychol. 2009;81:164-168. [ 9 ] . Br o t t o LA, M eh ak L, Ki t C. Yo ga an d sexu al
f u n ct i o n i n g: A r ev i e w. J Sex M ar i t al Th er. 2009;35:378-390.
[10]. Abeles M , Solit ar BM , Pillinger M H, Abeles AM . Up d at e o n f i b r o m yal gi a t h e r ap y. Am J M ed . 2008;121:555-561.
[11]. Harris RE, Clauw DJ, Scot t DJ, M cLean SA, Gracely RH, Zubiet a JK. Decreased central u-opioid recept or avai l ab i l i t y i n f i b r o m y al gi a. J N e u r o sci . 2007;27:10000-10006.
[12]. Sengupta P. Healt h im pacts of yoga and pranayama: A state-of-t he-art review. Int J Prev M ed. 2012;3:444-458.
[13]. Kinser PA, Goehler LE, Taylor AG. How m ight yoga help depr ession? A neurobiological per spect ive. Explore (NY) 2012;8: 118-126.
[14]. Dr M adanm ohan M D, Ef fect Of Yogic Pract ices On Dif ferent Syst em s Of Hum an Body, Depar t m ent of Physiology & Program m e Direct or, ACYTER, JIPM ER, Pg No 1-14.
[15]. M uscle Pain, Underst anding it s nat ure, Diagnosis and Treat m ent , Siegfried M ense, David G. Sim ons, I.Jon Russell, Chap 9, Fibr om yalgia Syn dr om e, Pg.No. 289-337.