English/Portuguese
REPERCUSSIONS IN THE LIFE OF THE ELDERLY PERSON’S CAREGIVER: CASE
STUDY
REPERCUSSÕES NA VIDA DO CUIDADOR DOMICILIAR DO IDOSO: ESTUDO DE CASO
REPERCUSIONES EN LA VIDA DEL CUIDADOR FAMILIAR DEL ANCIANO: ESTUDIO DE CASOMaria da Conceição Coelho Brito1, Eliany Nazaré Oliveira2, Cibelly Aliny Siqueira Lima Freitas3, Adriana Gomes Nogueira Ferreira4, Maria Josefina da Silva5, Denise Lima Nogueira6
ABSTRACT
Objective: to identify, through the Systematization of Nursing Care, the way how the health profile of an elderly person reverberates in the life of the home caregiver. Method: this is a descriptive study, with a case study design and qualitative approach, supported on the theoretical framework of Orem’s Self-Care. This study was approved by the Research Ethics Committee of Universidade Estadual Vale do Acarau, under the CAAE 2534.0.000.039-10. Results: caring for the dependent elderly person reverberates in the caregiver’s life, generating some levels of stress, deficiencies in the caregiver’s self-care, and lack of performance of routine activities, since the caregiver attributed to himself the duty of caring for as a strategy to repay the
genitor for all the latter had already provided him with. Conclusion: strategies comprising the quality of life of the elderly persons’ caregiver are needed, since the Brazilian society, besides caring for those who are becoming elder, should pay attention to their caregivers before they become “hidden patients”. Descriptors: Dependent Elderly People; Care; Nursing.
RESUMO
Objetivo: identificar, por meio da Sistematização da Assistência de Enfermagem, como o perfil de saúde do idoso repercute na vida do cuidador domiciliar. Método: trata-se de estudo descritivo, com delineamento do tipo estudo de caso e abordagem qualitativa, apoiado no referencial teórico do Autocuidado de Orem. Este estudo foi aprovado pelo Comitê de Ética em Pesquisa da Universidade Estadual Vale do Acaraú, sob o CAAE n. 2534.0.000.039-10. Resultados:cuidar do idoso dependente repercute na vida do cuidador, gerando níveis de estresse, deficiências no autocuidado do cuidador, e não realização de atividades rotineiras, uma vez que o cuidador atribuiu a si o dever de cuidar como uma estratégia de retribuir ao genitor tudo o que este já havia oferecido a ele. Conclusão:são necessárias estratégias que vislumbrem a qualidade de vida do cuidador de idosos, uma vez que a sociedade brasileira, além de cuidar dos que envelhecem, deve prestar atenção aos
seus cuidadores antes que eles se tornem “pacientes ocultos”. Descritores:Idosos Dependentes; Assistência; Enfermagem.
RESUMEN
Objetivo: identificar, por medio de la Sistematización de la Atención de Enfermería, como el perfil de salud del anciano repercute en la vida del cuidador domiciliario. Métodos: esto es un estudio descriptivo, con diseño del tipo estudio de caso y abordaje cualitativo, respaldado por el referencial teórico del Autocuidado de Orem. Este estudio fue aprobado por el Comité de Ética en Investigación de la Universidade Estadual Vale do Acaraú, bajo el CAAE 2534.0.000.039-10. Resultados: cuidar del anciano dependiente repercute en la vida del cuidador, generando niveles de estrés, deficiencias en el autocuidado del cuidador, y no realización de actividades de rutina, ya que el cuidador atribuyó a sí mismo el deber de cuidar como una estrategia para retribuir al genitor todo lo que este le había ofrecido. Conclusión: son necesarias estrategias que contemplen la calidad de vida del cuidador de ancianos, ya que la sociedad brasileña, además de cuidar de aquellos que envejecen, debe prestar atención a sus cuidadores antes que estos se conviertan en “pacientes ocultos”. Descriptores: Ancianos Dependientes; Atención; Enfermería.
1Nurse, MS student, Federal University of Ceara/UFC. Fortaleza (CE), Brazil. Email: [email protected]; 2Nurse, PhD, Professor at the
Nursing Course of UVA. Sobral (CE), Brazil. Email: [email protected]; 3Nurse, PhD, Professor at the Nursing Course of UVA. Sobral (CE),
Brazil. Email: [email protected]; 4Nurse, PhD student, Federal University of Ceara/UFC. Fortaleza (CE), Brazil. Email:
[email protected]; 5Nurse, PhD degree, Professor at the Nursing Course of UFC. Fortaleza (CE), Brazil. Email:
Nurse. Student at the Specialization Course in Audit of Systems and Health Services at the Institute for Applied Theology (Inta). Service of Permanent Education of Santa Casa de Sobral. Sobral (CE), Brazil. Email: [email protected]
English/Portuguese
Brazil has experienced a process of demographic transition, mainly due to the progressive increase in the elderly population, causing a significant prevalence of illnesses and disabilities in the population, which brought the need for changes in the forms of care, and one of them was resuming the home
care model.1
As a result, there emerged, attached to the Portaria 1,395/1999, from the Brazilian Ministry of Health, the National Policy for the Health of the Elderly (PNSI), which grounds the Public Power actions in the health care sector with regard to the elderly population in Brazil, introduces family care and regards this model as being crucial for the health care provided to this population group, setting up the convergence of the three caring
dimensions.2 In this context, the home
caregiver is back as an important part of actions for the maintenance of autonomy, integration, and participation of the elderly person in society, besides being decisive for the success of public policies, since it lowers costs and improves the quality of life of
elderly people.1
Caring for the elderly person at home is an arduous task, since this care is generally
attributed to a person who doesn’t have only
this activity and she/he ends up combining it with other tasks, such as taking care of children and home, besides a professional activity. This accumulation of activities results in exhaustion, something which leads the home caregiver to illness. Thus, home care is characterized by its repetitive and unceasing, with the possibility of causing an
overload of tasks and the caregiver’s affective
and social isolation.3
Then, the Family Health Strategy (FHS) emerges. Created in 1994, FHS has played a strategic role for the consolidation of the Unified Health System (SUS), favoring equity and universality through innovative actions in the sector. For this, one uses home visit as an interaction technology of health care, constituting a basic intervention tool adopted by the FHS teams to get into and know the
population’s life reality, in order to favor the establishment of ties with it, and the understanding of relevant aspects in the
family relations dynamics4, improving the
ability to provide the elderly person with an effective care.
To achieve this purpose, nurses employ the Systematization of Nursing Care (SNC), an
important resource for applying and
demonstrating the scientific, technical, and
human kinds of knowledge in the client’s
care, besides characterizing the professional
practice.5 Thus, one aims to identify, through
SNC, the way how the health profile of an
elderly person reverberates in the life of the home caregiver.
This is a descriptive study, with a case
study design and a qualitative approach,
supported on the framework of Orem’s Self
-Care Theory, carried out from March to June 2010, through 9 home visits to 1 elderly
person’s home caregiver. Data collection was
undertaken through a form addressing aspects such as the sociodemographic profile, lifestyle, and daily life activities using the
Barthel’s scale, access to health services,
medicines currently used, and
hospitalizations, besides the questionnaire SF-36, an instrument for assessing quality of life.
A genogram and an eco-map were
constructed, which are rich information sources for planning strategies in the family.
One designed a care plan, whose implementation was undertaken through SNC. The information analysis was conducted by means of the descriptive technique.
The study was approved by the Research Ethics Committee of Universidade Estadual Vale do Acarau (UVA), under the CAAE 2534.0.000.039-10 and the Protocol 817/2009.
● Knowing the health profile of the
elderly
person
This is a male elderly person, 86 years old and dependent for 8 years, due to a
cerebrovascular accident (CVA), which
manifested itself in 5 episodes, and the last one occurred 2 years ago, leading him to a total dependence degree, according to the
Barthel’s scale, with frequent demand for
health services.
One estimates that about 40% to 50% of individuals who suffer a CVA die after 6 months. In turn, survivors present neurological
deficits and significant residual disabilities6;
it’s in this context that the family caregiver
emerges. The dependent elderly person
reverberates in the caregiver and his family’s
life dynamics, since the tasks assigned to him, often without proper guidance, support from health institutions, a fact with reflects on the
caregiver’s quality of life. The activity of
caring for an elderly relative who is ill and dependent at home takes place in space
RESULTS AND DISCUSSION
METHOD
English/Portuguese
where a significant part of life is lived, in which knowledge and memory regarding facts and intimate relationships are important both for the caregiver and the individual who is
being cared for7, governed by subjective and
affective relations, named family
relationships.
● Understanding family and the intra and
extra-family relationships
In the geriatrics and gerontology field, by regarding family as a system, that is, as a unit
in which it’s possible to view the interaction
between its members, the presence of an elderly person who depends on care affects all components in the group, in varied degrees.
Thus, it’s important that health professionals
have an assessment tool which takes into account structure, development over time, and family functioning, by proposing care actions for this elderly person, in order to help understanding family as a care unit, instead of a mere sum of the individualities of
all family members in many contexts.8
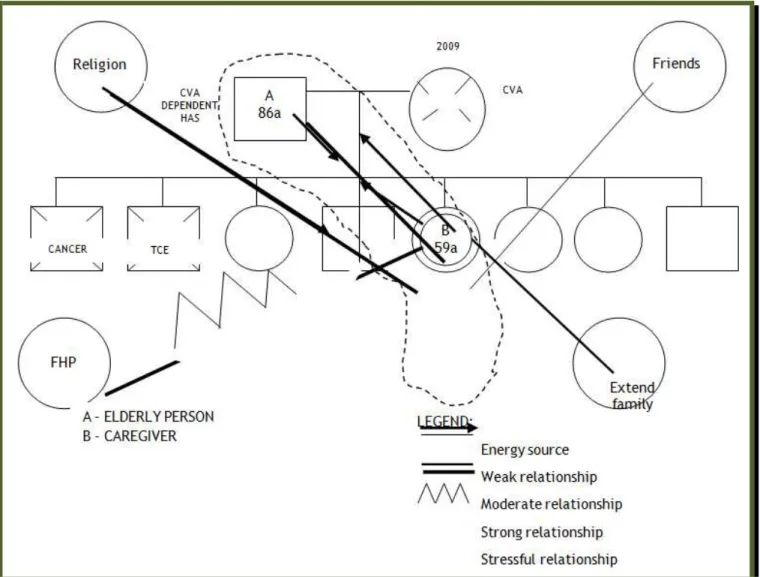
In Figure 1, the index-user is indicated as
“B” and he maintains a strong relationship with his father, being his caregiver, an aspect
requiring effort and time. Due to his genitor’s dependence, “B” has a stressful relationship
with the FHS, because of the precarious assistance provided by it. The caregiver has few support sources in society.
Figure 1. Genogram and an eco-map of the study family.
He also presents a moderate relationship with the other family members. His mother died recently, increasing his burden as caregiver and head of an unstructured family
due to the illness. There’s a strong
relationship between the index-subject and religion, too.
Knowing the family structure, its
composition, the way how members organize themselves and interact with each other and with the environment, the health problems, the risk situations, the vulnerability patterns is something crucial for the planning of family
health care.8
The intervention of health services along with this caregiver requires a greater effort,
since there’re few support sources in the
community, an aspect which may adversely
interfere with the user’s life dynamics and in
his health-illness process. It’s worth
highlighting that only the genitor and his daughter who cares for him at home are there. This is due to the new chain of issues and demographic changes, where the family
structure changes, going from the
predominance of multiple and extended families to families which tend to consist of a
English/Portuguese
It’s essential to establish care strategies fostering the promotion of caregivers’ health
and quality of life, aspects which may be better worked out when nurses use a care method directing its practices, SNC.
● Systematizing car
e for the caregiver
according to Orem’s Theory
This is a female caregiver client, 50 years old, single, with no occupation and complete high school, catholic. For 3 years, provides integral care for her genitor, the reason why she no longer performs her routine activities, quit her job and ended a love relationship.
She has 8 brothers, who don’t help to provide
care. She has no leisure activities. She feels depressed, has no mood to perform basic
activities, doesn’t eat or sleep well, live
under constant stress; she doesn’t perform
physical activities neither seeks health services. On physical examination, the following changes were found: low back pain, and neglect of physical appearance. Blood pressure: 120 x 80 mmHg; temperature: 36.7ºC; breathing: 18 rpm; and pulse: 86 bpm.
Orem’s Self-Care Theory comprises three
requirements: universal, developmental, and health deviation. The universal requirements relate to the quest for sustaining life, the
structure and functioning of the human body; the developmental ones are those which offer the needed conditions for changes occurring
throughout the life cycles, allowing
adaptations for the individual’s development;
in turn, health deviations are the self-care needs manifested in the presence of illness,
disabilities, and treatments for the
individual’s recovery.10
One designed a nursing care plan, as shown in Figure 2, displaying a predominance of actions aimed at the support-education system, where the individual has skills for
performing the therapeutic self-care, he’s
able to learn putting it into practice, but he needs professional support. In this case, nurse will be responsible for his training to be the agent of his own self-care, since the nursing process, as proposed by Orem, is a method seeking to determine the self-care deficits, as well as the role that the nurse (or person) will play to meet the requirements needed for a
satisfactory self-care.10
Nursing diagnoses Nursing prescriptions
Performance of a modified role, related to an ineffective support, as evidenced by caregiver’s overload.
- Listen actively;
- Express one’s own thoughts and feelings;
- Encourage self-care activities. Acute pain, related to back pain, evidenced by his
description.
- Evaluate signs and symptoms of pain;
- Provide information to help increasing pain tolerance.
Impaired social interaction, related to caregiver’s overload,
as evidenced by isolation.
- Plan along with relatives a schedule of care actions for the elderly person.
Leisure deficit, related to caregiver’s overload, as evidenced by discouragement.
- Try performing pleasurable activities;
- Modify the environment and the family relationships experienced.
Impaired home maintenance, related to inadequate support system, as evidenced by the requirement of the caregiver role.
- Explore available alternatives for a rearrangement of roles.
Disturbed nutrition, less than body demands, related to
caregiver’s overload, as evidenced by poor food intake.
- Encourage regular feeding habits;
- Diet diversification, and at appropriate intervals.
Disturbed sleep patterns, related to caregiver’s overload,
as evidenced by insomnia.
- Use strategies which optimize sleep patterns;
- Plan along with relatives the care for the elderly person, in order to offer uninterrupted sleeping hours.
Loneliness risk, related to social isolation. - Plan along with relatives the care for the elderly person, in order to offer hours for extra-family relationships.
Figure 2. Nursing diagnoses and prescriptions.
However, the care plan proposed to the
caregiver wasn’t successful, because there
was no family support. The caregiver participating in this study lives with the genitor and has only sporadic visits from other relatives, thus, the care for the elderly person is under his responsibility, preventing the implementation of the proposed self-care
strategies. Here, one emphasizes the State’s
role in the care for the elderly person at home, since, even returning to the family environment, this must offer a support for the
caregiver, otherwise, it’ll promote new
pathways for illness. Thus, there’s a need to
be alert in order to recognize the caregiver as
a “hidden patient”, who lacks appropriate
interventions.11
● Implications for nursing
English/Portuguese
all he had already offered him. This becomes so ingrained that prevents the caregiver from having a different look without experiencing a guilt feeling. In this conflict, thus, nursing needs to operationalize and optimize care for
the elderly person, as well as the caregiver’s
quality of life, in order to allow the participation of the elderly subject, and his family caregiver, in the care process, potentiating a qualified care.
It’s worth implementing health actions
aimed at the biological, psychological, social, and spiritual needs of the caregiver of a totally dependent individual on their roles, since the overload of care actions negatively
affects his life in society.12 One also highlights
that caregivers need a support with regard to training and education, as well as rest and physical and mental health, so that programs and policies provide them with coping strategies to face specific stressful situations
and negative consequences, too.13
The study had as its object to identify, through SNC, based on the concepts proposed
by Orem’s Self-Care Theory and the support
systems surrounding the caregiver, the way
how the health profile of an elderly person reverberates in the life of the home caregiver. It became evident, thus, that one of the
effects on the caregiver’s life is the
deprivation of his self-care. So, there’s a need
for implementing strategies which envisage
the quality of life of the elderly person’s
caregivers, since the Brazilian society is aging and it lacks more support for aging with quality, besides providing those who care for with a better care.
This study shows that there’s a need for
public policies aimed at the elderly person’s
caregivers, in order to promote a better quality of life, and further researches involving the caregiver in his various facets are also needed, incorporating aspects from his training to his professional practice, so
that he’s able to intervene in the most
coherent way with regard to the reality of caregivers and elderly people.
1. Resende MCF, Dias EC. Cuidadores de idosos: um novo/velho trabalho. Physis [Internet]. 2008 [cited 2010 Apr 25];
18(4):[about 7 p.]. Available from:
http://www.scielo.br/scielo.php?script=sci_ar ttext&pid=S0103-73312008000400010.
2. Ministério da Saúde (Brasil), Secretaria de Atenção à Saúde. Portaria nº 2.528, de
outubro de 2006 [internet]. Política Nacional de Saúde da Pessoa Idosa. Brasília: Ministério da Saúde; 2006 [cited 201º Apr 30]. Available from:
http://portal.saude.gov.br/portal/arquivos/p df/2528%20aprova%20a%20politica%20nacional %20de%20saude%20da%20pessoa%20idosa.pdf. 3. Schossler T, Crossetti MG. Cuidador domiciliar do idoso e o cuidado de si: uma análise através da teoria do cuidado humano de Jean Watson. Texto & contexto enferm [Internet]. 2008 apr/june [cited 2010 Apr 25];17(2):[about 7 p.]. Available from: http://www.scielo.br/pdf/tce/v17n2/09.pdf. 4. Martins JJ, Albuquerque GL, Nascimento ERP, Barra DCC, Souza WGA, Pacheco WNS. Necessidades de educação em saúde dos cuidadores de pessoas idosas no domicílio. Texto & contexto enferm [Internet] 2007 apr/june [cited 2010 Apr 27]; 16(2):[about 8
p.]. Available from:
http://www.scielo.br/scielo.php?script=sci_ar
ttext&pid=S0104-07072007000200007&lng=en&nrm=iso&tlng=pt .
5. Pereira APS, Teixeira GM, Bressan CAB, Martini JG. O genograma e o ecomapa no cuidado de enfermagem em saúde da família. Rev bras enferm [Internet]. 2009 may/june [cited 2010 Mar 25]; 62(3):[about 9 p.].
Available from:
http://www.scielo.br/scielo.php?pid=S0034-71672009000300012&script=sci_arttext.
6. Teixeira CP, Silva LD. As incapacidades físicas de pacientes com acidente vascular cerebral: ações de enfermagem. Enferm Glob [Internet]. 2009 feb [cited 2010 Apr 26];15
[about 7 p.]. Available from:
http://scielo.isciii.es/scielo.php?script=sci_ar
ttext&pid=S1695-61412009000100019&lng=pt&nrm=iso&tlng=pt. 7. Amendola F, Oliveira MAC, Alvarenga MRM. Qualidade de vida dos cuidadores de pacientes de dependentes no programa saúde da família. Texto & context enferm [Internet]. 2008 apr/june [cited 2010 June 06];17(2).
Available from:
http://www.scielo.br/scielo.php?script=sci_ar
ttext&pid=S0104-07072008000200007&lng=en&nrm=iso&tlng=pt .
8. Silva L, Bousso RS, Galera SAF. Aplicação do modelo calgary para avaliação de famílias de idosos na prática clínica. Rev bras enferm [Internet]. 2009 july/aug [cited 2010 Apr 25]; 62(4): [about 10 p.]. Available from: http://www.scielo.br/scielo.php?script=sci_ar ttext&pid=S0034-71672009000400006.
English/Portuguese
9. Manzini FC, Simonetti JP. Consulta de enfermagem aplicada a clientes portadores de hipertensão arterial: uso da teoria do autocuidado de Orem. Rev latinoam enferm [Internet]. 2009 jan/feb [cited 2010 June 06];17(1):[about 10 p.]. Available from: http://www.scielo.br/scielo.php?script=sci_ar
ttext&pid=S0104-11692009000100018&lng=en&nrm=iso&tlng=pt .
10. Feijão AR, Lopes MVO, Galvão MTG.
Importance of the Supportive-educative
System of Orem Model in the patient
compliance – Reflexive study. Online braz j
nurs [Internet]. 2009 nov 18; [Cited 2010 Dec
17];8(2). Available from:
http://www.objnursing.uff.br/index.php/nurs ing/article/view/j.1676-4285.2009.2213/490. 11. Figueiredo D, Lima MP, Sousa L. Os
“pacientes esquecidos”: satisfação com a vida
e percepção de saúde em cuidadores familiares de idosos. Rev kairós [Internet]. 2009 Jan [cited 2010 Apr 25]; 12(1):[about 16
p.]. Available from:
http://revistas.pucsp.br/index.php/kairos/art icle/viewFile/2782/1817.
12. Nogueira DL, Oliveira EN, Brito MCC, Borges VS, Vasconcelos DP, Pinto PD. Processo de enfermagem: uma ferramenta para o cuidado ao idoso com Alzheimer. Rev enferm UFPE on line [Internet]. 2011 aug [cited 2012 June 19];5(6):[about 7 p.]. Available from: http://www.ufpe.br/revistaenfermagem/inde x.php/revista/article/view/1666/pdf_600 13. Robison J, Fortinsky R, Kleppinger A, Shugrue N, Porter M. A broader view of family caregiving: effects of caregiving and caregiver conditions on depressive symptoms, health, work, and social isolation. J Gerontol B Psychol Sci Soc Sci [Internet]. 2009 Nov [cited 2012 June 19]; 64(6): [about 10 p.]. Available from:
http://psychsocgerontology.oxfordjournals.or g/content/64B/6/788.short
Submission: 2012/08/22 Accepted: 2013/01/15 Publishing: 2013/02/01
Corresponding Address
Maria da Conceição Coelho Brito
Rua Cel. Henrique Rodrigues, 164 / Ap. 201 Bairro Campo dos Velhos