4_x_
the
ORGANIZATION
PAN
HEALTH
di
r
ecting
AMERIcAN
c°uncil
ORGANIZATION
the regionalwoRLDcommitte__l__,__
HEALTH __
f
'
68th Meeting
Washington, D. C. July 1972
I Provisional A_enda Item 18 CE68/14 (Eng.) 7 June1972
ORIGINAL: ENGLISH-SPANISH
STRENGTHENING OF LABORATORY SERVICES. STUDY OF THE USE OF "AUTOANALYZERS"
PRELIMINARY REPORT ON THE USE OF AUTOMATED EQUIPMENT IN DIAGNOSTIC LABORATORIES
% Background
At the 13th Plenary Session of the 66th Meeting of the Executive
&
Committee of the Pan American Health Organization, Resolution VI was adopted, operative paragraphs 3, 4, and 5 of which read as follows:
To recommend to the Director that, subject to the avail-ability of budgetary funds, he undertake a study on the
use-fulness of autoanalyzers in national diagnostic laboratories. That study will include information on the type and capacity of this equipment, and advantages to be obtained from its use.
To request the Director to deal in the study with the problems involved in the maintenance of laboratory equipment.
To request the Director to report in due course to the Executive Committee the findings of the above-mentioned study.
In compliance with this resolution, a preliminary study was made covering the following aspects in particular:
1. Analysis of available information.
2. Survey of experience with the use of automated equipment in various laboratories in Latin American countries.
The study was made by a working group composed of two specialists and PAHO/WHO personnel.
An analysis was also made of the levels of the clinical laboratories in which automation is advisable. The corresponding document appears as the Annex.
' Because of the limited funds available, the scope of the study was necessarily limited.
. The results may be summarized as follows:
1. Automated Equipment Available
numerous models of each. As a rule, the price of this equipment is between US$5,000 and $100,000, depending on the capacity of the apparatus and its make. The models available range from the single channel autoanalyzer, which is the most commonly available, to highly complicated models equipped with computer systems and capable of making from 2 to 24 tests on a single
specimen. The operational capacities of these apparatus range from 30 to 60 examinations an hour, with a theoretical capacity of 1,200 laboratory
resultsperhour.
There are other more complicated apparatus, some of which can be programmed (i.e. the tests may be selected) or which can make preselected programs of from 10 to 20 tests on each specimen. There is a 24 channel apparatus with a selection capacity of 3,000 tests per hour. Its price is approximately US$500,000.
A list of most of the apparatus on the market, together with their most important features, appears as tables III and IV of the Annex.
2. Advantages and Problems of Automation
The automation of clinical laboratories may render significant bene-fits, foremost among which are improvement in the quality of results, re-duction of working time, increase in the capacity of the laboratory to carry out a greater number of analyses, reduction in operating costs, and limita-tion of the vulnerability of laboratory operations attributable to human error.
The experience gained in the last two decades shows that without a sound justification, and without the necessary precautions being taken, the automation of laboratories may be counterproductive and create more and more serious problems than already exist. In addition, it involves a siz-able investment, which may be ineffective because of the underutilization of apparatus. This may be due to the small demand for examinations or the
frequent breakdowns of the equipment resulting from poor handling and/or lack of maintenance. The investment also runs the risk of losing its value because of the rapid obsolescence of the equipment, more advanced models of which are frequently introduced.
Furthermore, the purchase of automated equipment entails the replace-ment of existing apparatus, which is not always advisable or necessary and results in financial losses.
The value of the investment and its implications are of even greater importance if it is borne in mind that the availability of resources is always a limiting factor on the operation of laboratories.
Page 3
it is necessary to gain more knowledge of the advantages and problems as-sociated with the use of this equipment, and it is advisable to establish criteria for guiding or influencing this process.
· The purchase of automated equipment is a decision that must be based on a careful study of the situation in each particular laboratory. The study should cover such factors as clear definition of the functions as-. signed to the laboratory; type of demand for examinations and their volume
(actual and anticipated); possibility of satisfying that demand by better use of available resources, without the quality of results being thereby affected; present cost of the unit; available facilities for the operation, maintenance, and repair of automated equipment, depending on its require-ments; possibility of reusing the resources that will be displaced; finan-cial capacity for purchasing and maintaining the new equipment; and the benefits it is hoped to obtain with the change, and so on.
In the second place, an overall comparison should be made of the laboratory concerned with the characteristics of the automated equipment to be purchased, especially its capacity, price, and ease of operation and repair. It is often thought that one or two channel machines are the most advisable when laboratory automation is initiated. These models are
ideal because their construction is based on modules or interchangeable basic parts which function as a system, and because of the flexibility this module assembly provides.
3. Availability and Use of Autoanalyzers in Latin America
Preliminary to the study, a list was drawn up of the countries and institutions currently using autoanalyzers. This information was obtained from the manufacturers of the equipment, their representatives in the coun-tries, PASB personnel, and other sources.
The following table shows the approximate number of autoanalyzers in use in Central and South America, including all types of laboratories.
Country or Zone No. of Apparatus No. of Channels
Argentina 70 i - 12
Brazil 60 1 - 12
Chile 4 4 - 6
Colombia 3 1 - 2
- CostaRica,Honduras,Guatemala 5 1 - 2
Mexico 65 1 - 12
Panama 5 1 - 2
Peru 6 1 - 18
Venezuela 25 1 - 12
It is estimated that the 243 autoanalyzers in the Americas represent a cost of about US$5,000,000.
To obtain information about the use of existing automated equipment, a sample survey covering 31 laboratories in the above-mentioned countries was made.
It was based on a questionnaire designed to identify the main features of the use of the equipment such as: (1) available resources and their
corre-sponding use; (2) trend in the demand for examinations in the last six years; (3) daily number and type of analyses; (4) model and characteristics of the automated equipment available; (5) rank of the personnel responsible for operating it, and type of training they received; and (6) problems connected with the operation, maintenance and repair of this equipment.
The 31 selected laboratories were visited. Only 16 of them returned the additional questionnaires in time for the data they contained to be
included in the present study.
The following table shows the distribution of these laboratories by country.
Country No. of Laboratories No. of Apparatus
Argentina 2 2
Chile 3 4
Colombia 4 5
Panama 3 5
Peru i 3
Venezuela 3 6
Total 16 25
This information covers 25 apparatus of which 23 are for clinical chemistry and two for hematology.
If the extent of the problem in Latin America is taken into account, it is obvious that the sample studied needs to be enlarged in future studies. Despite this limitation, this first attempt gives some general orientation
on the subject.
Automated apparatus were first introduced into Latin America in 1962. The number of apparatus purchased has gradually increased in recent years,
Page 5
FIGURE 1
DISTRIBUTION OF AUTOMATED EQUIPMENT PURCHASED, 1962-71
· 6O
54.2%
45
33.3%
30
15 12.5%
1962 1966 1969
1965 1968 1971
Year
In most cases, the decision to use automation was taken without a previous feasibility study, and there is little evidence that the decision was taken in the light of the volume of demand or for logistic reasons, or
to reduce operating costs.
· Apparatus in present use reach, on the average, 40% of their effec-tive capacity in a period of eight hours of work.
Difficulties arise in obtaining the solutions used in the tests, both for the laboratories that prepare them (65%) and for those which combine production with import and/or local purchase (35%). The most _idespread problems are the shortage of reagents or raw materials for preparing them,
excessive delays in supply, and limited choice as to quality.
With regard to maintenance and repair of equipment, the shortage of spare parts and of suitable technical personnel, as well as delay in provid-ing the necessary services, was mentioned.
4. Discussion
The study made was a preliminary one and dealt generally with the principal aspects of the use of autoanalyzers in diagnostic laboratories.
The information obtained suggests that it is necessary to expand these studies and to undertake other more specific studies designed to ascertain the results obtained and the cost-benefit ratio in laboratories and/or health programs.
The first fact to be emphasized in this study is the accelerating spread of these apparatus in diagnostic laboratories, despite their high cost. This is understandable since autoanalyzers represent a technological advance that has obvious advantages for laboratories. These apparatus are capable of processing automatically a large number of specimens per unit of time, which makes for a more rapid, possibly cheaper service, and increases the operating capacity of the laboratory. Because of its mode of operation, automated equipment reduces the vulnerability attributable to human error, and can thus improve the quality of the examination results.
However, the experience of more than two decades indicates that pru-dence is necessary in automating laboratories, since a premature decision generally results in more harm than good.
Although covering only a small number of laboratories, the survey shows that there are a number of problems involved in the maintenance and repair of the equipment; the supply of reagents, drugs, and spare parts; and personnel training. In addition it indicates underutilization of the
capacity of the equipment already available.
In order to improve the situation in laboratories it is generally necessary to try to solve their problems through the maximum utilization of
Page 7
In the light of the information available, the group proposes:
That the study on the use of autoanalyzers be continued and expanded;
That the data contained in this preliminary study be sent to the countries, together with such new information as is obtained, so that their authorities may be in a better position to take a decision on the use of autoanalyzers; and
That the countries be requested to inform the Organization of the problems they encounter in operating automated equipment in their diagnostic laboratories.
AUTOMATION IN THE CLINICAL LABORATORY
Review of the Information Available
by
Dr. Ronald Laessig State Laboratory of Hygiene
University of Wisconsin
ANNEX
Automation is a technique in which the processing, apparatus, or system is controlled by mechanical or electronic devices designed for the purpose of replacing human organs of observation, processing, or decision.
Automation in the clinical laboratory involves the integration of devices into the laboratory operation, where, along with the human techni-· clans, they contribute to the precision, accuracy, productivity and/or
effectiveness of the total operation. Their introduction is intended to make a significant improvement in at least one of the four above through a - process whereby human activities are modified. In a sense, expansion of
clinical laboratory automation involves considerations uniformly applicable to the most elementary as well as the most sophisticated laboratory.
To facilitate discussion of introduction and expansion of automation and its impact on the laboratory operation, we will define developmental status levels (five of them) which are based on the laboratory's capabil-ities as well as its mission. It should be emphasized that all laboratories contain elements of at least two adjacent levels. Therefore, a key concept in programming the development of the laboratory to higher levels of sophis-tication in terms of kinds, number, and quality of tests is the realization that growth must involve an orderly progression through, as well as reten-tion of capabilities at all levels. This plan is essential to a well con-ceived and developed laboratory. Specifically, quantum (step) jumps over levels is not in the best interests of the laboratory, the physician using it, or the patient requiring its services.
PROGRESS
I
ON
OFAUTOMATION
I
N CL
I
NICAL
L
ABORATOR
I
ES
J
)-kJ
Z
ILl
0
LLI LI_
D
EVELOP
I
N
COUNTRY
G
1
2
3
4
I
N
CRE
A
SED AUTOMAT
IO
N
O
F THE
L
AB
O
RA
TO
R
Y
,m,.--
ANNEX Page 3
THE BASIC LABORATORY (Level I)
1. Description: This laboratory provides only the most basic kinds of , services and is limited to a relatively few (four or five) kinds of tests. It is often included in a doctor's office or in a very small clinic. The services are provided in close association with the physician practicing medicine - often by the physician himself, his nurse, or his secretary. Near the upper end of this level, a technician, usually a high school grad-uate, may be employed and work under the nurse. Tests include hemoglobin, urine (usually dipstick), basic chemistries (usually glucose and BUN), and sometimes blood or urine microscopic examinations. Equipment is the most basic and is often the greatest source of trouble. The color reading device is most often a colorimeter giving very low specificity for the test involved. Laboratory glassware is minimal, often making poor substitutions (eyedrop-pers for pipettes and graduated pipettes for volumetric ones), with little volumetric equipment and with poor control over analytical variables, such as time and temperature of reactions. Personne_other than the physician and his nurse, are poorly trained, usually obtaining their training from
the physician himself or from a salesman for the equipment. These personnel are usually high school graduates with no formal training. Typically, l0 to
30 tests are performed per day.
2. Problems: The most significant problem is the poor quality of re-sults. This is due to poor equipment, poor reagents and chemicals, poor training, and poor supervision. The technician likewise has little or no capability to help herself or little idea where to seek help. The second problem is that the equipment is not adequate to the task at hand, poor
techniques of operation are used, and/or maintenance is not performing up to capabilities. A third problem lies in the area of the technician being faced with a large number of different procedures for which she cannot main-tain organization or transfer knowledge. A fourth problem centers about the laboratory and the ability of the staff at all levels to understand problems of quality assurance, or, if the need for them is understood, what to do about meeting them.
3. Suggested Solutions for Laboratories within this Level: Quality of results can be improved by use of prepackaged, single-use, disposable test systems. The problems of making, maintaining, and correctly using(includ-ing dispensin_ reagents and chemicals, can be offset through these proce-dures. The initial cost per test is quite high, but is justified by the quality of results and in many cases is offset by the reduction of overhead. Typically these "kits" contain vials with predispensed reagents which have
The prepackaged concept can help the technician perform a wider va-riety of test procedures. However, despite claims of the manufacturer to the contrary, single technicians at this level should not be required to perform more than four or five different tests (hemaglobin, glucose, BUN, dipstick, and microscopic, for example). This kind of laboratory can sup-port the physician at a fundamental level. If the doctor feels that he would like the variety of more complex tests, but still for one or two-man patient loads, he would be advised to increase the quality of technician to one who, with some understanding of the methods, can cope with the va-riety of procedures.
Quality assurance is most difficult at this level. The tests re-quired to control quality cost a good deal of money and must be absorbed
into the laboratory overhead. Even when the physician (laboratory director) "buys" this concept, organization of the program of quality control remains a significant problem. This problem is one which requires governmental
as-sistance and/or action. In the United States of America voluntary and man-datory action has been quite successful in this respect. A most useful approach would be to have some organization provide guidelines and recommen-dations along this very basic line through the medical profession itself. Some form of local, personal help is likewise required. It can be provided through medical technologist (bachelor's level) personnel with special training. In the United States the level of laboratory and quality control remains our most significant problem. Training manuals and programmed in-structional self-help programs would prove most useful once the interest of the physician operating the laboratory is obtained.
3.1 For progression to other levels the laboratory at this level must develop a sound basic capability in the tests performed. No consideration of expansion, i.e., providing 50-60 tests for three or four doctors, should be considered until this is accomplished. When loads are going to increase, additional instrumentation, preferably of the same type as already in use,
should be considered to provide back-up capability. In addition, upgrading of personnel with the increase in the numbers of tests should be of primary consideration. Expansion to the next level of laboratory is greatly depen-dent on having back-up personnel available, since the increased complexity and types of tests preclude the physician or any one else from "stepping ' into" the laboratory and doing the tests in an emergency. Consequently,
any thoughts of progression to Level II must include development of back-up capabilities in personnel as well.
The recommendations both for duplicate (back-up) instrumentation and for personnel are based on the assumption that criteria of adequate train-ing, suitable kit procedures, and quality assurance have been met.
ANNEX Page 5
high cost can be justified also on the basis of reduced overhead (efficient use of reagents and no lost time in preparation). The basic specialized meter (see Table I) is of relatively low cost. This type of laboratory will be heard from in increasing numbers. The economic advantages to the physi-cian are apparent and are the main reason for their growth and development.
4. Tabular Summary - Basic Level Laboratories: Table I-a describes pre-packaged and preprepared reagent systems. The first entries (1-6) are the totally prepackaged reagents, providing one test per vial. The tests include
the basice glucose, BUN, uric acid, and hemoglobin most typical of labora-tories at this level. In addition, other chemistries are available, usually eight to ten additional tests such as cholesterol, total protein, albumin, and chloride. The first mentioned are most relevant to this level. The basic "meter" for these instruments consists of a cuvet well designed to accept the tubes in which the reagent is packaged and a dial calibrated
di-rectly in concentration units (i.e., gm Hb/100 ml). The good kits supply a standard to check the calibration of the meter as a part of the analysis. The need to produce calibration curves and to check meter operating para-meters required with a spectrophotometer is eliminated.
The Dow system, No. 1, is probably the best of the systems; the Bio-dynamics, No. 3, is definitely counterindicated.
The second part of Table I-a describes bulk reagents which are essen-tially the same in concept but require the laboratory to dispense them into cuvets. In this case the basic meter or a spectrophotometer can be used for readout. With advanced personnel, i.e., nearing the end of this level, a switch to bulk reagents for the high volume tests will significantly reduce costs (to about $0.03 per test). For most laboratories, at volumes of up to 30 tests per day, this is not recommended. Items 7-11 are very much the same and when used with care will give good results.
Table 1-b describes filter photometers and Table I-c, spectrophotom-eters. The filter photometer or colorimeter is not recommended, since with little additional cost a much better spectrophotometer could be purchased. Purchase of an instrument of this type is dominant to a decision to move to Level II and to the development of extensive bulk reagent capabilities. For most laboratories at Level I, the attractive pricing of bulk reagents should
not be used as justification to precipitate this decision, as the technicians are not capable of working with the instrument and have additional opportun-ities for trouble.
PREPACKAGED, PREPARED REAGENT SYSTEMS, CHEMISTRY TESTS 1
No. Name Readout Comments/Cost
1. Dow "Diagnostest" (Direct Reading) Meter Self-contained, totally disposable system. Good quality,
supplied no glasswarerequired. About $600
2. Clay-Adams "Accustat" (Direct Reading) Meter Self-contained, disposable. Meter has unique code system supplied to assure correct units, calibration. $600
3. Biodynamics "Unimeter" (Direct Reading) Meter Self-contained, no wave-length selection, results poor
supplied quality. About$300
4. Ames/BMI "Blood Analyzer" (Direct Reading) Meter Self-contained, disposable based system. Good quality.
supplied About$500
5. Smith-Kline "Eskalab" Meter Very high quality, totally disposable. Requires high supplied degree of technical skill. Not recommended at basic
level because of complexity. About $2,800
6. Sarasonic Meter Prepackaged, disposable systems. Little known about supplied evaluation. Comment withheld.
7. Harleco Reagents None use Bulk reagents for most chemical tests. Costs are low, spectro- require manipulation, dispensing, or pipetting.
photometer
8. Hycel Reagents None use Bulk reagents, as above. Best known and oldest US supplier spectro- in field. Good quality; written directions are excellent photometer and an asset to laboratory.
9. Hyland Reagents None use Bulk reagents and reagent test kits. Quality is good; spectro- requires more manipulative skill than 8 and 9 above. photometer
10. StanBio Reagents None use Bulk reagents similar to Hycel's and of acceptable quality.
spectro-photometer
11. Dow Reagents None use Bulk reagents similar to methods in 1 above· Quality on spectro- par with 7-10 above.
photometer
Note two classes: bulk and individual test reagents. Bulk reagents require the true laboratory; entries 1-6 have na_ 1
No. Name Type Comments/Cost
12o Photelometer,C5A Filter Battery type, 390-645 nm, very low cost. $ 80
13. Cento Sheard B2 Filter Suitable for ASTM where filter is accepted, 380-700. $195
14. ColemanModel 8 Filter Very low cost, 390-655,good reputation. $250
15o Evelyn 4600 Filter Good quality,widely used system,350-840 nm. $995
16. Fisher, Electrophotometer II Filter Acceptable, accesBories available, 400-720. $385
17o Instra Tech, T/600 Filter Very low cost, 350-660. $ 70
18. Leitz, Mod M Filter Best known for 25 years; first choice if filter is
used; 415-700(limitedrange). $381
19. Photovolt, 40lA Filter Dual filters, good quality, 420-650 and 400-900. $310
20° Photovolt, 402E Filter Dual, extended-range version, only double-beam filter
instrument,390-730 and 400-900. $650
1Colorimeters are inherently simpler instruments when compared to spectrophotometers. With the advance of instrumental development, many of their advantages, particularly reliability, have been negated. Unless funds are restricted or personnel are of the lowest level, their purchase would be hard to justifiy.
_ F_oo
SPECTROPHOTOMETERS FOR THE BASIC LABORATORY 1
No. Name Type Comments/Cost
21. B & L Spectronic20 Grating Quality low cost instrument,340-950 $395
22. B & L Spectronic 70 Grating Accepts wide variety of cuvets, cells, best choice for
money of B & L series, 325-925 range is excellent. $685
23. B & L Spectronic 88 Grating Variety of readout capabilities make it superior to 70
for advancinglaboratory. $995
24. Coleman, Models 6A and 6C JRs Grating Wide variety of cuvets and accessories. Range 400-700
generally suitable for most lab work except enzymes. $322
25. Coleman Model 14 Grating Best known laboratory instrument. Highly reliable and rugged. Range 325-825 nm. Widely used with little
dolltime $820
26. Gilford 300N Grating 340-700. High quality instrument with numerical readout. Uses aspiration system. Too elegant for labs at this
level. $2,200
27. Unicam SP 600 Prism 335-1000 nm instrument. Good quality for money, adapts
to variety of test tubes and cuvets. $900
28. Rudolph MSP7 200-700. Single beam instrument,capable of reading on very small samples. Probably unwarranted at this
levelof laboratory. $2,450
29. Turner 330 Grating Small instrument, very simple to operate, and high quality for market. Designed for easy service and a
goodchoice. $595
SEMI-AUTOMATED LABORATORY (Level II)
1. Description: This laboratory performs a wider variety of chemical tests than the basic laboratory of Level I. In addition, it utilizes some different kinds of equipment to speed processing and give it the expanded capabilities. The purchase of this additional equipment and the implemen-tation of new procedures into the basic laboratory, a process often known as automating the laboratory, can assist it in evolving into Level II or
semiautomated status. The equipment is designed to eliminate hand process-ing and to speed and improve the analyses. The underlying objective, of which one often loses sight - improvement of results - must be the
motivat-ing factor. For this reason, the recommendations for automation are de-signed to bear directly on the major sources of error inherent in operation at this level.
Personnel at this level have some specialized training, usually vocational (two years after high school), or college training as medical technologists. Personnel in the laboratory are assigned to its exclusive operation, but often are required to cover three specialties (chemistry,
urinanalysis, hematology, and sometimes X-ray).
The laboratory's mission is to provide a relatively large number of determinations (usually 10 to 12) and a larger volume of tests (30 to 100 per day) and to serve the needs of several (up to 6 or 8) other laborato-ries directly or on a service laboratory basis.
Equipment is designed to reduce costs, to process tests in bulk or groups, and to serve a variety of purposes. Typically, this laboratory should have some sort of wave-length selective readout device (spectropho-tometer) and device for hematocrit determination.
2. Problems: The laboratory at this level is often unable to achieve the levels of accuracy and precision required of good work. The wide va-riety of tests and procedures expected of the laboratory require a large stock of chemicals and reagents as well as tests and procedures to be mas-tered. These reagents are difficult to prepare with precision, and results suffer from lack of uniformity of technique and chemical reagent alike.
Personnel at this level have a complex and new set of responsibil-ities thrust upon them. Their main concern is to make the laboratory and equipment flexible to meet changing needs of the different tests. The pro-blem of organization of the operation is also present at the upper extreme of this level where the laboratory must try to respond to larger numbers of requests.
The laboratory lacks the means of assessing its own performance
ANNEX Page 11
3. Suggested Solutions for Laboratories within this Level: Generally, it is assumed that if Level I capabilities are available they should be retained. They provide the laboratory with a valuable back-up capability,
q
a check on performance, and a means of providing "stat" tests.
Two major recommendations relate to the first problem. First, the ' laboratory should purchase bulk reagents (Table I-a) for all of its work.
Production of reagents on the site is definitely counterindicated. The cost of such reagents is very low, and the quality, as well as the value of well
established expiration dates, cannot be overestimated. Personnel in the laboratories are now equipped or interested in production of such reagents. Secondly, the use of automatic dispensers and/or diluters (Table II-a) will greatly speed the operation of the laboratory and streamline its operation. This will eliminate the errors of sample and reagent volume dispensing and
increase precision. The logical addition of these devices to the laboratory, assigning one to each test reagent, assists the laboratory in a logical de-velopmental sequence.
Personnel are required to perform a variety of duties. The high school technician cannot cope at this level but must be replaced by a med-ical technologist or other individual with specialized training. It is essential that personnel be capable of understanding the working of the instruments, particularly spectrophotometers, used in the testing. Further, the laboratory must now realize that it must work with and establish cal-ibration curves for its instrumentation, and regularly check on its perfor-mance. A good quality spectrophotometer is essential to this laboratory
level. Without it, no work beyond Level I should be attempted.
A quality control program must be an integral part of the laborato-ry's operation. It should include checking on the test results with a con-trol serum in every batch of analyses and it should be extended to checks on the instrumentation in use, including wave-length and response of spectro-photometers, and regular maintainance for all instruments. Diluter-pipetter instruments, should be checked regularly for accuracy and reproductability. Quality control of test results should include both an internal program and an external evaluation. The personnel should be indoctrinated in adequate record keeping for this purpose.
3.1 For Progression to Level III (Semiautomated Status): The major improvement in this level of laboratory must come in the area of enzymatic testing. The basic and Level II spectrophotometric measurement devices are not suitable for quality work in this area. Table II-b lists several which are suitable for this purpose. Again we recommend kits for the enzy-matic determinations since the preparation of reagents for these kinds of
tests is too complex for all but the most advanced laboratories.
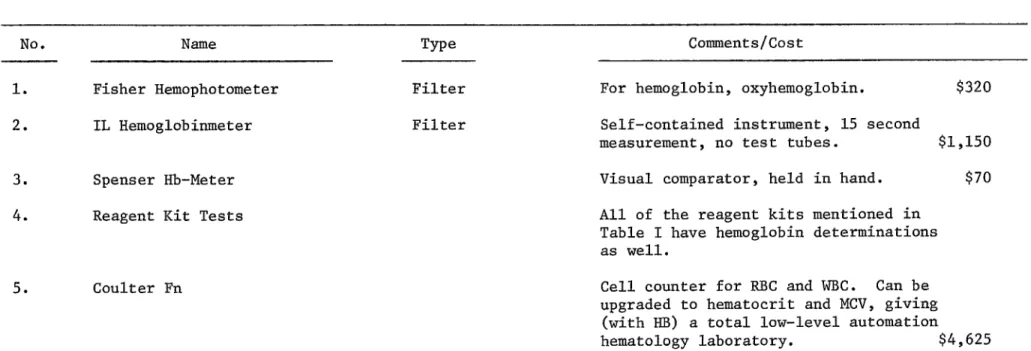
Additional recommendations lie in the area of purchase of special instruments for single tests, i.e., hemoglobin. Several instruments are listed for this purpose in Table II-b. Included is an automated cell coun-ter, the Coulter, for the hematology section. These single-purpose instru-ments speed processing and represent the best type of automation for
laboratories at Level II. A second kind of special instrument is the clin-ical flame photometer described in Table II-e. The main thrust of automa-tion recommendations for this level of laboratory, then, is in the area of purchase of such special purpose instruments as individual tests and work-load warrant.
4. Tabular Summary - Level II Laboratories: Table II-a describes di-luter and pipetter systems which can be used to dispense and store bulk reagents. In many cases the types which sample and dilute are excellent
choices because they eliminate the hand pipetting of reagents. The sample step is critical; the viscous nature of the serum and whole blood samples makes this a difficult requirement. The Oxford diluter is the best choice
for minimum cost. It is all glass and effectively stores and dispenses reagents. Laboratory Industries has an all-glass system for storage and dispensing as well as for sampling; it is manually operated but quite fra-gile. Choices 5, 6, and 7 are motor-driven systems which take care of both phases. Generally, highly corrosive reagents are not recommended. Dedica-tion of one of these to the most active (high volume) tests represents a good investment for the laboratory. Changeover is not recommended. A di-luter for the flame photometer system is essential and should be considered a part of this instrument purchase.
Table II-b describes special hemoglobin meters. As the workload in-creases, the laboratory will find that dedication of an instrument to this area speeds processing and increases accuracy. Hemoglobin determinations are usually left to the blood-drawing technician; hence, the reduction of error possibilities will result in an improvement in the laboratory
performance.
ANNEX Page 13
such as 2, 3 or 6 is an excellent choice, assuming that the laboratory has previously purchased a general purpose instrument. No. 8, Photovolt ERA I, is a unique instrument, making a rate measurement. It is new on the market but will possibly make a major contribution to the field.
· Table II-d lists enzymatic kits. Almost all of these are excellent. The author recommends the Worthington or Boerringer as first choice, but with Sigma and Calbiochem as excellent alternates. Key criteria involve . single-test vials, reaction in the test vials measurement at 340 - rate
preferable, and low cost.
Table II-e is a list of flame photometers. The criteria include internal standard, automated K and Na measurement, and the ability to make lithium determinations on the instrument. The Instrumental Lab Model 143
No. Name Manual Comments/Cost
1. Oxford Dispensors, Model A Yes Dispensor fits standard glass jar. Ideal for rea-gents with bulk tests. Requires minimum prime.
Volume 0-20 mis, adjustable. $65
2. Lab Industries Yes Ail glass, both samples and dilutes (dispenses). Wide ranges. If used with reagents, could be used to sample and dispense reagents_ Very high
precision,adjustable. $95
3. Hycel Dispensors Yes Ail glass with reservoirs. Suitable for one rea-gent. Volumesare fixed. $55
(This item may be replaced in near future)
4. Dade Diluter Motor Includesboth sample aspiration and dispensing driven with significant dilution. Low cost and high
precision for price, lacks high flexibility. $300 5. S/P Auto Diluter Motor Dial settable. Dilutes and dispenses.
driven Muchlike4. $320
6. Warner Chilcott Auto Spensor Motor Dual syringe-type mechanism, uses teflon coil to
driven minimizecontamination. $300
7. Fiser 240 Auto Diluter Motor Uses dual syringes and ail glass system. driven Variety of ranges depending on syringe size.
Very precisesystem. $350
8. General Diagnostics Compu-Pet Motor New item, push-button volume selection which both driven samples and dilutes (dispenses). High precision
and accuracy claimed. Very elegant equipment. $850
Reference: Lab. Management, Dec° 71, pp. 61-62, lists approximately 35 similar systems.
Note: There are many of these devices. Essentially they eliminate pipetting reagent, sample, or in some cases both.
We are listing some of the more common ones, and approximate costs. Real automation is achieved as costs and workload warrantdedication of one of these instruments to storing and dispensing one reagent for a single test.
.1>-TABLE II-b
SPECIAL INSTRUMENTS FOR HEMOGLOBIN DETERMINATIONS
No. Name Type Comments/Cost
1. Fisher Hemophotometer Filter For hemoglobin,oxyhemoglobin. $320
2. IL Hemoglobinmeter Filter Self-containedinstrument, 15 second
measurement, no test tubes. $1,150
3. SpenserHb-Meter Visual comparator,held in hand. $70
4. ReagentKit Tests All of the reagentkits mentionedin Table I have hemoglobin determinations as well.
5. CoulterFn Cellcounterfor RBC and WBC. Can be upgraded to hematocrit and MCV, giving (with HB) a total low-level automation
hematology laboratory. $4,625
_ _oo
t_
No. Name Type Comments/Cost
1. Gilford 300 N Grating Standard spectrophotometerwith flow-throughcell, electronic temp. control. Expandable to variety
of accessories. Base price $2,200 System prices (approx.) $4,700
2. BMG Telco-Meter Fixed Two grating instruments,with temperaturecon-wave-length trol (366 nm) with digital readout and recorder
hook-up, specifically for enzymes only $525-$625
3t Calbiochem, 85070, Spectro Fixed Temp. controlled with recorder accessories,
wave-length 340 nm, again specifically for enzymes $395
4. Coleman Model 101 Variable Temp control as accessory, basic instrument ex-grating tends to UV, suitable for enzymatic
determina-tions. Base price (accessories extra) $1,510
5. Coleman Model 111 Variable Slightly improved version, reaching 190 nm.
grating Base price of instrument (accessories extra) $2,800
6. Golden Enzymetron Fixed For NAD dependentenzyme systems only.
wave-length Temp. control not specified, questionable. $395
7. Unicam SP 500 Prism Basic instrumentwith kinetic accessories,down
to 180 nm. Base price (accessories extra) $2,900
8. Photovolt,ERA I Fixed Enzyme specific instrumentwith printer which makes only kinetic measurements. Temperature
control available, direct reading. Approx. $3,000
9. Spectronic 700 Variable Recorder attachmentsand scale suppression available giving instrument capabilities as enzyme system. Range down to 200 nm.
Acces-soriesextra. $2,040
KITS SUITABLE FOR ENZYMATIC DETERMINATIONS IN THE LABORATORY
No. Name Type Comments
1. Harleco Color Generalkits, no specificinstrumentsupplied. 2. Hycel Color Generalkits, standardenzymes (SGO,SGP, LDH, AP).
Simple to use.
3. Hyland Color/ General kits, some exotic. Require more technical UV skill than above listed.
4. Sigma Color/ Variety of kits, including advanced tests. UV Requires care in use.
5. Worthington Biochemical Corp. UV Variety of tests, including advanced. Good packaging techniques, relatively easy to use.
6. Ames Company Color Standardkits, easy to use, standardonly.
7. Boehringer Mannheim Corp. UV Special instrument available. Highest quality tests with own instrument. Expensive but good, standard, and advanced.
8. Calbiochem UV Also have own instrument. Good qualityand good reputation. Standard and advanced tests.
9. Dade Color Standardtestsonly, simpleto use. No instrument supplied.
10. Dow Color Prepackagedsingle test system,uses the Dow instrument or colorimeter. Very simple to use. For single tests, relatively high cost.
11. EM Reagent, Brinkman Color Standard enzymes only, no instrument supplied. Company specializes in other lab. tests as well.
12. General Diagnostics Color/ Company has list of specialized enzymatic tests. Kits UV are not major item, but reputation is good.
13. P and L Biochemicals Color/ Standard enzyme tests available. Tests are good UV quality, complex to perform. Kits are excellent and
No. Name Type Comments/Cost
1. Technicon Flame Attachment for Auto- Filter For AutoAnalyzer attachment. Rapid changeover when Analyzer. equipmentis availablemakes it a consideration,but
not recommended for Level II laboratories.
2. Process and Instruments Very simple instrument,Na, K, Li, uses 1:100 dil. Internal standard technique,
usesair. $860
3. Process and Instruments F Upgraded quality instrument, as above, either internal or direct, good choice over 2. $1,220
4. National Instruments Laboratory F Na, K only, two models with standard readout and digital. Lack of Li is difficult,
either internal or direct standard, $700
usesair $2,125
5. McKee Pedersen F Na, K, Li uses internaland direct standards, with oxygen required. $1,609
6. London Company FLM-1 F Na, K only, uses air, internalstandard. $2,250
7. InstrumentalLab, Model 143 F Na, K, Li, uses air, internal standard
(good quality choice for lab.). $2,290
8. InstrumentalLab, Model 343 F Upgraded version of 7 above.
9. Beckman KliNa Flame System F Air, all three tests, new entry in market. $3,340
10. AdvancedInstruments F Na, K only, low cost, air instrument. $690
ANNEX Page 19
BASIC AUTOMATED LABORATORY (Level III)
1. Description: The basic automated laboratory is similar in terms of capabilities to the semiautomated laboratory of Level II. All of the tests , in this laboratory should be organized around a redundant back-up system
which provides test capabilities in the event that the automated equipment is lost. Many of the tests, particularly the low volume ones, will continue . to be performed manually as in Level II. Automated processors will be
in-troduced for the tests performed in the highest volumes, usually BUN and glucose. In hematology, addition of a blood processor such as the Coulter Fn (or upgrade of the basic instrument which might be purchased in Level II to RBC, WBC, HCT, MCV) can take care of automation at this level. Urine analysis is still done by dipstick; there is little to replace this basic procedure.
This type of laboratory is usually in the small hospital or the large clinic (10 or more physicians). Typical test loads range from 30 to 50 for the most common (hemaglobin, glucose, BUN) with smaller numbers, ranging down to one or two for some of the others (i.e., calcium). This laboratory may perform as many as 20 to 25 different determinations.
Personnel at this level must involve at least one person who acts as laboratory supervisor and coordinator. In the United States of America these are usually medical technologists with advanced training. Depending on the size of the hospital, the number of technicians may range from three to six or seven for 200 beds. For a clinic (not including bacteriology) of 20 physicians (no call or stat involved), a supervisor and three technicians would suffice.
Tests included near the upper extreme of Level III are all common chemistries - glucose, BUN, uric acid, cholesterol, total protein, albumin, SGOT, alkaline, phosphatus, LDH, bilirubin, 17-keto and 17-hydroxy steroids, Ns, K, C1, and others. At the lower end, some of the tests are not
avail-able. The number of tests on automated equipment depends on the volume of work in the laboratory.
Automated equipment for this laboratory is basically the addition of the single and dual channel autoanalyzers. These analyzers are added · to the equipment of the laboratory as workload warrants, usually being
as-signed to specific tests such as glucose or BUN. Operating in this way, the laboratory can upgrade itself to the maximum in Level III, performing . multiple tests, up to eight or ten, on single and dual channel systems.
The quality of results is not improved by automation. New problems of quality assurance must be defined and solved. The laboratory will find
that a large percentage of its time and effort must be devoted to this activity.
Maintenance of instruments is a key consideration. The instruments will have down time. The laboratory must be ready to cope with these
pro-blems, which involves technicians, equipment, and alternate tests.
3. Suggested Solutions for Laboratories within this Level: Personnel must be upgraded within this level of laboratory. A laboratory supervisor
must be clearly designated. The operation of the AutoAnalyzer requires careful attention_ If technician-level personnel are used, a supervising chemist or technologist must carefully review all work. Personnel require special training on these machines.
Quality of results entails an active program of quality assurance. Elements of this program include a careful check on the systems themselves and on the results. These are two distinct and separate elements. Most laboratories operate on the principle that if the machine "hangs together" and produces results, it is operational. The various parameters, such as bath temperature, flow pattern, response to unit concentration, carryover, and interaction, must be checked regularly in a quality assurance program. Further, checking must involve (on the part of the supervisor) assurance
that the regular maintenance program is carried out.
Quality of results also entails a program of controls and check samples. These should be run with all samples. Further, the technician must be instructed as to what the quality control activities are trying to
accomplish; the results must be reviewed with her, and, where necessary, corrective measures must be taken. At all levels, the technician must clearly understand that she is responsible for performing data analyses which make the "go or no go" decision on the results as they are produced.
ANNEX Page 21
3.1 For Progression to the Next Level (Multichannel Laboratory): The single/dual channel automated laboratory soon faces the question of pur-chase of a multichannel instrument to perform several tests requested on single samples. Purchase of a multichannel instrument moves the labora-tory into the next level. Progression should be based on a consideration of the number of multiple-test requests actually received. At the level ' of 30-40 multiple (panel) tests, such a consideration could become
practi-cal. At lower levels it is definitely counterindicated. For most labora-tories progression to a 12 or more channel instrument from Level III is not recommended. An intermediate instrument (SMA 6/60) may be a valuable choice. Before proceeding, the laboratory should consider the status of all other tests it is required to perform. In most cases, upgrading of enzymatic or electrolytic determinations may be the best course.
No. Name Type Comments/Cost
1. Technicon AutoAnalyzer I Continuous Most common clinical analyzer. Modular approach facilitating back-up equipment in laboratory. Effective rates 40-60 per hour,
totally automated from raw sample through analog readout. Simple to operate. Per channel (test) $5,000-7,000
Dual channel $9,000-10,000
2. Technicon AutoAnalyzer II Continuous Second generation of above, same principles of operation, using smaller amounts of sample and reagents° More readily upgraded to dual and triple channel operation. Same degree of automation and ease of operation. For channel (1) $ 8,000
(2) $ 10,500
(3) $ 13,000
3. Sanda, Inc. Continuous Italian-made version of this instrument is essentially similar to AutoAnalyzer. One channel $6,000
Dual channel $9,000-10,000
4. Spectronic (B and L) Discrete Using standard spectrophotometer, additional modules present automated processing from sampling to analog recorder or printer output. This item is an attempt to circumvent Technicon patents. Most applicable to enzymatic determinations. $6,000-8,000
5. Honeywell, Inc. Diclan 240 Discrete Suitable for UV-kinetics and chemical analyses. Rates to
240/hour claimed, includes sampling capabilities. $10,000-15,000
6. Joyce, Loebel, and Co. Discrete Colorimetric instrument, British-made.
7. LKB Reaction Rate Analyzer (8600) Discrete Has totally automated system, specifically for enzymes. Lab-oratory characteristics of instruments are good, including time and temperature control. $8,500.
0_ _o_
bo _-J bo _-.
No. Name Type Comments/Cost
8. Unicam AC Discrete Processor table-based on discrete samples in moving belt. An instrument of good quality, made in England. Main problem is lack of protein separation before analysis. $9,000
9. ClinoMak II Discrete Italian-made instrument using much the same principles as 8 above. Lacks temperature control and adequate sampling devices. High claimed rates are effectively less than lO0/hr. $10,000
10. Zymat *B and L Discrete Enzyme analyzer based on discrete samples and 340 readout. In-strument has digital printer and syringe-driven system.
$9,000-10,000
11. ABBOTT Model 100 Discrete Kinetic enzyme analyzer, 100 per hour, very small volumes re-quired, rapid changeover. Instrument is high quality, but costs
areexcessive. $20,000
12. Farrand Optical Co. Discrete Enzymatic kinetic system (UV), capable of long tests (30 minutes or more) at high rates. Instrument would best be suited to re-searchlaboratory. Est. $20,000
13. Digecon, Sherwood Discrete Semiautomated system, operated by technician. High precision in-strument. Suitable only for advanced laboratories or exotic tests where capabilities could be exploited. 30/hour. $20,000
14. Technicon AutoZyme Continuous Sample processing contains elements of discrete and continuous flow techniques. Measurement is pseudokinetic. May be major factor in futuremarkets. Est. $15,000
15. Beckman DSA Discrete Dual channel instrument with blanks. Micro samples capable of making filtrate (deproteinization). High quality, finds
appli-cation in situations requiring micro specimens. 40/hour, printer
available. $22,000
THE MULTICHANNEL LABORATORY (Level IV)
1. Description: This level of laboratory has at least one major piece of equipment with six or more channels performing tests on single specimens. No laboratory should consider purchase of a multichannel instrument unless it has capabilities in most or all of the tests at lower levels. This lab-oratory is typically in the larger hospitals where several tests are ordered on a single patient or where, in some cases, admission profiles are ordered
on many or all patients. The laboratory should anticipate a minimum of 20 profiles per day, and usually considerably more should be indicated. If this is not the case, emphasis on other alternate instruments should be con-sidered. These laboratories perform all of the tests of Level III, but in larger volume. Personnel should include one primary operator for the major instrument, as well as the usual number of technicians commensurate with the Level III workload. Other equipment should include most of that for Level III with a possible reduction in the number of channels of instrumentation (since it now plays a supporting role). In addition to the technician assigned to the major equipment and the laboratory supervisor, technicians are usually responsible for several tests, often on a rotational basis.
2. Problems: The major problem of this laboratory is to find a means by which to fully utilize the large investment in capital and personnel in the large equipment to fullest advantage. In most cases the benefits of the large instrument do not justify the expenditure required for its purchase.
The second problem lies in the area of quality of results produced by the multichannel analyzers. Alternatively, these machines are claimed to be screening instruments when they are in fact doing diagnostic work. Recognition of problems of quality of results on the large complex system
as well as development of adequate programs of control, including mainte-nance, remain major problems.
When facing problems of choice of instrument, the laboratory must decide which tests to include in the instrumental package, as well as which instrument to choose for its particular operation. Heretofore, this has been a problem of availability for the manufacturer. At this point in time,
several viable alternatives are available.
4
Maintenance of the instrument is a major consideration. With a 12-channel instrument, loss of 8.5% of the analytical instrument (one channel) results in the loss of 100% of the laboratoryVs capability on these 12 tests. Suitable alternative plans must be developed. With this large investment (capital as well as the laboratoryVs production facilities) in one system, maintenance must be at the highest level. Justification is often difficult.
The final problem centers on how to use the instrument in the labo-ratory. Its mission and its capabilities must be defined. Its
ANNEX Page 25
3. Su88ested Solutions for Laboratories within this Level: The large multichannel instrument is used for diagnostic work in most laboratories.
This should be the fundamental purpose of the laboratory. Purchase of an instrument for screening inmost cases is not a viable concept. Integra-tion into the diagnostic workload can greatly increase its test capacity. The most common single tests are routed to the single channel analyzers (glucose, BUN) and the panel instrument geared to handle the lower volume · tests heretofore requiring setting up of a separate analyzer. When
instr-uments are considered for the laboratory at Level III contemplating a move to Level IV, we recommend the purchase of a smaller instrument, i.e., the SMA 6/60 (flex) instead of the larger SMA 12/60 or the Hycel Mark X or XVII series. Ultimately, the laboratory with two of the smaller instruments has better back-up and capability than the one with a single large one. Like-wise, the smaller instruments better fit the program of development and
orderly progression we envision for the laboratory. In short, the labora-tory should look to keeping its highest volume tests on the single instru-ments, and combining some of the less frequent and more difficult for
testing on the multichannel instrument. The "freed" AutoAnalyzer channels can be used to back up the system in case of a complete failure; in the meantime they can be devoted to other tests not normally automated because of cost. The essential back-up instruments then serve a primary function in the laboratory as well.
Quality control programs for the multichannel instruments are just emerging from the developmental stage. In this respect, the Wisconsin (USA) program can be studied° The state or national agency must take the lead in helping laboratories in this respect. Two criteria are essential: (a) a source of referral information for operators, and (b) an outside quality assurance program. The very nature of standardization and control of these instruments leads to a tendency to feed data back into the system. There is no alternative to an outside agency providing help in this respect.
The tests to include in this instrumental package have been described in the first recommendation. The use of a smaller, six-channel instrument permits maximum flexibility in this respect and allows the laboratory to make the instrument conform to its real mission° For example, in a children's hospital where dehydration and malnutrition are recurrent problems, an elec-trolyte/total protein/albumin system would be most beneficial (Na, K, C1, CO 2, TP, albumin)° In a cardiac hospital an enzyme profile_ for example, would be most helpful (SGOT, SGPT, LDH, Alkaline, phosphatase, CPK, glucose). The laboratory must decide where its heaviest workload lies, and where panels of tests would do the most good.
parts. Further, a primary consideration in purchase of the instrument is the location of the nearest stock of complete parts for the system. The large instruments have lost modularity to a large extent. Consequently, availability of maintenance supplies and spare parts must be a key consid-eration. One of our major recommendations is in the area of national guide-lines requiring suppliers and/or manufacturers to stock parts in ready
accessto the instrumentsin the country.
Use of the instrument in the laboratory runs in direct contrast to usual ideas of utilization of equipment° The cost of operating an SMA in-strument (12 channels) is only 7.3 cents per minute. The consequence of this is that a laboratory invests a major share of its expense in bringing the instrument to operational status. Then it can economically process samples for single tests, even though it produces a panel of results° In order to recover the large investment of the laboratory in this equipment, it is essential that it carry a major share of the laboratory's work in running single tests, once the screening tests or real panel requests are out of the way. Reagents amount to only 2.05% of the costs of operating
a large multichannel instrument in the laboratory.
3.1. For Laboratories at Level IV Moving to Level V (The Screening Lab-oratory): The screening laboratory is a special operation. This is _ot a logical growth step and should not be contemplated, since the operation and organization of a screening laboratory is different in concept and mission. Screening tests on multichannel instruments, either as an
admis-sion profile or in response to a health need, particularly screening during off hospital hours, is an excellent and viable concept. See Level V
discussion.
4. Tabular Summary - Level IV Laboratories: At this level we are talk-ing of very large, very expensive equipment° Its value is derived from its ability to produce large numbers of tests while processing samples at con-ventional rates of 30 to 90 per hour. The numbers of channels range from 4 to 7 in hematology and from 6 to 24 in chemistry. Usually they have 6, 10, and 12 channels while contemplated instruments will have 17, 22, and 24
channels (Mark XVII, Coulter, and Technicon) o Costs range from $40,000 for the 6-channel instruments to $70,000 for 10 and 12 channels. The larger instruments will cost about $100,000 each. In hematology, costs are around $75,000 for the Technicon SMA 7Ao
ANNEX Page 27
An alternate path is a Mark X system, soon to be expanded to the XVII. There are significant numbers of U.S. laboratories with the latter system. In the author's opinion, the programmability of the instrument
(i.e., selecting one or 10 tests) is oversold, in view of the low costs of reagents. Where workloads are not large, the speed of the instrument is not a factor (40/hour), and allow its alternative approach to chemistry
(discrete) to play a significant factor. The conservation of sample is a · strong point in many cases. The dealer/maintenance support in the United
States is strong. Choice of this instrument for Central and South America would have to be contingent on development of field parts and representa-tives in these countries.
The remainder of the instruments discussed in Table IV are relatively new and require field evaluation before a recommendation can be made. We have made a specific recommendation to PAHO in this respect.
Hematology instruments are dominated by two systems in the field. The Technicon SMA 7 and SMA 4, performing four determinations and option-ally calculating three others on whole bloods (WBC, RBC, HCT, MCV). The Coulter S is quite different in concept and also has enjoyed good sales and acceptance in the United States of America. Both instruments perform well and could be considered if back up and maintenance were available. Their costs are approximately the same, about $75,000. There are no other comparable systems available on the market.
THE SCREENING LABORATORY (Level V)
1. Description: This is not an evolution from Level IV. It is a spe-cific laboratory emphasizing screening of large numbers of samples for
spe-cific parameters in the most economical way. This type of laboratory is often established in relation to national or state health programs for the purpose of detection of chronic diseases or health status evaluation. In
the United States of America there are state programs, national insurance-related programs, and military programs.
This laboratory is usually in a health laboratory or center, usually not in a hospital. The choice of location has several disadvantages in this respect. Personnel are often narrow in field but have high qualifications to operate these instruments, such as an SMA 12 system, for example. Back-up in this case is often for a single purpose, to check on performance and to replace single lost tests. Since screening is the major concern, the laboratory has little need for emergency type care or the rapid turn-around
required in the hospital laboratories.
2. Problems: The major problem is that these laboratories are often established by throwing a machine, technicians, and some supporting equip-ment into a room, expecting them to produce good data. This is essentially
a problem of personnel. Purchase of the equipment does not establish the program. Very careful planning is required in establishing a working, viable system.
Data handling is a major concern. The large numbers of tests often impede the efficiency of the laboratory. Data processing should be an in-tegral part of the planning.
Determination of back-up equipment is often neglected in the devel-opment of the program. Back-up functions have to be clearly defined in
the organization of the program.
3. Su88ested Solutions for Laboratories within this Level: Establishing or operating a laboratory for multiphasic screening requires detailed plan-ning. Personnel must be found and trained. The mission of the program
(not the laboratory) must be defined and the laboratory designed around this goal. In many cases the specimen handling system, particularly field collection and return of results, constitute a major portion of the program. In a similar program in Wisconsin, collection personnel outnumber labora-tory personnel three to one. Costs of collecting specimens exceed by 50% the costs of analyzing them.
ANNEX Page 29
equipped to process the data. Unless adequate provision, essentially a separate aspect of the program, is included in the planning and development, the effectiveness of the program will be severely limited as the data bottle-necks in the laboratory.
For the pure screening laboratory, operating at near capacity of one machine, back-up is a critical problem. In most cases, auxiliary methods ' such as are used in clinical laboratories are not practical. Where volumes
are very large, provision of a second major system duplicating the first is one alternative. A cooperative arrangement with local hospitals is a second. For the relatively small screening program, establishment of the program in
conjunction with a hospital using the instrumentation for diagnostic work on a fee-for-service basis is a very useful alternative. This approach may be very practical if the agency is considering programs of this type and wishes
a trial before a full-scale program is established.
Personnel to establish and run this laboratory are a major problem. In many cases, tying the screening laboratory to some ongoing concern such as a hospital can be to the significant benefit of both. For the hospital, the increased capacity of the multiphasic screening operation can provide services to their patients. For the screening program, it can draw on the personnel and back-up equipment, and also the knowledge and experience of the personnel in running the system. In the United States of America, a program was established in conjunction with the clinical laboratories of the state public health laboratory, which operates a full clinical chemis-try section in addition to the multiphasic screening program.
Quality control of these instruments presents unique problems. This was covered in Level IV. We are making a specific recommendation that some national programs, on a cooperative and assistance (not police) basis be
established to open lines of communication between operators with similar needs and problems.
No. Name Type Comment s/Cos t
1. Coulter S Hematology Performs four determinations- hemoglobin, hematocrit, red blood cell, and white blood cell counts - and
calculates three indices for a total of seven values. Totally automated instrument. Accepted in the field as standard. Requires skilled operator. Est. $70,000
2. Technicon SMA 7 Hematology Performs similar function, uses continuous flow principles· Makes four measurements and performs three calculations for total of seven tests. Fully automated, requires skilled operator. Est. $70,000
3. Technicon SMA 4 Hematology Same as above, skips the three calculated
para-meters. Est.$50,000
4. Hemolog D Hematology Performs differentialcounts, only system of its type on market. Introduced about one year ago, and not yet fully accepted. Should be considered developmental for at least two additional years.
Est. $74,000
5. Hycel Mark X Chemistry lO-channel discrete analyzer, programmable. Ana-lyzes 40 samples per hour, one to ten tests per sample. Readout on chart, printer available.
Est. $70,000
6. Hycel Mark XVII Chemistry Same as above, with additional test channels,
including electrolytes. Est. $92,000
7. Technicon SMA 6/60 Chemistry 60/hour, continuous analyzer. Six tests, four of which are electrolytes, two chemistry
determina-tions may be chosen. Est. $40,000
8. Technicon SMA 6/60 (Flex) Chemistry 60/hour, any six chemical determinations, output on analog graph paper or printed (costs extra). Blanks and protein free filtrate (dialysis) possible. Flexible, may be changed over to new tests. $40,000
No. Name Type Comments/Cost
9. Technicon SMA 12/60 Chemistry 60/hour, 12 determinations per sample. Can include four electrolytes or 12 chemistry tests. Other
specificationsas 8 above. $73,000
10. Technicon 12/60 micro Chemistry 30/hour, as 8 and 9 above, designed to use much smaller samples and run at slow rate for maximum color development. Pediatric work is its
forte. $77,150
11. Vickers 300 Chemistry Built in England. Claimed rates up to 300, with modular system built up of 20 channels, two per station. The 10-station system cost can be reduced by a lesser number of channels.
20 channel system $243,000
12. DuPont ACA Chemistry Up to 24 channelsat about 60 tests per hour. Emphasis is on totally closed processing and full automation. System eliminates operator
interven-tion. Strong points are constant readiness and wide variety of tests. Rented on per test basis.
Est. $70,000
13. Union Carbide Centrifichem Chemistry One of three systems using a principle of centri-fugal mixing of reagents and measurement. The
system is true micro in nature (10 to 20 microli-ters per test). Three very similar systems due to public domain patent. Est. $60,000-$80,000
14. Damon Engineering Chemistry Similar to above. $40,000-$50,000 15. Aminco Rotochem Chemistry Similar to above. $65,000
16. IL/Harleco Clinicard Chemistry Discrete analyzer uses punched card and internal computer to control steps of analysis, improving by control and cuing the precision of the human
17. American Monitor Corp. Chemistry Discrete analyzer capable of 1,040 tests per hour on multiple channels· Est. $35,000
18. General Science Corp. Hematology Built in England. Series of instruments of which the MK-3 does WBC, RBC, HCT and HGB on single sam-ple. The instrument is not well known in the USA and is just beginning to make its influence felt
on market. Est. $70,000-$80,000
19. AGA AutoChemist Chemistry Produced in Sweden, 24-channel discrete processor rated at 3,240 tests per hour. Instrument requires most advanced laboratories at very high workloads.
0nly successful installations in the USA have been 24-hour operations of large commercial labs. $485,000
bo
_'-F_
0Q